Clinical/Translational Research Rationale:
advertisement

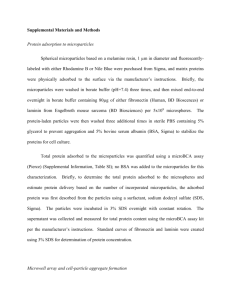
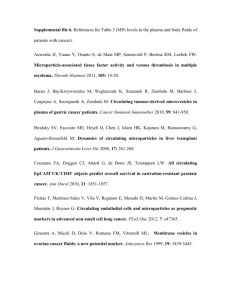
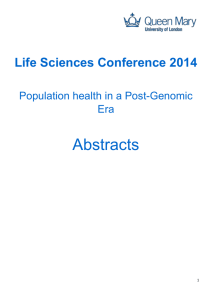
Clinical/Translational Research Dynamic Release and Clearance of Circulating Microparticles During Cardiac Stress Daniel Augustine,* Lisa V. Ayers,* Eduardo Lima, Laura Newton, Adam J. Lewandowski, Esther F. Davis, Berne Ferry, Paul Leeson Rationale: Microparticles are cell-derived membrane vesicles, relevant to a range of biological responses and known to be elevated in cardiovascular disease. Objective: To investigate microparticle release during cardiac stress and how this response differs in those with vascular disease. Methods and Results: We measured a comprehensive panel of circulating cell-derived microparticles by a standardized flow cytometric protocol in 119 patients referred for stress echocardiography. Procoagulant, platelet, erythrocyte, and endothelial but not leukocyte, granulocyte, or monocyte-derived microparticles were elevated immediately after a standardized dobutamine stress echocardiogram and decreased after 1 hour. Twenty-five patients developed stress-induced wall motion abnormalities suggestive of myocardial ischemia. They had similar baseline microparticle levels to those who did not develop ischemia, but, interestingly, their microparticle levels did not change during stress. Furthermore, no stress-induced increase was observed in those without inducible ischemia but with a history of vascular disease. Fourteen patients subsequently underwent coronary angiography. A microparticle rise during stress echocardiography had occurred only in those with normal coronary arteries. Conclusions: Procoagulant, platelet, erythrocyte, and endothelial microparticles are released during cardiac stress and then clear from the circulation during the next hour. This stress-induced rise seems to be a normal physiological response that is diminished in those with vascular disease. (Circ Res. 2014;114:109-113.) Key Words: dobutamine stress echocardiography ■ C ell-derived microparticles are subcellular membrane vesicles, ranging in size from 0.1 to 1.0 μm, that bud off during cell activation or apoptosis.1 They are identifiable in the circulation by their parent cell surface markers.2 Certain subtypes, particularly platelet derived, increase after strenuous exercise in healthy individuals,3,4 which suggests that microparticles may have a physiological function to remove stress-induced cellular by-products.5,6 Such a response could be relevant to cardiovascular disease pathogenesis because failure to clear microparticles could lead to an increase in the circulating levels of proatherogenic factors.7–9 In addition, ineffective microparticle release could lead to localized cell damage.10,11 We studied whether there is a stress-induced dynamic release and clearance of microparticles in patients exposed to cardiac stress during dobutamine echocardiography.12 The group included those with atypical symptoms in whom coronary disease is excluded, as well as those with complex disease who require risk stratification, which allowed study of variation in response between those with and without vascular disease. microparticles, cell-derived ■ vascular diseases In This Issue, see p 2 Editorial, see p 15 Methods Expanded Methods can be found in the Online Data Supplement. Sample Collection and Analysis Participants were recruited sequentially from patients undergoing dobutamine stress echocardiography (DSE) at the John Radcliffe Hospital, Oxford. Citrate blood samples were taken peripherally before, immediately after, and 1 hour after DSE.13 Circulating microparticles were measured by flow cytometry.14 Functional effect was assessed by procoagulant assay. Cardiovascular Disease Assessment DSE identified patients with coronary disease sufficient to cause acute myocardial ischemia to study microparticle response related to ischemia. Medical history and coronary angiography identified patients with vascular disease to determine whether differences in microparticle response relate to vascular disease or ischemia. Original received June 3, 2013; revision received October 16, 2013; accepted October 18, 2013. In September 2013, the average time from submission to first decision for all original research papers submitted to Circulation Research was 13.2 days. From the Oxford Cardiovascular Clinical Research Facility, University of Oxford, Oxford, United Kingdom (D.A., E.L., L.N., A.J.L., E.F.D., P.L.); and Department of Clinical Immunology, Oxford University Hospitals NHS Trust, Oxford, United Kingdom (L.V.A., B.F.). *These authors contributed equally to this work. The online-only Data Supplement is available with this article at http://circres.ahajournals.org/lookup/suppl/doi:10.1161/CIRCRESAHA. 