Serotonin transporter binding after recovery from eating disorders ORIGINAL INVESTIGATION
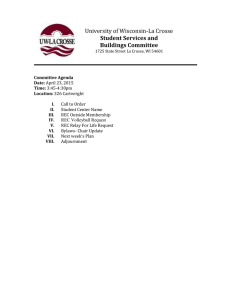
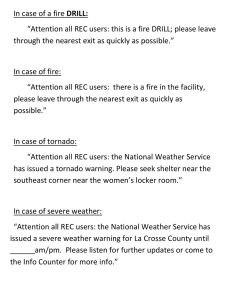
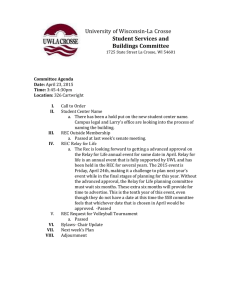
advertisement

Psychopharmacology DOI 10.1007/s00213-007-0896-7 ORIGINAL INVESTIGATION Serotonin transporter binding after recovery from eating disorders Ursula F. Bailer & Guido K. Frank & Shannan E. Henry & Julie C. Price & Carolyn C. Meltzer & Carl Becker & Scott K. Ziolko & Chester A. Mathis & Angela Wagner & Nicole C. Barbarich-Marsteller & Karen Putnam & Walter H. Kaye Received: 29 March 2007 / Accepted: 5 July 2007 # Springer-Verlag 2007 Abstract Rationale Several lines of evidence suggest that altered serotonin (5-HT) function persists after recovery from anorexia nervosa (AN) and bulimia nervosa (BN). Objectives We compared 11 subjects who recovered (>1 year normal weight, regular menstrual cycles, no bingeing or purging) from restricting-type AN (REC RAN), 7 who recovered from bulimia-type AN (REC BAN), 9 who Parts of the manuscript were presented at the 44th American College of Neuropsychopharmacology (ACNP) Annual Meeting, December 11–15, 2005, Waikoloa, Hawaii. U. F. Bailer : G. K. Frank : S. E. Henry : C. C. Meltzer : A. Wagner : W. H. Kaye (*) Western Psychiatric Institute and Clinic, University of Pittsburgh, Iroquois Building, Suite 600, 3811 O’Hara Street, Pittsburgh, PA 15213, USA e-mail: kayewh@upmc.edu W. H. Kaye Psychiatry, University of California San Diego, 8950 Villa La Jolla Drive, Suite C207, La Jolla, CA 92037, USA U. F. Bailer Department of Biological Psychiatry, University Hospital of Psychiatry, Medical University of Vienna, Vienna, Austria J. C. Price : C. C. Meltzer : C. Becker : S. K. Ziolko : C. A. Mathis Department of Radiology, Presbyterian University Hospital, School of Medicine, University of Pittsburgh, Pittsburgh, PA, USA C. C. Meltzer Departments of Radiology and Neurology, Emory School of Medicine, Atlanta, GA, USA recovered from BN (REC BN), and 10 healthy control women (CW). Materials and methods Positron emission tomography (PET) imaging with [11C]McN5652 was used to assess the 5-HT transporter (5-HTT). For [11C]McN5652, distribution volume (DV) values were determined using a twocompartment, three-parameter tracer kinetic model, and specific binding was assessed using the binding potential (BP, BP=DVregion of interest/DVcerebellum −1). Results After correction for multiple comparisons, the four groups showed significant (p<0.05) differences for [11C] C. C. Meltzer : W. H. Kaye School of Medicine, University of Pittsburgh, Pittsburgh, PA, USA G. K. Frank Laboratory for Developmental Brain Research, University of Colorado at Denver and Health Sciences Center, The Children’s Hospital, 1056 E. 19th Avenue, Denver, CO 80218, USA A. Wagner Department of Child and Adolescent Psychiatry, J.W. Goethe University of Frankfurt/Main, Frankfurt/Main, Germany N. C. Barbarich-Marsteller New York State Psychiatric Institute, Department of Psychiatry, College of Physicians and Surgeons, Columbia University Medical Center, New York, NY, USA K. Putnam Department of Environmental Health, Division of Epidemiology and Biostatistics, University of Cincinnati School of Medicine, Cincinnati, OH, USA Psychopharmacology McN5652 BP values for the dorsal raphe and antero-ventral striatum (AVS). Post-hoc analysis revealed that REC RAN had significantly increased [11C]McN5652 BP compared to REC BAN in these regions. Conclusions Divergent 5-HTT activity in subtypes of eating disorder subjects may provide important insights as to why these groups have differences in affective regulation and impulse control. Keywords Anorexia nervosa . Bulimia nervosa . Serotonin transporter . Positron emission tomography . Serotonin . 5-HTTLPR Introduction Anorexia nervosa (AN) and bulimia nervosa (BN) are disorders of unknown etiology that most commonly have their onset during adolescence in females. These disorders are characterized by the relentless pursuit of thinness, obsessive fears of being fat, and aberrant eating behaviors, such as restrictive eating and episodes of purging and/or binge eating (American Psychiatric Association 1994). Physiologic and pharmacologic studies show that disturbances of serotonin (5-HT) activity occur in people who are ill with eating disorders (EDs; Brewerton and Jimerson 1996; Walsh and Devlin 1998; Wolfe et al. 1997). Such 5HT disturbances may contribute to appetite dysregulation (Blundell 1984; Leibowitz and Shor-Posner 1986), anxious and obsessional behaviors and extremes of impulse control (Cloninger 1987; Higley and Linnoila 1997; Lucki 1998; Mann 1999; Soubrie 1986). Importantly, disturbances in 5HT measures appear to persist after individuals recover from AN and BN. It has been demonstrated that individuals who recovered from AN and BN have elevated cerebrospinal fluid (CSF) concentrations of 5-hydroxyindoleacetic acid (5-HIAA; Kaye et al. 1991a), reduced 5-HT2A receptor levels (Bailer et al. 2004; Frank et al. 2002; Kaye et al. 2001a), and increased 5-HT1A receptor levels (Bailer et al. 2005). Moreover, those recovered from AN and BN show altered behavioral responses to 5-HT challenges (Frank et al. 2001; Kaye et al. 2003; Smith et al. 1999; Ward et al. 1998). Recent imaging studies, using single photon emission computed tomography (SPECT) with [123I]betaCIT found reduced 5-HTT binding in people who are ill with bulimic-type EDs (Kuikka et al. 2001; Tauscher et al. 2001). Steiger found that individuals who recovered from BN had reduced platelet binding of paroxetine (Steiger et al. 2005b); however, recent studies have shown that peripheral measures of 5-HT receptor levels (5-HT2A and 5HTT) do not correlate with central measures in healthy controls. (Cho et al. 1999; Uebelhack et al. 2006; Yatham et al. 2000). To date, no studies have explored whether central 5-HTT abnormalities continue after individuals with EDs have recovered. The aim of this study was to use positron emission