Markets and Medical Care: What Should We Have Learned About Cost Control?

Markets and Medical Care:
What Should We Have Learned
About Cost Control?
Joseph White Ph.D.
Luxenberg Family Professor
Case Western Reserve
University
Presented at the Annual
Research Meeting
Academy Health
June 3, 2007
Old Questions and New
Evidence
• How well have market forces worked?
• How have market forces worked?
• Judging from U.S. experience since 1993?
Key Attributes of The Market
• Entrepreneurial Pursuit of Income by
Providers and by Insurers
• Shopping for Services and Coverage by
Consumers or Their Agents
(Employers)
• Investment and Change Financed by
Access to Capital Markets (Debt and
Equity):
So Allocation of Capital Shapes the
System
Markets Should Only Help Access
Through Cost Control
• Access Requires Subsidies and
Markets Don’t Do Subsidies:
• “ Markets will distribute goods based on the distribution of purchasing power; they will not redistribute to or cross subsidize lower income people.” (Mark Pauly, 1998)
• But if markets made health care less expensive, subsidies would be easier to arrange. So markets could improve access through costs.
Quality Problems Involve
Measurement and Management
• To improve quality you need to be able to measure and so identify it.
• To improve quality, medical care organizations have to be managed better.
• Neither regulation nor market forces have much relevance to these problems. If they’re not solved, neither can help much.
• And shopping with price constraints is not in principle more helpful than choice without price constraints.
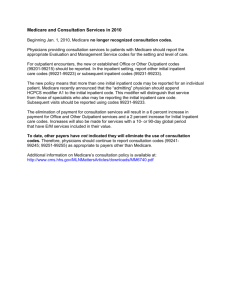
1970-
1993
1993-
1997
1997-
1999
1999-
2004
Years
Health Care Costs Per Capita
Percentage Growth Rates
All
Benefits
All
Benefits
Common
Benefits
Common
Benefits
MEDICARE PHI
10.9% 12.8% 10.7% 12.0%
7.6%
-0.2%
6.4%
4.3%
5.9%
9.5%
6.4%
1.4%
5.8%
2.6%
4.3%
8.6%
Two Meanings of “Managed
Care”
• Managing Treatments: Altering treatment decisions and so utilization, as with utilization review, risk-bearing gatekeeping, or the practice culture of the Kaiser model
• Selective contracting: Threatening to refuse to contract with a provider, so as to win lower prices. This requires that coverage be restricted to provider networks.
Estimated Health Plan Enrollment by
Plan Type: 1988 - 2005
HMO PPO POS YEAR Conventional
1988 73%
1993 46%
1996
1999
2002
2005
27%
4%
3%
3%
16%
21%
31%
28%
27%
21%
11%
26%
28%
39%
52%
61%
*
7%
14%
24%
18%
15%
Prices and Hospitalization
• “ Health plans, in early attempts at cost control, used fairly crude measures, including leveraging aggregated purchasing power to negotiate price discounts with providers. They turned their attention next to the potential for shifting service delivery from inpatient to outpatient settings.”
(HSChange Issue Brief 9, 1997)
• “the shift from inpatient to outpatient care has not gone unnoticed by hospital administrators. As care has shifted, so have charges. It is not uncommon to see outpatient charges exceeding the cost of an inpatient day…”
(Kongstvedt 1993)
The Pursuit of Market Share
• Aetna “sought to move as much enrollment as possible into the fully insured HMO, counting on aggessive provider discounts to control medical costs… The Aetna U.S. Healthcare managed care strategy relied above all else on massive scale, on millions in enrollment and billions in revenue to pressure physicians and hospitals to participate at low payment rates; cover the administrative overhead of utilization management; dilute adverse selection from weak underwriting; and spur continuous rounds of lower costs, lower premiums, and further growth.”
(Robinson 2004 in Health Affairs 23(2))
• Providers figured they had to get ahead of the wave
“to ensure they did not lose patients or revenue as beneficiaries moved into managed care”
(HSChange
Issue Brief 52, 2002)
• So “ panic-driven discounts ”
(Goldsmith in Issue Brief 10,
1997)
The Pushback
• In the case of Aetna, providers revolted,
“consolidating their local markets and demanding rate increases, litigating over delays in payment and denials in authorization, and, in some instances, simply walking away from HMO networks.”
(Robinson
2004)
• Wellpublicized showdowns, like St. Joseph’s and Pacificare in Orange County.
• By 2004: “plans have recognized and accepted their weaker position relative to providers”
(Hurley, Strunk and White 2004; Health
Affairs 23(2)
Summary of Reasons to Believe
Prices Were Crucial (1)
• The plans that most tightly managed treatment were never a large enough part of the system.
• Cost constraint occurred suddenly, across plan types, with little relationship to HMO market share.
• Even savings from reduced inpatient days required control of prices
Summary of Reasons to Think
Prices Were Crucial (2)
• Health System Change and other reports continually discussed change in terms of market power
• Comparisons of HMOs to PPOs found that the systems that managed treatments more had little if any cost advantage
• Analyses of the “Managed Care Backlash” show few effects from legislation or regulation. Instead, they report that plans abandoned treatment management measures due to their unpopularity in the market and perceived weak effects on costs.
“Health Plans” vs. Medicare
• “ having been in this world and worked for a plan trying to do this, I know what a disadvantage it is to have higher administrative costs, the marketing costs, and in the case of for-profit plans taxes and the like. So you’re behind before you even start in this game.” (Glenn Hackbarth, Dec
2003)
PPOs vs. Medicare
• Almost certainly, PPOs cannot get sustainable discounts from physicians or hospitals that approximate rates paid by
Medicare, as even the tightest HMO networks rarely approach Medicare’s administered prices. In that respect, Medicare is the
“mother of all PPOs” because it enjoys superior discounts over virtually all private payers. That the PPO will not be able to achieve the low administrative costs of traditional Medicare is a point conceded even by the proponents of PPOs.” Hurley, Strunk and White 2004 (Health Affairs 23:2)
“It’s the Prices, Stupid”
(With apologies to Anderson, Reinhardt, et al)
• Prices are the difference between the U.S. and other countries
• Prices were the reason for both private insurance successes and failures since 1993
• Prices are why Medicare has lower costs
• Controlling prices requires stable market power (at a minimum)
• Competing private insurers will only beat government-sponsored market power under very rare circumstances.