114.301904/-/DC1. Correspondence to Paul Leeson, PhD, FRCP, Oxford Cardiovascular Clinical Research Facility, John Radcliffe Hospital, Oxford OX39DU, United Kingdom. E-mail paul.leeson@cardiov.ox.ac.uk © 2013 American Heart Association, Inc. Circulation Research is available at http://circres.ahajournals.org DOI: 10.1161/CIRCRESAHA.114.301904 109 110 Circulation Research January 3, 2014 Nonstandard Abbreviations and Acronyms DSE EMP dobutamine stress echocardiography endothelial cell-derived microparticle Statistical Analysis Statistical analysis is detailed in the online-only Data Supplement. Results Microparticles and Cardiac Stress One hundred nineteen participants took part, and 107 had measurements 1 hour after DSE. Immediately after DSE, procoagulant, platelet, erythrocyte, and CD31+CD41− endothelial cell–derived microparticle (EMP) levels rose significantly. One hour later, procoagulant and platelet microparticle levels had returned to baseline. Erythrocyte-derived microparticles had also started to decrease, and CD31+CD41− EMPs had fallen below baseline (Figure 1). Other microparticles did not change during stress (data not shown). The rise in microparticles was correlated with an increase in procoagulant activity, consistent with a clinically relevant functional effect (Figure 2C). Microparticles and Myocardial Ischemia There were 94 negative and 25 positive DSEs. Participants with a positive DSE were significantly older and had slightly lower cholesterol, but other clinical and echocardiographic variables were similar (Online Table I). Baseline microparticle levels did not differ between groups (Online Table II). However, procoagulant, platelet, erythrocyte, and CD31+CD41− EMPs increased in participants after a negative DSE (Figure 2A), with no change up to 1 hour in those with a positive DSE. Adjustment for risk factors and medication by regression analysis did not alter this finding. Microparticles and Vascular Disease To investigate whether this lack of response related to myocardial ischemia or underlying vascular disease, we compared microparticle release in 72 participants with a negative DSE without evidence of vascular disease with microparticle release in 11 participants with known vascular disease. Procoagulant, platelet, and erythrocyte-derived microparticles had not increased in participants with vascular disease (Figure 2B). In 14 participants who subsequently underwent coronary angiography, procoagulant, platelet, and erythrocyte-derived microparticles had increased only in individuals with normal coronary arteries (Figure 3A). Interestingly, a stress-induced increase in procoagulant and erythrocyte-derived microparticles had occurred in a patient with a positive DSE subsequently found to have normal coronaries, and no change in microparticles had occurred in a patient with a negative DSE found to have coronary disease (Figure 3B). Discussion We demonstrate a dynamic rapid rise and fall in a broad range of circulating microparticles in response to cardiac stress. Interestingly, this response was not apparent in those who developed myocardial ischemia, which seemed to relate to their underlying vascular disease because no increase was seen in those with a negative stress echo but known vascular disease. Subsequent analysis based on angiographic disease supported these findings. Our findings are consistent with previous reports of a trend for platelet-derived microparticles to increase after DSE,15 as well as significant rises in healthy individuals after exercise3,4 and a high-fat meal.16 Our analysis shows that procoagulant, erythrocyte, and platelet-derived microparticle levels are related, and all elevate immediately after DSE. Microparticle levels depend on speed of clearance mechanism, currently thought to involve direct receptor binding of liver or spleen phagocytes to phosphatidylserine or opsonization proteins Figure 