tomography (PET) imaging with [11C]McN5652 to determine if alterations of 5-HTT persist after recovery from AN and BN. Persistence of these abnormalities into recovery may indicate a “trait” phenomenon, possibly linked to the pathogenesis of the illness. In contrast, normalization of the 5-HTT alterations upon recovery would suggest a “state” phenomenon. The boundaries between subtypes of eating disorders are poorly understood and somewhat controversial. Reasons for subdividing recovered restricting-type anorexia nervosa (REC RAN) and recovered bulimia-type anorexia nervosa (REC BAN) is that they have differences in affective modulation and perhaps response to selective serotonin reuptake inhibitor (SSRI) medication. In addition, other studies from our group show that they are different in terms of binding of the 5-HT1A receptor (Bailer et al. 2005). Finally, this is reasonably consistent with the Diagnostic and Statistical Manual of Mental Disorders (DSM IV; American Psychiatric Association 1994) practice of categorizing subgroups as AN, AN-BN, and BN. A secondary, exploratory aim of this study was to examine the possible effects of the functional polymorphism in the promoter region of the 5-HTT gene (5HTTLPR) on in vivo expression of 5-HTT in healthy women and those who recovered from EDs. Some, but not all, genetic studies find altered frequency of a short allele polymorphism in the 5-HTTLPR in people with AN and BN (Di Bella et al. 2000; Gorwood 2004; Lauzurica et al. 2003; Matsushita et al. 2004; Monteleone et al. 2005; Steiger et al. 2005a). The correlation of genotypes with imaging findings can be problematic, given the fact that the sample size is small. Thus, we report exploratory findings. Materials and methods Twenty-seven women who recovered from EDs [7 women recovered from bulimic-type anorexia nervosa (REC BAN), 11 women who recovered from restricting-type anorexia nervosa (REC RAN), 9 women who recovered from bulimia nervosa (REC BN)] were recruited as previously described (Bailer et al. 2005; Wagner et al. 2006) All individuals underwent four levels of screening: (1) a brief phone screening, (2) an intensive screening assessing psychiatric history, lifetime weight, binge eating and methods of weight loss/control, and menstrual cycle history as well as eating pattern for the past 12 months, (3) a comprehensive assessment using structured and semistructured psychiatric interviews conducted by phone or in person, and (4) a face- to-face interview and physical Psychopharmacology examination with a psychiatrist. To be considered “recovered,” subjects had to (1) maintain a weight above 85% average body weight (Company 1959), (2) have regular menstrual cycles, and (3) have not binged, purged, or engaged in significant restrictive eating patterns for at least 1 year before the study. Restrictive eating pattern was defined as regularly occurring behaviors, such as restricting food intake, restricting high-caloric food, counting calories, and dieting. Additionally, subjects must not have used psychoactive medication such as antidepressants or met criteria for alcohol or drug abuse or dependence, major depressive disorder, or severe anxiety disorder within 3 months of the study. Ten healthy control women (CW) were recruited through local advertisements and had no history of an ED, psychiatric or neurologic disorder, or serious medical illness. This study was conducted according to the institutional review board regulations of the University of Pittsburgh, and all subjects gave written informed consent. Blood was drawn for assessment of β-hydroxybutyrate (BHBA), a plasma ketone body that is relatively sensitive to reflecting the presence of starvation (Fichter et al. 1990), as well as for evaluation of gonadal hormone levels (estradiol, E2). The Structured Clinical Interview for DSM-IV Axis I Disorders (First et al. 1996) was used to assess the lifetime prevalence of Axis I psychiatric disorders. The ED diagnosis was made by a modified version of module H of the SCID I. Current psychopathology was assessed with a battery of standardized instruments including the Beck Depression Inventory (BDI; Beck et al. 1961), the Spielberger–Trait Anxiety Inventory (STAI; Spielberger et al. 1970), the Frost Multidimensional Perfectionism Scale (MPS; Frost et al. 1990), the Eating Disorders Inventory (EDI-2; Garner 1990)), the Yale– Brown Obsessive Compulsive Scale (Y-BOCS; Goodman et al. 1989a,b), the Yale–Brown–Cornell Eating Disorder Scale (YBC-EDS; Mazure et al. 1994; Sunday et al. 1995), the Barratt Impulsiveness Scale (BIS; Barratt and Patton 1983), and the Temperament and Character Inventory (TCI; Cloninger et al. 1994) for assessment of harm avoidance, novelty seeking, and reward dependence. All subjects were scanned on the ECAT HR+PET scanner (CTI PET systems, Knoxville, TN) in threedimensional (3D) imaging mode during the first 10 days of the follicular phase of the menstrual cycle. Details of PET and magnetic resonance imaging (MRI) acquisition and co-registration are described elsewhere (Lopresti et al. 2001). Immediately after slow bolus intravenous injection of 13.8±1.8 mCi [11C]McN5652, dynamic emission scanning with arterial blood sampling (input function) was performed over 90 min. A scanning time of 90 min was used to achieve time stable measurements of distribution volume (DV) across regions for [11C]McN5652 (Frankle et al. 2004). The following regions of interest (ROI) were hand drawn on the coregistered MR images by technicians blind to subject diagnosis and applied to the dynamic PET data to generate time–activity curves: subgenual cingulate, thalamus, antero-ventral striatum, dorsal caudate, and cerebellum (as a reference region; Bailer et al. 2005; Drevets et al. 2001; Frank et al. 2005). For the dorsal raphe nucleus, due to the lack of identifiable anatomic boundaries on the MR, the ROI was placed directly on the PET image in the following manner. Based on the coregistered MRs, the brain stem was subdivided into a