Reduction in Fatalities, Ambulance Calls, and Hospital
advertisement

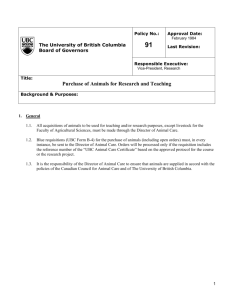
RESEARCH AND PRACTICE Reduction in Fatalities, Ambulance Calls, and Hospital Admissions for Road Trauma After Implementation of New Traffic Laws Jeffrey R. Brubacher, MD, MSc, Herbert Chan, PhD, Penelope Brasher, PhD, Shannon Erdelyi, BSc, Edi Desapriya, PhD, Mark Asbridge, PhD, Roy Purssell, MD, Scott Macdonald, PhD, Nadine Schuurman, PhD, and Ian Pike, PhD Motor vehicle crashes (MVCs) are a major public health problem that disproportionately affects youths and young adults.1 Worldwide, more than 3300 people per day are killed in road trauma,2 and many more are disabled. Crashes are caused by numerous factors, including faulty vehicles and poor road design, but the majority are attributed to driver-related factors, especially alcohol-impaired driving,3,4 speeding,5,6 and driver distraction.7,8 In Canada, driving with a blood alcohol concentration (BAC) of 0.08% or more is a federal criminal offense. Most provinces have regulations that allow for administrative sanctions (fines or license suspension) for drivers with a BAC of 0.05% or more. Speed limits are set by the provinces and enforced through administrative sanctions. Before September 2010, drunk drivers in British Columbia were subject to fines and administrative driving prohibitions of 24 hours for a BAC of 0.05% or more and of 90 days for a BAC of 0.08% or more or failure to provide a breath sample. The 90-day driving ban came into effect after a 21-day period that allowed the driver to find alternative means of transportation or to appeal the decision. There were no vehicle impoundments for drunk drivers. In addition to administrative penalties, drivers with a BAC of 0.08% or more and those who refused to provide a breath sample were subject to possible penalties under the Criminal Code of Canada. Before September 2010, the penalty for street racing was vehicle impoundment for 2 days for a 1st offense and for 30 days for 2nd and subsequent offenses in addition to fines and possible criminal code charges. In September 2010, British Columbia introduced harsher penalties for drunk drivers and for excessive speeding (> 40 km/h over the speed limit) as well as for drivers caught street racing or stunt driving. Under these laws, Objectives. We evaluated the public health benefits of traffic laws targeting speeding and drunk drivers (British Columbia, Canada, September 2010). Methods. We studied fatal crashes and ambulance dispatches and hospital admissions for road trauma, using interrupted time series with multiple nonequivalent comparison series. We determined estimates of effect using linear regression models incorporating an autoregressive integrated moving average error term. We used neighboring jurisdictions (Alberta, Saskatchewan, Washington State) as external controls. Results. In the 2 years after implementation of the new laws, significant decreases occurred in fatal crashes (21.0%; 95% confidence interval [CI] = 15.3, 26.4) and in hospital admissions (8.0%; 95% CI = 0.6, 14.9) and ambulance calls (7.2%; 95% CI = 1.1, 13.0) for road trauma. We found a very large reduction in alcohol-related fatal crashes (52.0%; 95% CI = 34.5, 69.5), and the benefits of the new laws are likely primarily the result of a reduction in drinking and driving. Conclusions. These findings suggest that laws calling for immediate sanctions for dangerous drivers can reduce road trauma and should be supported. (Am J Public Health. 2014;104:e89–e97. doi:10.2105/AJPH.2014.302068) which add to but do not replace the older laws, drivers with a BAC of 0.05% or more may be subject to license suspension of 3, 7, or 30 days; vehicle impoundment of 3, 7, or 30 days (discretionary with 3- or 7-day license suspensions, mandatory for 30-day license suspensions); and possible referral to remedial programs (including ignition interlock) for third-time offenders. Drivers with a BAC of 0.08% or more are subject to 30-day vehicle impoundment, 90-day license suspension, and possible referral to remedial programs (including ignition interlock). In addition, drunk drivers are subject to fees that include towing costs, vehicle storage costs, and a processing fee to have their license reinstated. License prohibitions and vehicle impoundments are issued immediately at the roadside on the basis of results of a handheld breathalyzer. The penalties for excessive speeding, street racing, and stunt driving include fees and mandatory vehicle impoundment of 7 to 60 days.9,10 Table 1 summarizes penalties for drinking and driving October 2014, Vol 104, No. 10 | American Journal of Public Health and for speeding and related offenses under the old versus new traffic laws. British Columbia’s laws were designed to