Service Income Requisition Print Form
advertisement

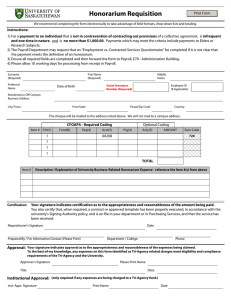
Service Income Requisition Print Form We recommend completing the form electronically to take advantage of field formats, drop-down lists and totaling. Instructions: 1) For a service income payment to an INDIVIDUAL as a guest lecturer/speaker, an academic reviewer, or for a contracted service. 2) Payments will NOT be processed unless the following documents are attached to this form: a) Details describing the guest lecturer/speaker or academic reviewer service arrangement or b) The completed signed copy of the "Certification Page" of the "Employment vs. Contracted Services Questionnaire" or the "Recurring Engagement/ Approved Contract Template / Certification Page" and the service provider's invoice. 3) Ensure all required fields are completed and then forward the form to Payroll, E70 - Administration Building. 4) Please allow 10 working days for processing from receipt in Payroll. Surname (Required) First Name (Required) Preferred Name Middle Name Social Insurance Number (Required) Date of Birth Employee ID (If Applicable) Residential or Off-Campus Business Address City/Town Prov/State Postal/Zip Code Country The cheque will be mailed to the address noted above. We will not mail to a campus address. If amount is greater than $5,000.00 enter contract number Enter Worker's Compensation Board number if applicable CFOAPA - Required Coding Item # Cht(1) Fund(6) 1 Org(4) Acct(5) Optional Coding Prg(4) Acty(5) AMOUNT 70403 Earn Code 723 1 1 1 TOTAL Description / Explanation of University Business-Related Service Expense - reference the Item #(s) from above Item # Certification: Your signature indicates certification as to the appropriateness and reasonableness of the amount being paid. You also certify that, when required, a contract or approved template has been properly executed, in accordance with the university's Signing Authority policy, and is on file in your department or in Purchasing Services, and that the service has been received. Requisitioner's Signature Prepared By / For Information Contact (Please Print) Date Department / College Phone Approval: Your signature indicates approval as to the appropriateness and reasonableness of the expenses being claimed. To the best of my knowledge, any expenses on this form identified as Tri-Agency related charges meet eligibility and compliance requirements of the Tri-Agency and the University. Approver's Signature Please Print Name Title Date Institutional Approval: (only required if any expenses are being charged to a Tri-Agency fund.) Inst. Appr. Signature Print Name Date