rostral (midbrain/upper pons) and caudal region (medulla/ pons) to approximate the dorsal and median raphe nuclei, respectively. A dorsal midbrain raphe nucleus was drawn on the dynamic PET image, using circular fixed 6 mm radius ROIs placed over the area of highest radioactivity. The dorsal raphe was drawn over three contiguous planes, and the data from those three planes were sampled. The inferior border of the dorsal raphe nucleus was identified by the interpeduncular cistern on the MR. Previous imaging studies of our group in EDs (Bailer et al. 2004, 2005, 2007; Frank et al. 2005) have found alterations in these ROIs and therefore guided our choice of brain regions to investigate in our subjects in this study. Figure 1 shows examples of MR and PET image data acquired at the level of the dorsal raphe. For the kinetic analyses, regional [11C]McN5652 DV values were determined using a two-compartment, threeparameter tracer kinetic model (Lopresti et al. 2001). Specific 5-HTT binding was assessed using binding potential (BP), where BP was derived as the difference between the ROI DV value and the cerebellar DV value, normalized to the cerebellar DV [BP=(DVROI −DVCER)/ DVCER] (Parsey et al. 2000). An MR-based partial volume effect correction method was applied to correct the PET data for the dilutional effect of expanded CSF spaces accompanying normal aging and disease-related cerebral atrophy (Meltzer et al. 1996, 1999). For the genotyping data, S and L alleles were determined using DNA amplification (polymerase chain reaction, PCR) and established flanking primers. Amplification products were resolved by electrophoresis and visualized with ethidium bromide staining and UV transillumination, according to Edenberg and Reynolds (1998). Genotyping was performed blind to diagnosis and imaging results. Global BP differences were estimated by multivariate analysis of variance (MANOVA) to explore if mean differences among the three ED groups and controls were likely to occur by chance. A new linear combination consisting of all the dependent ROI’s variables (subgenual cingulate, antero-ventral striatum, thalamus, dorsal caudate, and dorsal raphe) controlled the experiment-wise error rate before evaluating specific regions and allowed overall assessment of global BP patterns. Multiple comparisons Psychopharmacology Fig. 1 This figure is representative of a recovered anorexic women, restricting type (REC RAN). The image is an SUV normalization of a late sum (30 to 90 min) [ 11 C] McN5652 positron emission tomography (PET) scan (left) and the subject’s associated coregistered SPGR magnetic resonance (MR) image (right). The SUV image was created from the late sum by division (of each pixel) by the subject’s injected dose in mCi and multiplying by the subject’s weight in kg. Also shown are examples of the regions-of-interest that were used to generate the PET time-activity data. DRP Dorsal raphe nucleus; CER cerebellum using the Tukey–Kramer method identified the significant group pairs for statistically significant ANOVAs. Correlations were examined with Pearson correlation coefficients. A repeated measures analysis of variance (ANOVAR) was applied to examine potential group differences in radiolabeled metabolites of [11C]McN5652. Values are expressed as mean±standard deviation (SD). Standard statistical software packages (SAS Version 9.1) were used. time course (data not shown). The regional [11C]McN5652 BP values followed the rank order of 5-HTT binding (Parsey et al. 2000) as shown in Table 2. MANOVA results for global BP differences were significant at the 5% level. Follow-up univariate ANOVA significantly distinguished the groups apart for [11C] McN5652 BP values in the regions of antero-ventral striatum (F3,35 =5.19, p=0.004) and dorsal raphe (F3,35 = 4.64, p=0.008; Table 2). Post-hoc analysis revealed that the REC RAN had significantly increased [11C]McN5652 BP compared to REC BAN in these regions. REC BAN had significantly lower [11C]McN5652 BP in the antero-ventral striatum compared to REC BN. Illustrative scatterplots for the dorsal raphe and antero-ventral striatum are shown in Fig. 2. [11C]McN5652 BP was not related to lifetime history of major depressive disorder (n=16; 5 REC RAN, 4 REC BAN, and 7 REC BN), obsessive–compulsive disorder (n= 18), alcohol abuse (n=3) or alcohol dependence (n=1), any anxiety disorder (n=11), use of birth control pills (n=14), levels of plasma β-hydroxybuteric acid (BHBA), length of recovery, age, or current or low body mass index (BMI) in REC ED (all REC subgroups together) subjects. There was no relationship between [11C]McN5652 BP and measures of anxiety, depression, obsessionality, or impulse control at the time of the study. Genotyping data were available in 24 REC ED subjects and 10 CW. ED subjects showed allele frequencies of 58% for the L and 42% for the S allele and a genotype distribution of 29.2% LL (n=7), 58.3% SL (n=14), and 12.5% SS (n=3). CW had frequencies of 60% for the L and 40% for the S allele and genotype frequencies of 40% LL (n=4), 40% SL (n=4) and 20% SS (n=2). This small number of subjects showed no significant differences in allele or genotype frequencies between REC ED and CW. Because of the small sample, all subjects were considered together (REC ED and CW) when compared to [11C] McN5652 BP. The subjects with SS alleles had lower [11C] McN5652 BP than subjects with LL alleles for the dorsal caudate (SS, 0.43±0.06; LL, 0.60±0.12; p=0.01), but not other brain regions (Fig. 3). Findings were similar for the dorsal caudate when only the REC ED subjects were considered (SS, 0.44±0.08; LL, 0.63±0.09; p=0.03). Discussion Results Demographic data and behavioral assessment data are shown in Table 1. The repeated measures analysis of the unmetabolized fraction of [11C]McN5652 (5 time points) indicated no differences between the four groups over the This study has several major findings. First, REC RAN had elevated [11C]McN5652 BP in the dorsal raphe and anteroventral striatum in