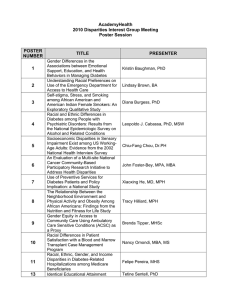
Unequal Treatment for Young Children? Racial and Ethnic Disparities in
advertisement

1 Unequal Treatment for Young Children? Racial and Ethnic Disparities in Early Childhood Health and Healthcare Glenn Flores, MD,1 Sandy Tomany, MS1 and Lynn Olson, PhD2 1Department of Pediatrics, Medical College of Wisconsin and Children’s Hospital of Wisconsin; 2Department of Practice & Research, American Academy of Pediatrics Funding: Robert Wood Johnson Foundation, AHRQ, Gerber Foundation 2 Background US experiencing demographic surge in minority children, particularly among youngest age groups By 2030 There will be more minority children than non-Hispanic white children 0-18 years old Among 0-5 year olds, minorities will outnumber non-Hispanic whites by 1.1 million As number and proportion of minority children grow, racial/ethnic disparities will take on even greater importance for pediatric providers 3 Background Recent reports by IOM and AHRQ called attention to tendency for US minorities to receive lower quality healthcare than whites, even after adjustment for access-related factors Although multiple studies document racial/ethnic disparities in adults, few studies have examined such disparities in children For example, only 5 of 103 studies in IOM’s extensive literature review specifically addressed disparities in children In particular, little known about whether younger children experience racial/ethnic disparities in healthcare 4 Study Aim To examine racial/ethnic disparities in early childhood health and healthcare using nationally representative sample Methods: Data Source- National Survey of Early Childhood Health (NSECH) Telephone survey in 2000 of national random sample of households with children 4-35 months old Oversampled households with black and Hispanic children Parent or guardian most responsible for child’s healthcare interviewed 2,068 interviews completed Interview completion rate = 79% Estimates based on sampling weights generalize to entire US population of children 4-35 months of age 5 6 Methods: Study Variables Variables examined included Selected sociodemographics Healthcare provider characteristics Use of health services Parental satisfaction with care Topics discussed with parents by providers Children’s race/ethnicity defined as white, black, or Hispanic by parental report ( “black” and “Hispanic” = NSECH terms) Because of insufficient sample sizes, subjects from other racial/ethnic groups excluded 7 Methods: Statistical Analysis Multivariable analyses performed to examine racial/ethnic differences after adjustment for Insurance coverage Survey language chosen by parent (English vs. Spanish) Health status Poverty Child’s age Parental educational attainment Characteristics: 4-35 Month-Old US Children in 2000 (NSECH) 8 White Black Hispanic Characteristic (N = 718) (N = 477) (N = 817) Mean age (mo) 19.5 19.5 18.7 0.22 Male sex (%) 53 48 51 0.34 Mother not high school grad (%) 11 26 49 <.001 Mother married (%) 81 32 58 <.001 Mother not employed (%) 45 39 53 <.001 Family income at/below poverty level (%) 13 49 48 <.001 Uninsured (%) Private insurance (%) Public insurance (%) 9 72 19 18 32 50 31 29 40 <.001 Child’s health excellent/very good (%) 90 79 72 <.001 P 9 Characteristics: Well Child Care Providers for 4-35 Month-Old US Children White Black Hispanic (N = 718) (N = 477) (N = 817) P Usual medical care in private practice 80% 68% 58% <.001 No specific well child care provider 52% 61% 63% <.001 Well child provider assigned to child 7% 14% 19% .01 Urban provider practice location 50% 66% 76% <.001 Well child care provider male 63% 51% 56% .03 Characteristic 10 Parental Satisfaction and Interactions with Well Child Care Providers: 4-35 Month-Old US Children White Black Hispanic (N = 718) (N = 477) (N = 817) P Never/only sometimes took time to understand child’s specific needs 10% 15% 30% <.001 Never/only sometimes respects parent as expert on child 14% 22% 25% <.001 Never/only sometimes understands parents’ childrearing preferences 35% 45% 46% <.001 Never/only sometimes asks how parent is feeling as parent 55% 53% 61% <.001 