1. Dot plots (median with interquartile range) of annexin V+ (A), platelet (B), erythrocyte (C), and endothelial cell microparticles (MP; D) at time points before dobutamine stress echocardiography (DSE), immediately after DSE, and 1 after DSE. EMP indicates endothelial cell–derived MP; and PMP, platelet-derived MP. Augustine et al Cardiac Stress–Induced Microparticle Release 111 Figure 2. Dot plots (median with interquartile range) of annexin V+, platelet, erythrocyte, and endothelial cell microparticles (MP) in negative dobutamine stress echocardiography (DSE) and positive DSE patients before and immediately after DSE (A) and in patients with a negative DSE and no vascular disease or vascular disease before and immediately after DSE (B). Microparticle procoagulant activity by Zymuphen assay (C). EMP indicates endothelial cell–derived MP; PMP, platelet-derived MP; and RBC, red blood cell. on the microparticles.17,18 Platelet-derived microparticle levels are known to fall rapidly after injection into rabbits19 and within 30 minutes after infusion in mice,17 but few studies have investigated human clearance.20 We found that, within 1 hour, elevated circulating procoagulant, platelet, and EMPs are significantly reduced. Clearance rate differed by cellular origin so that erythrocyte-derived microparticles had not declined as much and 112 Circulation Research January 3, 2014 Figure 3. Dot plots (median with interquartile range) of annexin V+ microparticles (MPs), CD31+CD41+ platelet-derived MPs (PMPs), glycophorin A+ erythrocyte-derived microparticles, and CD31+CD41− endothelial cell–derived MPs (EMPs) before and immediately after dobutamine stress echocardiography (DSE) in participants with a confirmed diagnosis by angiogram (A). Percentage change in microparticle levels during DSE in a false-positive and a false-negative participant (B). RBC indicates red blood cell. CD31+CD41− EMPs fell below baseline. Because EMPs carry von Willebrand factor,21 they present a potential thrombotic risk, which might explain their apparently more rapid clearance mechanism. However, EMP response to cardiac stress, in general, differed. CD31+CD41− EMPs, indicative of endothelial apoptosis,22 increased, but with a relatively small proportional change. There was no change in CD62E+ EMPs, a marker of endothelial cell activation,22 or CD144+ EMPs, an independent predictor of future cardiovascular events.23 Lower concentrations of CD31+CD41− EMPs or the standard negative staining approach,24,25 which excludes platelet-derived microparticles but may lead to inclusion of leukocyte-derived microparticles, could explain this. Alternatively, CD31+CD41− EMP release in response to stress may have distinct characteristics because different EMP subpopulations are known to be released in response to different triggers.22 Although we found no difference in EMP levels between those with and without vascular disease, EMP levels are an independent predictor of cardiovascular events in coronary patients26 and in those with end-stage renal failure,27 so EMP stress response in vascular patients may vary from other cellular microparticles. This significant variability in the degree of change in microparticle levels between individuals after cardiac stress raises the interesting possibility that this could be a predictive biomarker.28 One patient with a normal DSE subsequently had an out-of-hospital arrest and had no microparticle rise during stress. However, lack of microparticle release was an indicator of vascular disease rather than ischemia. A larger study with more extensive angiographic and clinical follow-up will be required to determine prognostic significance of this dynamic response and allows for calculation of positive and negative predictive values. Investigation of dynamic microparticle release from other cells, in particular cardiomyocytes, may be of interest as markers of ischemic burden. In summary, we demonstrate, in a large cohort, that procoagulant, platelet, erythrocyte, and endothelial-derived microparticles are released and cleared rapidly in response to cardiac stress. This dynamic response was not evident in the group of subjects with vascular disease. Although provisional pending replication, these observations raise the possibility that microparticle release is a protective mechanism to remove cellular stress signals, which