comparison to REC BAN. Furthermore, REC BAN had decreased [11C]McN5652 BP in the anteroventral striatum in comparison to REC BN. These findings suggest that subtypes of ED have differences in 5-HT Psychopharmacology Table 1 Demographic values between groups CW (n=10) REC RAN (n=11) REC BAN (n=7) REC BN (n=9) SD Mean SD Mean SD Sig. 24.74 20.74 13.33 (9) 15.91 43.36 43.10 42.33 19.56 (9) 0.83 0.31 0.52 (9) 15.00 4.67 13.78 (9) 0.30 0.67 18.60 (10) 5.48 2.44 2.25 3.21 49.52 26.68 0.31 3.87 4.09 23.66 21.75 15.14 15.83 (6) 12.00 (6) 25.2 (5) 0.52 (4) 16 (5) 18.57 4.17 2.27 1.53 1.94 13.56 25.37 0.21 2.45 3.36 24.44 23.24 18.59 17.38 (8) 17.13 (8) 90.56 1.25 (8) 16.11 19.78 5.27 2.76 1.76 4.69 10.16 99.65 1.46 6.17 1.39 0.396 0.119 <0.001 2, 3<1, 4 0.622 0.143 0.083 0.215 0.729 <0.001 1<2, 3, 4 53.80 20.90 8.40 28.70 80.90 0.00 12.26 4.98 4.22 5.14 21.14 0.00 111.82 15.27 18.00 45.00 72.27 4.64 17.10 7.42 6.26 12.81 21.64 6.39 113.43 21.71 12.86 38.71 88.71 8.00 (6) 20.32 8.50 10.78 12.35 22.22 8.99 99.11 20.32 19.88 47.33 98.33 11.63 (8) 22.03 8.28 6.28 9.80 25.92 10.46 <0.001 0.210 0.004 0.002 0.092 0.013 0.30 0.95 6.18 6.62 6.67 (6) 5.79 5.88 (8) 5.06 0.034 1.50 2.27 8.36 6.82 6.00 4.97 9.11 9.84 0.063 Mean SD Age (years) Current BMI (kg/m2) Low BMI (lifetime) (kg/m2) Age of Onset (years of age) Length of Recovery (months) Estradiol (pg/mL) β-hydroxybuteric Acid (mg/dL) Cortisol (mcg/dl) EDI 2 –Drive for Thinness (“worst ever”) (Garner 1990) Perfectionism (MPS) (Frost et al. 1990) Novelty Seeking (TCI (Cloninger 1987)) Harm Avoidance (TCI) Trait Anxiety (STAI) (Spielberger et al. 1970) Self Control (BIS (Barratt and Patton 1983)) Yale-Brown Obsessive-Compulsive Scale (YBOCS) (Goodman et al. 1989a,b) Yale-Brown-Cornell Eating Disorders Scale (YBC-EDS) (Mazure et al. 1994; Sunday et al. 1995) Depression (BDI) (Beck et al. 1961) Mean 27.93 6.89 22.66 2.02 20.37 1.60 ANOVA Group Diff. 1<2, 3, 4 1<2, 4 1<2, 4 1<4 Group comparisons by ANOVA Sig. Significance; CW healthy control women; REC RAN recovered anorexic women, restricting type; REC BAN recovered anorexic women, bulimic-type; REC BN recovered bulimic women; BDI Beck Depression Inventory; TCI Temperament and Character Inventory; BIS Barratt Impulsiveness Scale; STAI State Trait Anxiety Inventory; MPS Multidimensional Perfectionism Scale function, which may provide important insights into why these groups have differences in affective regulation and impulse control. To our knowledge, imaging studies of 5-HTT have not been done in individuals with RAN, whether ill or recovered. Other imaging studies have found reduced 5HTT levels in symptomatic BN subjects. Tauscher et al. (2001) found reduced [123I]beta-CIT binding in ten individuals who were ill with BN. Two of those individuals had a history of AN, but specific imaging data for those two individuals were not identified. Kuikka et al. (2001) found reduced [123I]beta-CIT binding values in subjects ill with binge eating disorder. In addition, Steiger et al. (2005b) showed that individuals remitted from BN have reduced platelet [3H]paroxetine binding. We found that reduced [11C]McN5652 BP appeared to occur mainly in the remitted BAN, not the REC BN subjects. New studies, seeking to replicate these findings with [11C]DASB, a more specific Table 2 Regional [11C]McN5652 binding potential (BP) between groups Dorsal raphe Antero-ventral striatum Thalamus Dorsal caudate Subgenual cingulate CW (n=10) REC RAN (n=11) REC BAN (n=7) REC BN (n=9) ANOVA Mean SD Mean SD Mean SD Mean SD df F 1.169 0.743 0.693 0.526 0.239 0.337 0.129 0.221 0.129 0.052 1.316 0.835 0.744 0.553 0.237 0.288 0.117 0.201 0.137 0.105 0.749 0.549 0.519 0.575 0.236 0.332 0.236 0.085 0.180 0.066 1.027 0.767 0.722 0.565 0.224 0.348 0.133 0.327 0.155 0.086 3.35 3.35 3.35 3.35 3.35 4.65 5.19 1.54 0.19 0.06 Uncorrected p value Tukey-Kramer Multiple Comparison 0.008 0.004 0.073 0.882 0.752 2>3 2>3; 3<4 Group comparisons by ANOVA. The cerebellar DV values were similar between groups (CW, 21.23±5.07; REC RAN, 20.56±5.62; REC BAN, 20.58±4.75; REC BN, 22.30±3.54; p=.860). CW healthy comparison women; REC RAN recovered anorexic women, restricting type; REC BAN recovered anorexic women, bulimic-type; REC BN recovered bulimic women Psychopharmacology 2.0 1.2 1.8 1.0 [11C]McN 5652 BP 1.6 [11C]McN 5652 BP Fig. 2 Scatterplots of the [11C] McN5652 binding potential (BP) values in the dorsal raphe (left plot) and antero-ventral striatum (right plot). CW Healthy control women; REC RAN recovered anorexic women, restricting type; REC BAN recovered anorexic women, bulimic-type; REC BN recovered bulimic women 1.4 1.2 1.0 0.8 0.6 0.8 0.6 0.4 0.4 0.2 CW R REC AN B REC AN radiotracer for a reliable quantification of 5-HTT parameters in regions of moderate 5-HTT density, including the limbic regions (Frankle et al. 2004), are in progress. Still, this finding raises the possibility that these data can be used to understand who might respond to medication. The eating disorders are thought to share a common vulnerability, as crossover between subtypes is common (Herzog et al. 1996) and subtypes are cross-transmitted in families (Kendler et al. 1995; Lilenfeld et al. 1998; Strober et al. 2000). However, other factors appear to differentiate subtypes of AN and BN, including degree of weight loss, affect regulation, self-control, and perhaps response to SSRI medication (Kaye et al. 2004). It should be noted that we only studied recovered individuals with “pure” subtypes. For example, RAN individuals had never engaged in bulimic behaviors. While BN individuals show a response to higher doses of fluoxetine (Fluoxetine Bulimia Nervosa Collaborative Study Group 1992), the efficacy of such medication has been questioned, as relatively few individuals abstain from binge and purge behaviors, and relapse during treatment is common (Walsh 1991). It remains controversial whether BN 0.2 CW REC RAN REC BAN REC 0.8 p = .03 p = .01 0.7 0.7 0.6 0.6 0.5 0.5 0.4 0.4 0.3 0.3 0.2 0.2 SS LL Genotype BN SSRIs are effective in RAN