Cost of Gestational Diabetes Mellitus Presented by: Yaozhu (Juliette) Chen, MPA
 Chen, MPA")
HEALTH CARE AND HUMAN SERVICES POLICY, RESEARCH, AND CONSULTING - WITH REAL-WORLD PERSPECTIVE.
Cost of Gestational Diabetes Mellitus
Presented by: Yaozhu (Juliette) Chen, MPA
June 28, 2009
Acknowledgement
Co-authors
Tim Dall, MS
Grace Yang, MPA
William Quick, MD, FACP
Yiduo Zhang, PhD
Alan Baldwin, MS
Jane Moran, MD
Victoria Moore, BS
Navita Sahai, BA
Funded by National Changing Diabetes Program (NCDP)
Citation
Chen Y, Quick WW, Yang W, et al. Cost of Gestational Diabetes
Mellitus in the U.S. in 2007. Population Health Management. June
2009, 12(3): 165-174. www.lewin.com
2
Overview
Cost of Gestational Diabetes Mellitus (GDM) model
Research design
Data sources
Analytical specifics
Findings
Strengths and limitations
Policy implications www.lewin.com
3
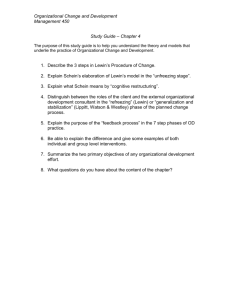
Conceptual Framework for the Cost of GDM
www.lewin.com
4
Research Design
Prevalence-based approach
Focus on medical costs
Target pregnancies that result in delivery
Populations to analyze the health care use
Mothers: 9 months preceding the delivery through 12 months following the delivery
Newborns: first 12 months of life
Service delivery setting
Hospital inpatient and outpatient
Emergency department
Physician office
Attribute risk fractions of GDM www.lewin.com
5
Data Sources
Prevalence
National Hospital Discharge Survey (NHDS) 2003-2005
Case identification: ICD-9-CM code 648.8 at delivery
Health care services
Hospital inpatient days: Nationwide Inpatient Sample (NIS) 2005
Physician office visits: National Ambulatory Medical Care Survey
(NAMCS) 2000-2005
Emergency and outpatient department visits: National Hospital
Ambulatory Medical Care Survey (NHAMCS) 2000-2005
Pharmaceuticals: NAMCS and NHAMCS 2000-2005
Unit cost per medical event
NIS 2005 and Medical Expenditure Panel Survey (MEPS) 2003-2005
GDM induced increase in health care use
Ingenix Research Data Mart (RDM ), extracted 26,911 deliveries in
2005 and mothers were continuously enrolled in 2004-2006 www.lewin.com
6
Categories of Health Care Use and Costs
Associated with GDM
Direct treatment of GDM
Maternal outcomes (8 groups)
Cesarean delivery, polyhydramnios, urinary tract infection, amniotic cavity infection, preeclampsia and eclampsia, other hypertension complicating pregnancy, other pregnancy-related events, and all other maternal care events
Neonatal outcomes (10 groups)
Intrauterine hypoxia and birth asphyxia, macrosomia, endocrine and metabolic disturbances specific to the fetus and newborn, birth trauma due to long gestation and high birth weight, fetus or newborn affected by other complications of labor and delivery, respiratory distress syndrome, jaundice, congenital anomalies, other neonatal events, and all other neonatal care events www.lewin.com
7
Analytical Specifics
Etiological fraction method
Calculate difference in health care use for people with GDM compared to what their health care use would be in absence of GDM
Provide demographic-complication-setting specific estimates of the proportion of national health care use attributed to GDM
Apply fractions to generate the cost of GDM
Multiply fractions by estimates of national maternal and neonatal health care use and costs in 2007
Extrapolation and adjustments
U.S. population in 2007 using the Census Bureau population estimates
Cost estimates adjusted to 2007 dollars using medical component of consumer price index www.lewin.com
8
Formula to Calculate Etiological Fraction
ε
=
P ( RR d
×
P ( RR d
×
−
1)
ε: etiological fractions
P: GDM prevalence rates
RR: health care use rate ratios
c: complication groups of mothers and newborns d: demographic - mother’s age
(for maternal analysis) and newborn’s sex (for newborn analysis) o: outcome measures - hospital inpatient days, emergency visits, other ambulatory visits
(hospital outpatient visits and physician office visits), and pharmaceuticals www.lewin.com
9
Calculate Rate Ratios
Use a generalized linear model (GLM) to estimate a series of demographic-complication-setting specific rate ratios
With a Poisson distribution and a log link
Controlling for other determinants of health care use
Dichotomous control variables, indicating
Presence of GDM
Maternal age groups (for maternal analysis only)
<21,21-25,26-30,31-35, >35
Gender (for newborn analysis only)
Male and Female
Census region (Northeast, South, West, and Midwest)
Presence of maternal or perinatal complications www.lewin.com
10
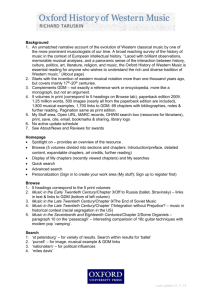
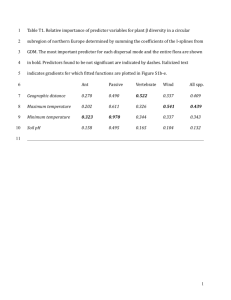
GDM Prevalence by Maternal Age, Race and
Ethnicity
10%
8%
6%
4%
2%
0%
16%
14%
12%
Age < 21 Age 21-25
NH White
Age 26-30
NH Black
Note: “NH” stands for Non-Hispanic.