is diminished in those with vascular disease. Interventions to enhance release and clearance of microparticles may be relevant for disease prevention. Sources of Funding The work was supported by grants to P. Leeson from the British Heart Foundation (FS/06/024 and FS/11/65/28865). D. Augustine was supported by the Engineering and Physical Science Research Council, and L.V. Ayers was supported by a National Institute of Health Research Healthcare Science Research Fellowship and the Oxford National Institute for Health Research Biomedical Research Centre. Disclosures None. References 1. Baron M, Boulanger CM, Staels B, Tailleux A. Cell-derived microparticles in atherosclerosis: biomarkers and targets for pharmacological modulation? J Cell Mol Med. 2012;16:1365–1376. 2.Andrews RK, Berndt MC. Microparticles facilitate neutrophil/platelet crosstalk. Blood. 2008;112:2174–2175. 3. Maruyama K, Kadono T, Morishita E. Plasma levels of platelet-derived microparticles are increased after anaerobic exercise in healthy subjects. J Atheroscler Thromb. 2012;19:585–587. 4.Chaar V, Romana M, Tripette J, Broquere C, Huisse MG, Hue O, Hardy-Dessources MD, Connes P. Effect of strenuous physical exercise on circulating cell-derived microparticles. Clin Hemorheol Microcirc. 2011;47:15–25. 5. VanWijk MJ, VanBavel E, Sturk A, Nieuwland R. Microparticles in cardiovascular diseases. Cardiovasc Res. 2003;59:277–287. Augustine et al Cardiac Stress–Induced Microparticle Release 113 6. Dignat-George F, Boulanger CM. The many faces of endothelial microparticles. Arterioscler Thromb Vasc Biol. 2011;31:27–33. 7. Bulut D, Tüns H, Mügge A. CD31+/Annexin V+ microparticles in healthy offsprings of patients with coronary artery disease. Eur J Clin Invest. 2009;39:17–22. 8. Nozaki T, Sugiyama S, Koga H, Sugamura K, Ohba K, Matsuzawa Y, Sumida H, Matsui K, Jinnouchi H, Ogawa H. Significance of a multiple biomarkers strategy including endothelial dysfunction to improve risk stratification for cardiovascular events in patients at high risk for coronary heart disease. J Am Coll Cardiol. 2009;54:601–608. 9.Ueba T, Nomura S, Inami N, Nishikawa T, Kajiwara M, Iwata R, Yamashita K. Plasma level of platelet-derived microparticles is associated with coronary heart disease risk score in healthy men. J Atheroscler Thromb. 2010;17:342–349. 10.Tushuizen ME, Diamant M, Sturk A, Nieuwland R. Cell-derived microparticles in the pathogenesis of cardiovascular disease: friend or foe? Arterioscler Thromb Vasc Biol. 2011;31:4–9. 11.Bernal-Mizrachi L, Jy W, Fierro C, Macdonough R, Velazques HA, Purow J, Jimenez JJ, Horstman LL, Ferreira A, de Marchena E, Ahn YS. Endothelial microparticles correlate with high-risk angiographic lesions in acute coronary syndromes. Int J Cardiol. 2004;97:439–446. 12. Marcovitz PA, Armstrong WF. Accuracy of dobutamine stress echocardiography in detecting coronary artery disease. Am J Cardiol. 1992;69:1269–1273. 13.Sicari R, Nihoyannopoulos P, Evangelista A, Kasprzak J, Lancellotti P, Poldermans D, Voigt JU, Zamorano JL; European Association of Echocardiography. Stress echocardiography expert consensus statement: European Association of Echocardiography (EAE) (a registered branch of the ESC). Eur J Echocardiogr. 2008;9:415–437. 14.Ayers L, Kohler M, Harrison P, Sargent I, Dragovic R, Schaap M, Nieuwland R, Brooks SA, Ferry B. Measurement of circulating cell-derived microparticles by flow cytometry: sources of variability within the assay. Thromb Res. 2011;127:370–377. 15.Galloway MT, Paglieroni TG, Wun T, Arena FJ, Lewis WR. Platelet activation during dobutamine stress echocardiography. Am Heart J. 1998;135:888–900. 16. Ferreira AC, Peter AA, Mendez AJ, Jimenez JJ, Mauro LM, Chirinos JA, Ghany R, Virani S, Garcia S, Horstman LL, Purow J, Jy W, Ahn YS, de Marchena E. Postprandial hypertriglyceridemia increases circulating levels of endothelial cell microparticles. Circulation. 2004;110:3599–3603. 17. Flaumenhaft R. Formation and fate of platelet microparticles. Blood Cells Mol Dis. 2006;36:182–187. 18. Davila M, Amirkhosravi A, Coll E, Desai H, Robles L, Colon J, Baker CH, Francis JL. Tissue factor-bearing microparticles derived from tumor cells: impact on coagulation activation. J Thromb Haemost. 2008;6: 1517–1524. 19. Rand ML, Wang H, Bang KW, Packham MA, Freedman J. Rapid clearance of procoagulant platelet-derived microparticles from the circulation of rabbits. J Thromb Haemost. 