individuals (Kaye et al. 2001b; Walsh et al. 2006). Our clinical experience (Kaye et al. 1991b) suggests that individuals with RAN respond better to fluoxetine than those with BAN did and that some individuals with BN can be relatively insensitive to high doses of SSRIs. There is little data determining whether BAN and BN individuals have differential responses to SSRIs. While highly speculative, our findings raise the provocative possibility that decreased 5-HTT function may be related to poor response to SSRI medication, whereas individuals with increased 5-HTT activity may respond to higher SSRI doses. Thus, PET and radioligand studies may be a useful tool for investigating and managing medication response in treatment resistant individuals. In general, the REC RAN individuals had elevated 5HTT binding, suggesting they have relatively greater 5-HT uptake and reduced extracellular 5-HT compared to REC BAN and BN. In support of this possibility, the REC BAN and BN individuals tend to have higher binding of 5-HT1A post-synaptic receptors and autoreceptors (Bailer et al. 2005; Kaye et al., unpublished data), which may be a compensatory means of downregulating raphe activity 0.8 [11C]McN 5652 BP dorsal caudate Fig. 3 Scatterplot of [ 11 C] McN5652 binding potential (BP) in the dorsal caudate in the CW and REC eating disorder sample (left graph) and REC eating disorder only (right graph) by 5-HTLPR genotype (SS and LL only) REC SS LL Genotype Psychopharmacology (Cooper 1996; Hajos et al. 2003). Moreover, reduced 5HTT activity, in terms of genotypes (Steiger et al. 2005a), has been associated with affect dysregulation, which tends to be more common in the bulimic subgroups. Furthermore, in people with impulsive aggressivity, reduced 5-HTT binding was found in the anterior cingulate cortex, a region involved in affect regulation (Frankle et al. 2005). Imaging studies (using SPECT or PET) in other psychiatric disorders with altered affect regulation have revealed inconsistent results. In obsessive–compulsive disorder, increased (Pogarell et al. 2003), unaltered (Simpson et al. 2003), or decreased 5-HTT binding (Hesse et al. 2005; StenglerWenzke et al. 2004; Zitterl et al. 2007) was found. Results remain contradictory in depression as well (see Hesse et al. 2004 for review). The functional polymorphism in the promoter region of the human 5-HTT gene (SLC6A4) has been implicated in the modulation of mood and antidepressant response (Murphy et al. 2004). We included data on possible relationships between 5-HTTLPR and [11C]McN5652 BP, despite our concerns that the sample was small, because of the interest in this topic. Several lines of evidence show that the genotype with two copies of the long (L, 528 bp) allele leads to greater 5-HT reuptake compared to genotypes having either one or two copies of the short (S, 484 bp) allele (Lesch et al. 1996). As 5-HTT regulates 5-HT concentrations in the synaptic cleft by recycling released 5-HT, individuals with the S allele are likely to have higher extracellular 5-HT due to decreased 5-HT reuptake (Lesch et al. 1996; Sundaramurthy et al. 2000). In other disorders, relationships between 5-HTTLPR genotypes and imaging measures of the transporter measures have been reported to occur (Heinz et al. 2000; Little et al. 1998) or not (Parsey et al. 2006; Shioe et al. 2003; Willeit et al. 2001). Some, but not all studies, have found increased S allele frequency in BN and AN (Di Bella et al. 2000; Fumeron et al. 2001; Hinney et al. 1997; Lauzurica et al. 2003; Matsushita et al. 2004; Sundaramurthy et al. 2000). The data in our study suggest that SS homozygous individuals have reduced 5HTT binding in the dorsal caudate. In individuals with BN, the S allele has been associated with poor response to SSRI therapy (Monteleone et al. 2005) and outpatient multimodal group therapy (K. Bruce, personal communication), as well as greater affective instability and impulsivity (Steiger et al. 2005a). Together, these data further support the possibility that there is a group of individuals with ED who have decreased 5-HTT function, and these individuals may respond poorly to treatment. The subjects in our study were all white women, 18 to 45 years old, studied in their early follicular menstrual phase. Other studies have been less homogenous, which may obscure potential findings. In terms of limitations, the sample size is small, and replication of these findings in larger samples is clearly needed. The major limitation of the radioligand used in this study is the high nonspecific binding, precluding reliable measurement of 5-HTT in the human neocortex; we therefore restricted our ROI analysis to regions for which the derivation of [11C]McN5652 BP has been found reliable (Parsey et al. 2000) and in which we previously found alterations. Persistent alterations in monoamine activity after recovery raise the question of whether this is a premorbid vulnerability for developing ED symptoms. Alternatively, it is possible that chronic disturbances of nutrition during the ill state might contribute to a persistent “scar” in recovered individuals, caused by chronic malnutrition and emaciation. Patients were off medication (e.g., SSRIs) for greater than 3 months, so it is unlikely that persistent effects of 5-HT active medication accounted for the results. Fourteen ED subjects (3 REC RAN, 5 REC BAN, and 6 REC BN) were on SSRIs in the past. There was no difference in [11C]McN BP across ROIs between subjects who were or were not on SSRIs in the past within each group and within the entire group of REC ED subjects. In summary, these data support and extend studies suggesting that a disturbance of 5-HTT neuronal function persists after normalization of weight and nutritional status in people who have had eating disorders. Acknowledgements The authors are indebted to the participating individuals for their contribution of time and effort in support of this study. We would like to thank W. Gordon Frankle for review of this manuscript, Eva