Age 31-35
NH Other
Age > 35
Hispanic www.lewin.com
11
GDM Associated Health Care Use in 2007
U.S. Total Pregnant
Women and Their
Offspring
Incurred by Pregnant
Women with GDM and
Their Offspring
Health Resource Use
Mother
Unit (thousands)
Unit
(thousands)
Hospital Inpatient Days 17,423 838
Emergency Visits 3,808 170
Ambulatory Visits 41,438 1,958
Prescriptions 38,435 2,085
Newborn
Hospital Inpatient Days 18,969 873
Emergency Visits 169 8
Ambulatory Visits 5,372 248
Prescriptions 4,928 227
% U.S.
Total
Attributable to GDM
Unit
(thousands)
4.81% 269
4.47% 36
4.73% 651
5.43% 735
4.60% 28
4.63% 1
4.62% 30
4.61% 27
% U.S.
Total
1.54%
0.95%
1.57%
1.91%
0.15%
0.62%
0.56%
0.55% www.lewin.com
12
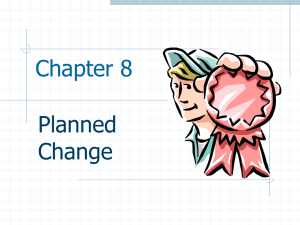
GDM Associated Medical Expenditures in 2007
U.S. Total
Pregnant Women and Their
Offspring
Incurred by Pregnant
Women with GDM and
Their Offspring
Medical Cost Dollars (millions)
Dollars
(millions) % U.S. Total
Mother
Hospital Inpatient $ 25,452 $ 1,260
Emergency Department $ 2,125 $ 92
Ambulatory Services $ 8,699 $ 418
Prescriptions $ 3,146 $ 171
Subtotal $ 39,423 $ 1,940
Newborn
Hospital Inpatient $ 24,287 $ 1,092
Emergency Department $ 100 $ 4
Ambulatory Services $ 1,566 $ 70
Prescriptions $ 416 $ 19
Subtotal $ 26,368 $ 1,185
Attributable to GDM
Dollars
(millions)
4.95% $ 386
4.31% $ 20
4.81% $ 130
5.43% $ 60
4.92% $ 596
4.50% $ 28
4.50% $ 1
4.48% $ 9
4.47% $ 2
4.50% $ 40
% U.S.
Total
1.52%
0.93%
1.49%
1.91%
1.51%
0.12%
0.70%
0.55%
0.53%
0.15%
Total (Mother and Newborn) $ 65,791 $ 3,125 4.75% $ 635 0.97%
Note: numbers may not add to totals because of rounding.
www.lewin.com
13
Other Findings
180,000 pregnancies are complicated by GDM every year
GDM induced per capita costs
$3,305 per pregnancy for mother
$209 per newborn in the first year of life
Who paid for the costs imposed by GDM?
Government programs (primarily Medicaid): 36%
Commercial payers: 56%
Self pay and charity care: 8% www.lewin.com
14
Study Strengths
A comprehensive list of pregnancy and newborn complications that the literature suggests may be associated with GDM
Use of multiple, nationally representative data sources
A large (n≈27,000) sample of women (and their newborns) with multiple years of medical claims data to analyze the impact of GDM on per capita care use
A standardized method that was recently used to calculate the national cost associated with pre-diabetes, undiagnosed diabetes, type 1 and type 2 diagnosed diabetes www.lewin.com
15
Study Limitations
Use of proprietary data source Ingenix RDM may over represent privately insured
Claims data tend to be less accurate than clinical data in condition identification
Estimates do not include
Intangible costs such as pain, suffering, and reduced quality of life
Indirect costs such as care provided by non-paid caregivers, increased time off from school, and reduced offspring’s performance in school
Long-term sequelae, e.g., higher risk of developing chronic diseases for both GDM mothers and their offspring www.lewin.com
16
Policy Implications
National economic burden of GDM potentially can be reduced by
Behavior change to prevent GDM
Early detection of GDM
Improved management among women diagnosed with GDM
Timely and appropriate treatment
Cost estimates of GDM help inform the business case for promoting women and children’s health
Impact of preventing and treating GDM
An opportunity of lifetime
Generational succession of obesity and type 2 diabetes www.lewin.com
17
The Lewin Group
3130 Fairview Park Drive
Suite 800
Falls Church, VA 22042
Main: (703) 269-5500 www.lewin.com
The Lewin Group | Health care and human services policy research and consulting | www.lewin.com
3130 Fairview Park Drive, Suite 800 • Falls Church, VA • 22042 • From North America, call toll free: 1-877-227-5042 • inquiry@lewin.com
The Lewin Group is an Ingenix Company. Ingenix, a wholly-owned subsidiary of UnitedHealth Group, was founded in 1996 to develop, acquire and integrate the world's best-in-class health care information technology capabilities. For more information, visit www.ingenix.com. The Lewin Group operates with editorial independence and provides its clients with the very best expert and impartial health care and human services policy research and consulting services. The Lewin Group and logo, Ingenix and the Ingenix logo are registered trademarks of Ingenix. All other brand or product names are trademarks or registered marks of their respective owners. Because we are continuously improving our products and services, Ingenix reserves the right to change specifications without prior notice.
Ingenix is an equal opportunity employer. Original © 2008 Ingenix. All Rights Reserved www.lewin.com
18