deter drinking and driving by increasing the severity, certainty, and speed of punishment for drunk drivers with a BAC of 0.05% or more. Deterrence is effective in laws against traffic violations,11 and increased likelihood of punishment acts as a greater deterrent than increased severity.12,13 The speed with which a punishment is applied is an additional deterrent.14 For drivers with a BAC of 0.08% or more, the administrative sanctions under the new laws are actually less severe than those associated with a criminal code conviction for drunk driving. However, the new sanctions are applied immediately at roadside and are less subject to legal challenge, making punishment more swift and certain. Not all drunk drivers are deterred by threat of punishment,15 but through vehicle impoundment and license suspension, British Columbia’s new laws remove more dangerous drivers from the roads Brubacher et al. | Peer Reviewed | Research and Practice | e89 RESEARCH AND PRACTICE TABLE 1—Comparison of British Columbia’s Old and New Speeding and Street Racing Laws Penalties a Driving Offense After September 2010b,c Before September 2010 BAC level 0.0–0.049 12-h driving prohibition for drivers 0.05–0.079 (1st offense) 24-h driving prohibition with restricted license 3-d driving prohibition Possible 3-d vehicle impoundment Fees (£ $600) 0.05–0.079 (2nd offense within 5 y) 24-h driving prohibition 7-d driving prohibition Possible 7-d vehicle impoundment Fees (£ $780) 0.05–0.079 (3rd offense within 5 y)d 24-h driving prohibition 30-d driving prohibition 30-d vehicle impoundment Fees (£ $1330) ‡ 0.08 or refuses breath testd 90-d driving prohibition beginning 21 d after the offense (this 21-d period was to allow driver to arrange alternate transportation or to appeal the decision) 90-d driving prohibition (immediate) 30-d vehicle impoundment Fees (£ $1450) Possible Criminal Code of Canada charges Speeding and stunt driving Speeding £ 40 km over limit Fines and demerit points No change Speeding > 40 km per hour or stunt drivinge Fines and demerit points 7-d vehicle impoundment Speeding > 40 km per hour or stunt drivinge (second offense within 2 y) Fines and demerit points 30-d vehicle impoundment Fees £ $700 Speeding > 40 km per hour or stunt drivinge Fines and demerit points 60-d vehicle impoundment Fees £ $210 (first offense) Fees £ $1200 (third offense within 2 y) Street racing 1st offense Fines and demerit points (street racing only) 7-d vehicle impoundment 48-h vehicle impoundment Fees £ $210 2nd offense within 2 y Fines and demerit points (street racing only) 30-d vehicle impoundment 3rd and subsequent offense within 2 y 30-d vehicle impoundment Fines and demerit points (street racing only) Fees £ $700 60-d vehicle impoundment 30-d vehicle impoundment Fees $1200 Note. BAC = blood alcohol concentration; IRP = immediate roadside prohibitions. a All penalties that existed before September 2010 remain in effect. Starting September 2010, IRPs provided an additional tool for police to use at their discretion. b Since September 2010, police usually apply immediate penalties under the new laws. However, they still have the option of using the preexisting laws instead. Therefore, the 3 typical outcomes for drivers with BAC ‡ 0.05% or who refuse a breath test are as follows: (1) most get an IRP, (2) some get a 24-h (or 12-h) driving prohibition, and (3) some get a 90-d driving prohibition plus criminal code charges. c Note that the penalties for excessive speeding (> 40 km over limit), street racing, and stunt driving are identical under the new laws. d Drivers with 3 offenses for BAC = 0.05%–0.079% or 1 offense for BAC > 0.08% may be referred to the responsible driver program, the ignition interlock program, or both. e The new laws expanded the vehicle impound program to introduce and define “stunt driving,” something that was not specifically covered under the old laws. quicker. High-risk drunk drivers can also be mandated to undergo therapy, install an alcohol interlock device on their vehicle, or both. These laws were promoted through public awareness and educational campaigns and received considerable media coverage. Opinion and roadside surveys in 2012 found that majority of drivers were aware of the new measures16 and that public perception of police commitment to traffic enforcement had increased.17 During the first 12 months, British Columbia police used the new laws to issue 22 734 roadside license prohibitions for drinking and driving. At the same time, the number of criminal code convictions for impaired driving fell from 8221 per year in the e90 | Research and Practice | Peer Reviewed | Brubacher et al. 5 years preceding the new laws to 1853 in the subsequent 12 months (Figure 1). The new laws were associated with change in driver behavior. In