Gerardi and Katherine Plotnicov for editorial assistance, and the University of Pittsburgh Medical Center PET Facility staff for their invaluable contribution to this study. This study was supported by grants from National Institute of Mental Health (NIMH) MH46001, MH42984, K05-MD01894, NIMH Training Grant T32-MH18399, and the Price Foundation. U.F.B. was funded by an Erwin-Schrödinger-Fellowship of the Austrian Science Fund (nos. J 2188 and J 2359-B02). References American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders, 4 edn. American Psychiatric Association Bailer UF, Price JC, Meltzer CC, Mathis CA, Frank GK, Weissfeld L, McConaha CW, Henry SE, Brooks-Achenbach S, Barbarich NC, Kaye WH (2004) Altered 5-HT2A receptor binding after recovery from bulimia-type anorexia nervosa: relationships to harm avoidance and drive for thinness. Neuropsychopharmacology 29:1143–1155 Bailer UF, Frank GK, Henry SE, Price JC, Meltzer CC, Weissfeld L, Mathis CA, Drevets WC, Wagner A, Hoge J, Ziolko SK, McConana CW, Kaye WH (2005) Altered brain serotonin 5HT1A receptor binding after recovery from anorexia nervosa measured by positron emission tomography and [11C] WAY100635. Arch Gen Psychiatry 62:1032 Bailer UF, Frank G, Henry S, Price J, Meltzer C, Mathis C, Wagner A, Thornton L, Hoge J, Ziolko SK, Becker C, McConaha C, Kaye WH (2007) Exaggerated 5-HT1A but normal 5-HT2A receptor Psychopharmacology activity in individuals ill with anorexia nervosa. Biol. Psychiatry 61:1090–1099 Barratt ES, Patton JH (1983) Impulsivity: cognitive, behavioral, and psychophysiological correlates. In: Zuckerman M (ed) Biological bases of sensation seeking, impulsivity, and anxiety. Lawrence Earlbaum Associates, Hillsdale, NJ, p 85 Beck AT, Ward M, Mendelson M, Mock J, Erbaugh J (1961) An inventory for measuring depression. Arch Gen Psychiatry 4:53–63 Blundell JE (1984) Serotonin and appetite. Neuropharmacology 23:1537–1551 Brewerton TD, Jimerson DC (1996) Studies of serotonin function in anorexia nervosa. Psychiatry Res 62:31–42 Cho R, Kapur S, Du L, Hrdina PD (1999) Relationship between central and peripheral serotonin 5-HT2A receptors: a positron emission tomography study in healthy individuals. Neurosci Lett 261:139–142 Cloninger CR (1987) A systematic method for clinical description and classification of personality variants. A proposal. Arch Gen Psychiatry 44:573–588 Cloninger CR, Przybeck TR, Svrakic DM, Wetzel RD (1994) The Temperament and Character Inventory (TCI): a guide to its development and use. Center for Psychobiology of Personality, Washington University, St. Louis, MO Company MLI (1959) New weight standards for men and women. Stat Bull Metrop Insur Co, pp 1–11 Cooper SJ (1996) Cholecystokinin modulation of serotonergic control of feeding behavior. Ann N Y Acad Sci 780:213–222 Di Bella DD, Catalano M, Cavallini MC, Riboldi C, Bellodi L (2000) Serotonin transporter linked polymorphic region in anorexia nervosa and bulimia nervosa. Mol Psychiatry 5:233–234 Drevets W, Gautier C, Price J, Kupfer D, Kinahan P, Grace A, Price J, Mathis C (2001) Amphetamine-induced dopamine release in human ventral striatum correlates with euphoria. Biol Psychiatry 49:81–96 Edenberg H, Reynolds J (1998) Improved method for detecting the long and short promoter alleles of the serotonin transporter gene HTT (SLC6A4). Psychiatric Genetics 8:193–195 Fichter MM, Pirke KM, Pollinger J, Wolfram GM, Brunner E (1990) Disturbances in the hypothalamo-pituitary-adrenal and other neuroendocrine axes in bulimia. Biol Psychiatry 27:1021–1037 First MB, Gibbon M, Spitzer RL, Williams JBW (1996) Users guide for the structured clinical interview for DSM-IV Axis I disorders— research version (SCID-I, version 2.0, February 1996 Final Version). Biometrics Research Department, New York State Psychiatric Institute, New York Fluoxetine Bulimia Nervosa Collaborative Study Group (1992) Fluoxetine in the treatment of bulimia nervosa. A multicenter, placebo-controlled, double-blind trial. Arch Gen Psychiatry 49:139–147 Frank GK, Kaye WH, Weltzin TE, Perel J, Moss H, McConaha C, Pollice C (2001) Altered response to meta-chlorophenylpiperazine in anorexia nervosa: support for a persistent alteration of serotonin activity after short-term weight restoration. Int J Eat Disord 30:57–68 Frank GK, Kaye WH, Meltzer CC, Price JC, Greer P, McConaha C, Skovira K (2002) Reduced 5-HT2A receptor binding after recovery from anorexia nervosa. Biol Psychiatry 52:896–906 Frank G, Bailer UF, Henry S, Drevets W, Meltzer CC, Price JC, Mathis C, Wagner A, Hoge J, Ziolko SK, Barbarich N, Weissfeld L, Kaye W (2005) Increased dopamine D2/D3 receptor binding after recovery from anorexia nervosa measured by positron emission tomography and [11C]raclopride. Biol Psychiatry 58:908–912 Frankle W, Huang Y, Hwang D, Talbot P, Slifstein M, Van Heertum R, Abi-Dargham A, Laruelle M (2004) Comparative evaluation of serotonin transporter radioligands 11C-DASB and 11C-McN 5652 in healthy humans. J Nucl Med 45:682–694 Frankle W, Lombardo I, New AS, Goodman M, Talbot P, Huang Y, Hwang D, Slifstein M, Curry S, Abi-Dargham A, Lauruelle M, Siever L (2005) Brain serotonin transporter distribution in subjects with impulsive aggressivity: a positron emission study with [11C]McN 5652. Am J Psychiatry 162:915–923 Frost RO, Marten P, Lahart C, Rosenblate R (1990) The dimensions of perfectionism. Cognitive Therapy & Research 14:449–468 Fumeron F, Betoulle D, Aubert R, Herbeth B, Siest G, Rigaud D (2001) Association of a functional 5-HT transporter gene polymorphism with anorexia nervosa and food intake. Mol Psychiatry 6:9–10 Garner DM (1990) Eating disorder inventory-2 professional manual. Psychological Assessment Resources, Odessa, FL Goodman WK, Price LH, Rasmussen SA, Mazure C, Delgado P, Heninger GR, Charney DS (1989a) The Yale-Brown obsessive compulsive scale. II. Validity. Arch Gen Psychiatry 46:1012– 1016 Goodman WK, Price LH, Rasmussen SA, Mazure C, Fleischmann RL, Hill CL, Heninger GR, Charney DS (1989b) The Yale-brown obsessive