Did not spend enough time with child during last check-up (parent report) 11% 10% 17% .02 Parent very likely to recommend provider 84% 77% 60% <.001 Provider Characteristic 11 Topics Discussed with Parent by Well Child Care Providers: 4-35 Month-Old US Children White Black Hispanic (N = 718) (N = 477) (N = 817) P Violence in community 6% 14% 20% <.001 Smoking in household 72% 86% 85% <.001 Alcohol or drug use in household 35% 58% 65% <.001 Trouble paying for child’s needs 10% 18% 14% .001 Spouse/partner supports parenting style 34% 46% 46% <.001 Told parent developmental assessment done 47% 34% 43% .001 Immunizations 97% 96% 94% .16 Food/feeding issues 83% 83% 85% .78 Car seats 69% 77% 77% .001 Importance of reading to child 59% 69% 64% .006 Topic Use of Selected Health Services: 4-35 Month-Old US Children 12 White Black Hispanic (N = 718) (N = 477) (N = 817) Made age-appropriate # of well-child care visits (by AAP guidelines) 68% 70% 66% .55 Mean number of phone calls to doctor’s office in past year 4.2 3.1 2.0 <.001 1 or more ED visits in past year 32% 47% 41% <.001 1 or more hospital stays in past year 9% 17% 12% .005 Provider referred child to specialist 22% 17% 11% <.001 Measure P 13 Multivariate Analyses: Racial/Ethnic Disparities for 4-35 Month-Old US Children Odds Ratio (95% CI)* Measure Black Hispanic Uninsured 1.7 (1.02, 2.9) 2.3 (1.4, 3.8) Child’s health not excellent or very good 2.1 (1.3, 3.3) 1.3 (0.8, 2.1) Parent not very likely to recommend provider 1.2 (0.7, 2.2) 1.9 (1.1, 3.3) Provider never/sometimes understands child’s needs 1.4 (0.9, 2.3) 2.2 (1.4, 3.6) Provider never/sometimes understands parents’ childrearing preferences 1.5 (1.1, 2.2) 1.5 (1.1, 2.2) Mean # of calls to doctor’s office in past year -1.1 (-1.8,-0.3) -1.0 (-1.8,-0.2) One or more ED visits in past year 1.5 (1.1, 2.2) 1.4 (0.96, 2.0) Child not referred to specialist by provider 1.8 (1.1, 2.9) 1.7 (1.1, 2.8) *Reference group: white children 14 Multivariate Analyses: Racial/Ethnic Disparities for 4-35 Month-Old US Children Odds Ratio (95% CI)* Topic Discussed with Parent by Provider Black Hispanic Violence in community 2.2 (1.1, 4.4) 2.3 (1.2, 4.4) Smoking in household 1.9 (1.2, 2.8) 1.5 (0.9, 2.3) Use of alcohol or drugs in household 2.0 (1.4, 2.8) 1.6 (1.1, 2.3) Trouble paying for child’s needs 1.7 (1.03, 2.8) 1.3 (0.8, 2.1) Spouse/partner supports parenting efforts 1.6 (1.2, 2.3) 1.4 (1.0, 2.1) Childcare arrangements 2.0 (1.4, 2.8) 1.3 (0.9, 1.9) Importance of reading to child 1.6 (1.1, 2.3) 1.2 (0.8, 1.7) *Reference group: white children 15 Multivariate Analyses: Parent Survey Language Disparities for 4-35 Month-Old US Children Measure Odds Ratio (95% CI) Parent Survey in Spanish* Uninsured Child’s health not excellent or very good Usual place for medical care not private/group practice Provider never/sometimes understands child’s needs Provider discussed violence in community Provider discussed use of alcohol or drugs in household Parent told developmental assessment done by provider Mean # of calls to doctor’s office in past year Child not referred to specialist by provider *Reference group: parent completed survey in English 1.9 (1.2, 2.9) 2.8 (1.7, 4.6) 2.5 (1.6, 3.9) 1.9 (1.2, 3.2) 2.3 (1.4, 3.7) 2.8 (1.8, 4.4) 2.2 (1.4, 3.4) -2.0 (-2.8, -1.2) 2.7 (1.4, 5.2) 16 Conclusions Young minority children in US and those with Spanish-speaking parents experience multiple disparities in Insurance coverage Health status Parental satisfaction with well-child care providers Provider understanding of child’s needs and parents’ childrearing preferences Provider discussion of violence and alcohol/illicit drug use Parents’ calls to doctors’ offices Specialty referrals 17 Implications Greater insight needed about why such racial/ethnic disparities exist Study findings suggest priority areas for monitoring, quality assurance, and provider and system performance evaluation in health plans and systems providing healthcare to diverse pediatric populations Targeted educational interventions, such as cultural competency training, might help ensure equal treatment for all young children in pediatric visits