the 2012 British Columbia roadside surveys, 6.5% of evening and nighttime drivers tested positive for BAC compared with 9.9% in 2010 before the new laws were introduced.16 Telephone surveys found that the percentage American Journal of Public Health | October 2014, Vol 104, No. 10 RESEARCH AND PRACTICE of British Columbia drivers reporting driving while over the legal limit was above the national average in 2009 and 2010 but fell below the national average in 2011 and 2012.18 The new laws included harsher penalties for excessive speeding but, unlike the case with drinking and driving, the number of sanctions for speeding or for excessive speeding did not increase (Figure 1). We previously reported a reduction in alcohol-related fatal crashes in the 2 years after introduction of British Columbia’s new laws.19 In this study, we investigated the effects of the new laws on total fatal crashes, hospital admissions, and ambulance calls. We drew on police, ambulance, and hospital data from British Columbia and on police data from adjacent jurisdictions in which similar legislative changes were not implemented. research ethics board. Briefly, we used an interrupted time-series approach to model the impact of the new laws on crashes and medical events. We assessed the intervention effects using a linear regression model with an autoregressive integrated moving average (ARIMA) error term. METHODS Data Sources We used deidentified administrative data and obtained approval from our institutional a Charges, No. Intervention 1500 Criminal code 90-day ADPs 90-day IRPs 3-, 7-, or 30-day IRPs 1000 500 0 2008 2009 2010 2011 Time Charges, No. b Intervention 20 000 15 000 10 000 2008 2009 2010 2011 Time c Charges, No. Intervention 1200 1000 800 600 400 2008 2009 2010 2011 Time Note. ADPs = administrative driving prohibitions; IRPs = immediate roadside prohibitions. In part (a), an abrupt decrease occurred in the number of criminal code charges and 90-day ADPs for impaired driving after the introduction of the new laws accompanied by an even greater increase in the number of IRPs issued under the new laws (note that, under the old laws, drivers with criminal code charges were typically also given a 90-day driving prohibition). In parts (b) and (c), the new laws were not associated with a change in the number of charges for speeding or for excessive speeding. However, under the new laws, excessive speeding resulted in mandatory vehicle impoundment for 7 days. FIGURE 1—Monthly charges for (a) impaired driving, (b) speeding, and (c) excessive speeding: British Columbia, September 2007–September 2011. October 2014, Vol 104, No. 10 | American Journal of Public Health We analyzed British Columbia data from MVC fatalities from police reports (2000--2012), hospital admissions (2005---2011), and ambulance calls (2004---2012). We obtained MVC fatality data from Alberta, Saskatchewan, and Washington State police reports (2000--2012). We did not have access to hospitalization or ambulance data from any jurisdiction other than British Columbia. Road fatalities. The British Columbia traffic accident system contains details of all policereported crashes in British Columbia, including factors that police believe contributed to the crash (e.g., speeding, impaired driving). The traffic accident system is reconciled with coroners’ data to ensure that it captures all fatal crashes (i.e., those who died on a public road and within 30 days of the crash). Nonfatal crashes may not be captured because police attendance at nonfatal crashes is discretionary. For this reason, we studied only fatal crashes. Fatal crashes related to alcohol or speeding were our outcome of interest, and fatal crashes unrelated to alcohol or speeding served as an internal control. Similarly, we obtained monthly counts of total fatal crashes and of fatal crashes involving alcohol or speeding from police reports of neighboring jurisdictions (Alberta, Saskatchewan, and Washington State). We used the analyses of these data as an external comparison to account for regional trends and conditions that might explain the observed effects of the new laws in British Columbia. Hospital admissions and ambulance dispatches. All hospital admissions in Canada are recorded in the Discharge Abstract Database, which includes mechanism of injury but has no information on factors that caused the crash. In this study, we used admissions for road trauma as a measure of hospital utilization by road injury victims in British Columbia. We defined “road trauma admissions” as those with International Classification of Diseases, 10th Revision (ICD-10),20 Brubacher et al. | Peer Reviewed | Research and Practice | e91 RESEARCH AND PRACTICE external cause of injury codes ranging from V02.1 (pedestrian injured in collision