compulsive scale. I. Development, use, and reliability. Arch Gen Psychiatry 46:1006–1011 Gorwood P (2004) Eating disorders, serotonin transporter polymorphisms and potential treatment response. Am J Pharmacogenomics 4:9–17 Hajos M, Gartside SE, Varga V, Sharp T (2003) In vivo inhibition of neuronal activity in the rat ventromedial prefrontal cortex by midbrain-raphe nuclei: role of 5-HT1A receptors. Neuropharmacology 45:72–81 Heinz A, Jones D, Mazzanti C, Goldman D, Ragan P, Hommer D, Linnoila M, Weinberger D (2000) A relationship between serotonin transporter genotype and in vitro protein expression and alcohol neurotoxicity. Biol Psychiatry 48:334–335 Herzog DB, Field AE, Keller MB, West JC, Robbins WM, Staley J, Colditz GA (1996) Subtyping eating disorders: is it justified. J Am Acad Child Adolesc Psychiatry 35:928–936 Hesse S, Barthel H, Schwarz J, Sabri O, Muller U (2004) Advances in in vivo imaging of serotonergic neurons in neuropsychiatric disorders. Neurosci Biobehav Rev 29:1119 Hesse S, Muller U, Lincke T, Barthel H, Villman T, Angermeyer M, Sabri O, Stengler-Wenzke K (2005) Serotonin and dopamine transporter imaging in patients with obsessive–compulsive disorder. Psych Res 140:63–72 Higley JD, Linnoila M (1997) Low central nervous system serotonergic activity is traitlike and correlates with impulsive behavior. A nonhuman primate model investigating genetic and environmental influences on neurotransmission. Ann NY Acad Sci 836:39–56 Hinney A, Barth N, Ziegler A, von Prittwitz S, Hamann A, Hennighausen K, Pirke KM, Heils A, Rosenkranz K, Roth H, Coners H, Mayer H, Herzog W, Siegfried A, Lehmkuhl G, Poustka F, Schmidt MH, Schafer H, Grzeschik KH, Lesch KP, Lentes KU, Remschmidt H, Hebebrand J (1997) Serotonin transporter gene-linked polymorphic region: allele distributions in relationship to body weight and in anorexia nervosa. Life Sci 61:PL295–PL303 Kaye WH, Gwirtsman HE, George DT, Ebert MH (1991a) Altered serotonin activity in anorexia nervosa after long-term weight restoration. Does elevated cerebrospinal fluid 5-hydroxyindoleacetic acid level correlate with rigid and obsessive behavior? Arch Gen Psychiatry 48:556–562 Kaye WH, Weltzin TE, Hsu LK, Bulik CM (1991b) An open trial of fluoxetine in patients with anorexia nervosa. J Clin Psychiatry 52:464–471 Psychopharmacology Kaye WH, Frank GK, Meltzer CC, Price JC, McConaha CW, Crossan PJ, Klump KL, Rhodes L (2001a) Altered serotonin 2A receptor activity in women who have recovered from bulimia nervosa. Am J Psychiatry 158:1152–1155 Kaye WH, Nagata T, Weltzin TE, Hsu LK, Sokol MS, McConaha C, Plotnicov KH, Weise J, Deep D (2001b) Double-blind placebocontrolled administration of fluoxetine in restricting- and restricting-purging-type anorexia nervosa. Biol Psychiatry 49:644–652 Kaye WH, Barbarich NC, Putnam K, Gendall KA, Fernstrom J, Fernstrom M, McConaha CW, Kishore A (2003) Anxiolytic effects of acute tryptophan depletion in anorexia nervosa. Int J Eat Disord 33:257–267 Kaye W, Strober M, Jimerson D (2004) The neurobiology of eating disorders. In: Charney DS, Nestler EJ (eds) The neurobiology of mental illness. Oxford Press, New York, pp 1112–1128 Kendler KS, Walters EE, Neale MC, Kessler RC, Heath AC, Eaves LJ (1995) The structure of the genetic and environmental risk factors for six major psychiatric disorders in women. Phobia, generalized anxiety disorder, panic disorder, bulimia, major depression, and alcoholism. Arch Gen Psychiatry 52:374–383 Kuikka JT, Tammela L, Karhunen L, Rissanen A, Bergstrom KA, Naukkarinen H, Vanninen E, Karhu J, Lappalainen R, Repo-Tiihonen E, Tiihonen J, Uusitupa M (2001) Reduced serotonin transporter binding in binge eating women. Psychopharmacology (Berl) 155:310–314 Lauzurica N, Hurtado A, Escarti A, Delgado M, Barrios V, Morande G, Soriano J, Jauregui I, Gonzalez-Valdemoro M, Garcia-Camba E, Fuentes J (2003) Polymorphisms within the promoter and the intron 2 of the serotonin transporter gene in a population of bulimic patients. Neurosci Lett 352:226–230 Leibowitz SF, Shor-Posner G (1986) Brain serotonin and eating behavior. Appetite 7:1–14 Lesch K, Bengel D, Heils A, Sabol S, Greenberg B, Petri S, Benjamin J, Muller C, Hamer D, Murphy D (1996) Association of anxietyrelated traits with a polymorphism in the serotonin transporter gene regulatory region. Science 274:1527–1531 Lilenfeld LR, Kaye WH, Greeno CG, Merikangas KR, Plotnicov K, Pollice C, Rao R, Strober M, Bulik CM, Nagy L (1998) A controlled family study of anorexia nervosa and bulimia nervosa: psychiatric disorders in first-degree relatives and effects of proband comorbidity. Arch Gen Psychiatry 55:603–610 Little K, McLaughlin D, Zhang L, Livermore C, Dalack G, McFinton P, DelProposto A, Hill E, Cassin B, Watson S, Cook E (1998) Cocaine, ethanol, and genotype effects on human midbrain serotonin transporter binding sites and mRNA levels. Am J Psych 155:207–213 Lopresti B, Mathis C, Price J, Villemagne V, Meltzer C, Holt D, Smith G, Moore R (2001) Serotonin transporter binding in vivo: further examination of [11C]McN5652 molecular and pharmacological brain imaging with positron emission tomography. Academic, San Diego, pp 265–271 Lucki I (1998) The spectrum of behaviors influenced by serotonin. Biol Psychiatry 44:151–162 Mann JJ (1999) Role of the serotonergic system in the pathogenesis of major depression and suicidal behavior. Neuropsychopharmacology 21:99S–105S Matsushita S, Suzuki K, Murayama M, Nishiguchi N, Hishimoto A, Takeda A, Shirakawa O, Higuchi S (2004) Serotonin transporter regulatory region polymorphism is associated with anorexia nervosa. Am J Med Genet B Neuropsychiatr Genet 128B:114–117 Mazure CM, Halmi KA, Sunday SR, Romano SJ, Einhorn AM (1994) The Yale-Brown-Cornell eating disorder scale: development, use, reliability and validity. J Psych Res 28:425–445 Meltzer CC, Zubieta JK, Links JM, Brakeman P, Stumpf MJ, Frost JJ (1996) MR-based correction of brain PET measurements for heterogeneous gray matter radioactivity distribution. J Cereb Blood Flow Metab 16:650–657 