2006;4:1621–1623. 20. Rank A, Nieuwland R, Crispin A, Grützner S, Iberer M, Toth B, Pihusch R. Clearance of platelet microparticles in vivo. Platelets. 2011;22: 111–116. 21. Jy W, Jimenez JJ, Mauro LM, Horstman LL, Cheng P, Ahn ER, Bidot CJ, Ahn YS. Endothelial microparticles induce formation of platelet aggregates via a von Willebrand factor/ristocetin dependent pathway, rendering them resistant to dissociation. J Thromb Haemost. 2005;3:1301–1308. 22.Jimenez JJ, Jy W, Mauro LM, Soderland C, Horstman LL, Ahn YS. Endothelial cells release phenotypically and quantitatively distinct microparticles in activation and apoptosis. Thromb Res. 2003;109:175–180. 23. Nozaki T, Sugiyama S, Sugamura K, Ohba K, Matsuzawa Y, Konishi M, Matsubara J, Akiyama E, Sumida H, Matsui K, Jinnouchi H, Ogawa H. Prognostic value of endothelial microparticles in patients with heart failure. Eur J Heart Fail. 2010;12:1223–1228. 24.Periard D, Boulanger CM, Eyer S, Amabile N, Pugin P, Gerschheimer C, Hayoz D. Are circulating endothelial-derived and platelet-derived microparticles a pathogenic factor in the cisplatin-induced stroke? Stroke. 2007;38:1636–1638. 25. Takahashi T, Kobayashi S, Fujino N, Suzuki T, Ota C, He M, Yamada M, Suzuki S, Yanai M, Kurosawa S, Yamaya M, Kubo H. Increased circulating endothelial microparticles in COPD patients: a potential biomarker for COPD exacerbation susceptibility. Thorax. 2012;67:1067–1074. 26.Sinning JM, Losch J, Walenta K, Böhm M, Nickenig G, Werner N. Circulating CD31+/Annexin V+ microparticles correlate with cardiovascular outcomes. Eur Heart J. 2011;32:2034–2041. 27. Amabile N, Guérin AP, Tedgui A, Boulanger CM, London GM. Predictive value of circulating endothelial microparticles for cardiovascular mortality in end-stage renal failure: a pilot study. Nephrol Dial Transplant. 2012;27: 1873–1880. 28. Ikonomidis I, Athanassopoulos G, Stamatelopoulos K, Lekakis J, Revela I, Venetsanou K, Marinou M, Monaco C, Cokkinos DV, Nihoyannopoulos P. Additive prognostic value of interleukin-6 at peak phase of dobutamine stress echocardiography in patients with coronary artery disease. A 6-year follow-up study. Am Heart J. 2008;156:269–276. Novelty and Significance What Is Known? • Microparticles are small membrane vesicles, which can be stimulated to bud off from cells into the circulation and can trigger a range of biological responses. • The cellular origin and quantity of circulating microparticles can be measured. • Certain subtypes have been shown to be elevated in those with cardiovascular disease but also in healthy individuals after exercise. What New Information Does This Article Contribute? • Cardiac stress induces a rapid dynamic increase in a broad range of circulating microparticles. • These microparticles are then cleared from the circulation during the next hour. • The stress-induced rise seems to be a normal physiological response that is diminished in those with vascular disease. Microparticles are subcellular membrane vesicles that bud off from cells into the circulation in response to different stimuli and can be identified, and quantified, based on markers on their surface. Although circulating levels of certain microparticles are increased in people with cardiovascular disease, exercise has also been found to increase levels in healthy subjects. This study investigated whether microparticle release is a normal phenomenon in response to cardiac stress, what type of microparticles are released, how quickly they then clear from the circulation, and whether vascular disease is associated with a different response. A dynamic rapid rise in a broad range of circulating microparticles was demonstrated in patients undergoing a standardized cardiac stress protocol. These microparticles then cleared from the circulation within an hour. Interestingly, this dynamic rise and fall was not apparent in those who had vascular disease, diagnosed based on their medical history and, when available, evidence from coronary angiography. These observations raise the possibility that stress-induced microparticle release may be a biomarker of a physiological response to remove cellular stress signals, which is diminished in those with vascular disease. Interventions to enhance both release and clearance of microparticles may be relevant for disease prevention.