with 2or 3-wheeled motor vehicle, traffic accident) through V89.9 (person injured in unspecified vehicle accident). We also included sequelae of transport accidents (Y85, Y850, Y959). We excluded non---traffic accident events such as boarding or alighting from a vehicle, events that occurred on industrial premises, events that did not involve a motorized vehicle, and events in which the only vehicle involved was a streetcar, railway vehicle, specialized agricultural vehicle, airplane, or watercraft. We included traffic injury involving snowmobiles and all-terrain vehicles because these vehicles are subject to traffic laws when driven on a public road. We used hospital admissions for non-MVC trauma (i.e., all other injury codes) as controls. The British Columbia Ambulance Service provides emergency medical service for the entire province. Each call for emergency medical assistance is assigned 1 of 32 Advanced Medical Priority Dispatch System numbers using standardized questions. Multiple calls for the same event are combined into a single dispatch record. We used ambulance dispatches for traffic and transportation incidents (code 29) as a measure of ambulance service use by road injury victims. We used ambulance calls for non-MVC trauma as controls. Analysis For each outcome, we aggregated counts by month and converted them to rates. For crashes, rates were per 1 000 000 licensed drivers. Hospital admissions and ambulance calls included victims of all ages and were converted to rates per 1 000 000 British Columbia residents. We adjusted rates to account for the number of days in each month. We chose the time before intervention a priori to accommodate data availability and to exceed the recommended minimum number of observations required for time-series analyses.21 For the purpose of this study, we considered fatal crashes to be alcohol related if police cited alcohol involvement, alcohol suspected, or ability impaired by alcohol as a contributory factor for any driver of a motorized vehicle involved in the crash. We deemed crashes to be speeding related if police cited exceeding the speed limit, excessive speed, driving too fast for conditions, or unsafe speed as a contributory factor for any driver involved in the crash. Crashes with multiple contributory factors were included in all relevant analyses. We conducted subgroup analyses that excluded crashes involving both alcohol and speeding. We excluded cases in which relevant contributory factors were cited only for pedestrians or pedal cyclists. We analyzed event rates using an interrupted time-series approach. We fitted a multivariate linear regression model that included an indicator variable for the intervention (new law) effect, an internal control variable, and a seasonal ARIMA error term to control for seasonality, autocorrelation, and data instability. Internal controls served as a surrogate for unmeasured confounders and trends unrelated to the intervention. Controls were scaled and centered for model convergence. We originally included the effects of other events, such as a court challenge and temporary suspension of the new laws (November 2011),22 in the regression model. However, these events did not have a statistically significant effect on crash rates, and we omitted them from the final model. To complement ARIMA analyses, which estimate permanent changes in mean crash rate, we performed supplementary analyses to identify breakpoints (significant changes in the slope of the crash rate trendline) and to estimate the year in which any detected breakpoint occurred. To do this, we fitted regression models to annual crash rates with a segmented relationship for the yearly trend. The number of breakpoints was automatically selected but constrained to be less than 3.23,24 Data transformations were made to meet the assumptions of the model. First, we took the logarithm of crash rates to stabilize the variance when necessary. Second, we used differencing to achieve a stationary time series. If necessary, we calculated the difference from one period to the next to remove trends over time. We also used seasonal differencing to eliminate any strong seasonal patterns. An iterative procedure was used to identify the order of the ARIMA error model. We selected the initial model using a stepwise algorithm to minimize the corrected Akaike information criterion. We explored correlation structures via plots of the autocorrelation and partial autocorrelation functions. If the model e92 | Research and Practice | Peer Reviewed | Brubacher et al. fit was deemed inadequate, we used residual diagnostics to identify improved error structures. We selected the model with the lowest Akaike information criterion that also satisfied residual assumptions. The error model was not constrained