Human Resources Wellness Incentive Program Full-Time Faculty Program Overview 2015–2016
advertisement

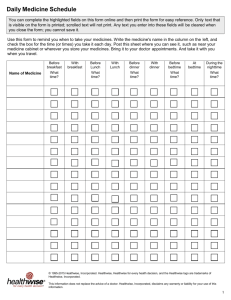
Human Resources Wellness Incentive Program Full-Time Faculty Program Overview 2015–2016 Here is all the information that you need to know in order to earn your Wellness Incentive — $240.00 (prorated per pay period) off your annual health insurance premiums. • Requirements must be completed between July 1, 2015 and June 9, 2016 and submitted to Human Resources by June 13, 2016. Refer to the Faculty Contract for specific information on types of eligible requirements. • Proof of Completion — See the requirements for proof of completion listed for each activity. Names of participants for the Annual Health Power Profile are held on file in HR, therefore, no proof of participation is required. • In order to earn the reduction in your health insurance premiums, you must complete the following requirements listed below. If approved for the Wellness Incentive, Faculty on 26 pays will get a $10.00 reduction that will begin the first payroll of the fiscal year and continue for 24 payrolls. Faculty on 20 pays will get a $12.00 reduction that will begin the first payroll of the academic year and continue for 20 payrolls. This also applies if a spouse has been approved for the Wellness Incentive. • Complete the Annual Health Power Profile offered each year. This is a mandatory requirement. In addition to participation in the mandatory Annual Health Power Profile, you will need to provide proof of completion of three (3) of the following requirements in the same fiscal year as the Health Power Profile. 1) Minimum of one activity class at COD or equivalent. Accepted activity classes include: • Any PE Activity Class Proof of Completion: Copy of final grade report or transcript for COD PE class or letter from instructor or fitness program for PE classes taken outside of COD. • Health Club Membership Proof of Completion: Copy of Health Club Membership receipt of payment indicating current fiscal year enrollment and active participation or record of health club visits. • Participation of run or walk in “Laps with the Chaps” 5K Proof of Completion: Documentation that you participated in the run or walk. Other activity equivalents are handled on an individual basis. Please contact Human Resources if you have a question or to verify activity eligibility. Two (2) different activities in the above category may be used towards satisfaction of the three (3) required in addition to the Health Power Profile. 2) TLC Class Offering (or TLC Self-Study Class) Only classes approved for this benefit, taken voluntarily by the Faculty Member and not used for any other benefit under this agreement. Specific class offering eligibility requirements will be noted in the TLC offering announcements as they become available. Proof of Completion: Copy of certificate of completion. 3) Supervised Weight Loss Program Participation in a supervised weight loss program for a minimum of 10 weeks. Proof of Completion: Copy of weight loss program enrollment and completion and receipt for payment. 4) Healthwise Handbook Usage of the Healthwise Handbook. Proof of Completion: Healthwise Handbook “Getting Healthwise” Form. This form should indicate how the book has benefited you or a family member over the past year. 5) Physical Examination Completion of a physical exam every three (3) years can be submitted. PPO Members can receive a physical exam through a preferred provider, Northwestern Medicine Occupational Health (formerly Cadence) every three (3) years. Northwestern Medicine Occupational Health can be reached at (630) 539-5270. Similar physical examinations can be scheduled through your personal physician and submitted for this benefit once every three (3) years. Please contact Human Resources if you have a question or to verify eligibility. Proof of Completion: Signed and dated document from the physician’s office indicating completion of physical examination. The same requirements listed above must be fulfilled by the employee’s covered spouse in order to earn the Wellness Incentive of an additional $240 annually (prorated per pay period) in their health insurance premiums. However, some activities (i.e., TLC Courses) are only available to COD employees. 1 of 4 HR-15-19759(8/15) Full-Time Faculty Wellness Incentive Program 2015–2016 Overview Form Please print all information clearly. This form must accompany the proof of completed requirements. Do not send form or supporting documents separately. Send all forms together to Human Resources. In order to receive credit, all materials must be received no later than June 13, 2016. Name: ____________________________________________________________________ Date: _________________________ Department: _______________________________________________________________ Extension: _____________________ Supervisor/Associate Dean’s Name: ___________________________________________________________________________ From the choices below, I am providing the required proof of completion documents for the Wellness Incentive Program: __X__ Annual Health Power Profile in Spring 2016. This is mandatory to participate in the employee Wellness Incentive Program. Names are held on file in HR, therefore proof of participation is not required. _____ PE Activity Class (maximum of two only) — including Health Club Membership which counts as one activity. _____ TLC Wellness Class (non-mandatory class sessions only) _____ Healthwise Handbook “Getting Healthwise” Form. _____ Physical Examination (once every three years) between July 1, 2015 and June 9, 2016. _____ One 10-week supervised Weight Loss Program between July 1, 2015 and June 9, 2016. _____ Laps with Chaps 5K run or walk. An email confirmation will be sent to you upon verification of enclosed documents and approval of incentive. —HR USE ONLY— Full-Time Faculty Wellness Incentive Program RECEIPT OF PROGRAM PACKET MATERIALS Date Review: __________________________ Authorized by: ________________________________________________ Requirements Verified: ______ Health Power Profile — Mandatory ______ 10-week Supervised Weight Loss Program ______ PE Activity Class ______ Physical Examination (once every 3 years) ______ Health Club Membership ______ Healthwise Handbook ______ TLC Class Approved for Wellness Incentive? 2 of 4 ❑ yes ❑ ______ Laps with Chaps 5K Run or Walk no (if no, state reason: ______________________________________) Getting Healthwise 2015–2016 Complete this form if you are using the Healthwise Handbook to earn your Wellness Incentive. Please print and return along with your Overview Sheet. All sections must be completed with specific examples or information. 1. How long have you had a Healthwise Handbook (all versions)? ___ year(s) ___ month(s) (if less than one year, state how many months) 2. Where is your copy of the Healthwise Handbook? ❑ home ❑ work 3. How often do you (or your family) use the Healthwise Handbook? ❑ once in a awhile ❑ monthly ❑ weekly 4. List which chapters you found to be the most helpful and state why below: Chapter #______: Title: ________________________________________________________________________ Chapter # ______: Title: ________________________________________________________________________ 5. What are the two most common reasons you use the Healthwise Handbook? ❑ injuries ❑ sickness (colds, flu) ❑ tips on prevention ❑ accidents ❑ first aid ❑ learn how to work with my doctor better ❑ other _____________________________________________________________________________________ 3 of 4 Getting Healthwise 2015–2016 (cont.) 6. Over the past 12 months, the Healthwise Handbook has helped me and my family to save time and money by doing the following (please enter the number of times for each below): _____ # of phone calls to doctors saved _____ # of visits to family doctor(s) saved _____ # of visits to Urgent Care/Walk-In Clinic saved _____ # of visits to Emergency Room saved 7. How have the Employee Wellness programs and services benefited you and/or your family? (check all that apply) ❑ improved my/our ability to prevent problems (i.e. accidents, injuries, diseases, aches, pains) ❑ improved my/our ability to better handle health problems ❑ helped me to be more productive at work ❑ reduced the number of times I got sick ❑ reduced the number of times family members got sick ❑ improved my/our early detection efforts ❑ improved my/our health ❑ helped to make me feel like College of DuPage cares about me and my family ❑ other (please specify): ______________________________________________________________________ _________________________________________________________________________________________________________ _________________________________________________________________________________________________________ _________________________________________________________________________________________________________ Name: _____________________________________________________________________________________________________ Signature: _______________________________________________________________ 4 of 4 Date: _______________________