Meltzer CC, Kinaham P, Nichols TE, Greer PJ, Comtat C, Cantwell MN, Price J (1999) Comparative evaluation of MR-based partial-volume correction schemes for PET. J Nucl Med 40:2053–2065 Monteleone P, Santonastaso P, Tortorella A, Favaro A, Fabrazzo M, Castaldo E, Caregaro L, Fuschino A, Maj M (2005) Serotonin transporter polymorphism and potential response to SSRIs in bulimia nervosa. Mol Psychiatry 10:716–718 Murphy D, Lerner A, Rudnick G, Lesch K (2004) Serotonin transporter: gene, genetic disorders, and pharmacogenetics. Mol Interv 4:109–123 Parsey RV, Kegeles LS, Hwang DR, Simpson N, Abi-Dargham A, Mawlawi O, Slifstein M, Van Heertum RL, Mann JJ, Laruelle M (2000) In vivo quantification of brain serotonin transporters in humans using [11C]McN 5652. J Nucl Med 41:1465–1477 Parsey RV, Hastings RS, Oquendo MA, Hu X, Goldman D, Huang Y, Simpson N, Arcement J, Huang Y, Ogden RT, Van Heertum R, Arango V, Mann JJ (2006) Effect of a triallelic functional polymorphism of the serotonin-transporter-linked promoter region on expression of serotonin transporter in the human brain. Am J Psych 163:48–51 Pogarell O, Hamann C, Popperl G, Juckel G, Chouker M, Zaudig M, Riedel M, Moller H, Hegerl U, Tatsch K (2003) Elevated brain serotonin transporter availability in patients with obsessivecompulsive disorder. Biol Psychiatry 54:1406–1413 Shioe K, Ichimiya T, Suhara T, Takano A, Sudo Y, Yasuno F, Hirano M, Shinobara M, Kagami M, Okubo Y, Nankai M, Kanba S (2003) No association between genotype of the promoter region of serotonin transporter gene and serotonin transporter binding in human brain measured by PET. Synapse 15:184–188 Simpson H, Lombardo I, Slifstein M, Huang H, Hwang D, Abi-Dargham A, Liebowitz MR, Laruelle M (2003) Serotonin transporters in obsessive-compulsive disorder: a positron emission tomography study with [11C]McN 5652. Biol Psychiatry 54:1414–1421 Smith KA, Morris JS, Friston KJ, Cowen PJ, Dolan RJ (1999) Brain mechanisms associated with depressive relapse and associated cognitive impairment following acute tryptophan depletion. Brit J Psychiatry 174:525–529 Soubrie P (1986) Reconciling the role of central serotonin neurons in human and animal behavior. Beh Brain Sci 9:319 Spielberger CD, Gorsuch RL, Lushene RE (1970) STAI manual for the state trait anxiety inventory. Consulting Psychologists Press, Palo Alto, CA Steiger H, Joober R, Israel M, Young S, Ng Ying Kin NM, Gauvin L, Bruce K, Joncas J, Torkaman-Zehi A (2005a) The 5HTTLPR polymorphism, psychopathological symptoms, and platelet [3H-] paroxetine binding in bulimic syndromes. Int J Eat Disord 37:57–60 Steiger H, Richardson J, Israel M, Ng Ying Kin NM, Bruce K, Mansour S, Marie Parent A (2005b) Reduced density of plateletbinding sites for [3H]paroxetine in remitted bulimic women. Neuropsychopharmacology 30:1028–1032 Stengler-Wenzke K, Muller U, Angermeyer M, Sabri O, Hesse S (2004) Reduced serotonin transporter-availability in obsessive– compulsive disorder (OCD). Eur Arch Psychiatry Clin Neurosci 254:252–255 Strober M, Freeman R, Lampert C, Diamond J, Kaye W (2000) Controlled family study of anorexia nervosa and bulimia nervosa: evidence of shared liability and transmission of partial syndromes. Am J Psychiatry 157:393–401 Sundaramurthy D, Pieri LF, Gape H, Markham AF, Campbell DA (2000) Analysis of the serotonin transporter gene linked polymorphism (5-HTTLPR) in anorexia nervosa. Am J Med Genet Neuropsychiatr Genet 96:53–55 Psychopharmacology Sunday SR, Halmi KA, Einhorn A (1995) The Yale-Brown-Cornell eating disorder scale: a new scale to assess eating disorder symptomatology. Int J Eat Disord 18:237–245 Tauscher J, Pirker W, Willeit M, de Zwaan M, Bailer U, Neumeister A, Asenbaum S, Lennkh C, Praschak-Rieder N, Brücke T, Kasper S (2001) [123I]beta-CIT and single photon emission computed tomography reveal reduced brain serotonin transporter availability in bulimia nervosa. Biol Psychiatry 49:326– 332 Uebelhack R, Franke L, Herold N, Plotkin M, Amthauer H, Felix R (2006) Brain and platelet serotonin transporter in humans– correlation between [123I]-ADAM SPECT and serotonergic measurements in platelets. Neurosci Lett 406:153–158 Wagner A, Barbarich N, Frank G, Bailer UF, Weissfeld L, Henry S, Achenbach S, Vogel V, Plotnicov K, McConaha C, Kaye W, Wonderlich S (2006) Personality traits after recovery from eating disorders: Do subtypes differ. Int J Eat Disord 39:276– 284 Walsh BT (1991) Psychopharmacologic treatment of bulimia nervosa. J Clin Psychiatry 52Suppl:34–38 Walsh BT, Devlin MJ (1998) Eating disorders: progress and problems. Science 280:1387–1390 Walsh B, Kaplan A, Attia E, Olmsted M, Parides M, Carter J, Pike K, Devlin M, Woodside B, Roberto C, Rocket W (2006) Fluoxetine after weight restoration in anorexia nervosa: a randomized controlled trial. JAMA 295:2605–2612 Ward A, Brown N, Lightman S, Campbell IC, Treasure J (1998) Neuroendocrine, appetitive and behavioural responses to dfenfluramine in women recovered from anorexia nervosa. Br J Psychiatry 172:351–358 Willeit M, Stastny J, Pirker W, Praschak-Rieder N, Neumeister A, Asenbaum S, Tauscher J, Fuchs K, Sieghart W, Hornik K, Aschauer H, Brucke T, Kasper S (2001) No evidence for in vivo regulation of midbrain serotonin transporter availability by serotonin transporter promoter gene polymorphism. Biol Psychiatry 50:8–12 Wolfe BE, Metzger ED, Jimerson DC (1997) Research update on serotonin function in bulimia nervosa and anorexia nervosa. Psychopharmacol Bull 33:345–354 Yatham L, Steiner M, Liddle P, Shiah I, Lam R, Zis A, Coote M (2000) A PET study of brain 5-HT2A receptors and their correlation with platelet 5-HT2 recptors in healthy humans. Psychopharmacology (Berl) 15:424–427 Zitterl W, Aigner M, Stompe T, Zitterl-Eglseer K, Gutierrez-Lobos K, Schmidl-Mohl B, Wenzel T, Demal U, Zettinig G, Hornik K, Thau K (2007) [(123)I]-beta-CIT SPECT imaging shows reduced thalamus–hypothalamus serotonin transporter availability in 24 drug-free obsessive–compulsive checkers. Neuropsychopharmacology 32(8):1661–1668