to be the same across jurisdictions or outcomes. We fitted all models using conditional-sumof-squares to find starting values. Final estimates were obtained by maximum likelihood. We performed all regression analyses with R version 3.0.1 (R Foundation for Statistical Computing, Vienna, Austria). The intervention effect was treated as abrupt and permanent. We considered P < .05 to be statistically significant; all tests were 2-sided. RESULTS Between January 2000 and December 2012, 4507 fatal crashes occurred in British Columbia, including 1121 related to alcohol and 1600 related to speeding (163 to excessive speed). In 589 fatal crashes, both alcohol and speeding were involved. We found overall downward trends and seasonal patterns with peaks during summer months for both alcoholand speeding-related fatal crashes. Figure 2 shows monthly rates of fatal alcohol-related crashes over the study period. Table 2 summarizes the changes in occurrence rates for each outcome after the new laws went into effect. In the 24 months after British Columbia’s new laws were implemented, statistically significant reductions occurred in total fatal crashes and in fatal crashes related to alcohol and to speeding. Segmented regression analyses detected 1 breakpoint in the annual trend for alcohol-related fatal crash rates in 2010 (95% confidence interval [CI] = 2009, 2011). Breakpoints for speeding-related and all-cause fatal crash rates occurred in 2005, before the new laws. In subgroup analyses that excluded crashes involving both alcohol and speeding, we found a 46.5% reduction (95% CI = 23.1, 70.0) in alcohol-related crashes and a nonstatistically significant reduction of 21.1% (95% CI = –4.4, 46.7) in speeding-related crashes. During the same period, we observed a smaller reduction in alcohol-related fatal crashes in Alberta (32.7%) and much smaller reductions in Saskatchewan and American Journal of Public Health | October 2014, Vol 104, No. 10 RESEARCH AND PRACTICE Intervention Rate/1 000 000 Licensed Drivers 11 Fatal alcohol Fatal non−alcohol and non−speeding 10 9 8 7 6 5 4 3 2 1 0 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 Time Note. The vertical line indicates the first full month of implementation of the new laws in October 2010 (intervention effect = –1.41 fatal alcohol crashes/1 000 000 licensed drivers). The dotted curves represent the smoothed annual average of monthly rates from the fitted model for fatal alcohol crashes (dark curve) and from observed rates for fatal nonalcohol and nonspeeding crashes (light curve). FIGURE 2—Monthly alcohol-related fatal crash rate per 1 000 000 licensed drivers in British Columbia: January 2000–December 2012. Washington State (1.2% and 9.8%, respectively); the latter 2 were not statistically significant. Similarly, fatal crashes related to speeding decreased by 30.6% (95% CI = 17.0, 41.9) in Washington State. We found a smaller, nonsignificant decrease in fatal speeding crashes in Alberta (14.4%) and a trivial, non---statistically significant increase in Saskatchewan (2.5%). During the study period, British Columbia had 3553 hospital admissions and 32 225 ambulance calls for road trauma per year. Monthly rates of road trauma---related hospital admissions and ambulance calls are illustrated in Figures 3 and 4. We found an 8.0% (95% CI = 0.6, 14.9) reduction in hospital admissions and a 7.2% (95% CI = 1.1, 13.0) reduction in ambulance calls attributable to road trauma. DISCUSSION British Columbia’s new traffic laws were associated with decreases in fatal crashes (21.0%) and in hospital admissions (8.0%) and ambulance calls (7.2%) for road trauma, corresponding to monthly decreases of 2.21 fatal crashes per 1 000 000 drivers and 5.71 hospital admissions and 47.29 ambulance dispatches per 1 000 000 residents. Our findings of reductions not only in fatal crashes but also in ambulance calls and hospital admissions for road trauma strengthen the conclusion that British Columbia’s laws were effective in reducing road trauma. An alternate explanation is that these benefits are attributable to factors other than the new laws. We feel that this is unlikely for several reasons. First, we used internal controls to account for trends in need for trauma care or the number of fatal crashes. Second, with the exception of fines for drivers using cell phones (February 2010), British Columbia did not introduce any other significant traffic laws or policy changes in 2010 or 2011. The cell phone laws are unlikely to have had a significant impact on crash fatality rates because an analysis of distraction-related fatal crashes (not shown) showed no intervention effect. Furthermore, only 11 crash fatalities were attributed to use of electronic equipment between 2004 and 2012. Finally, we looked at crash fatality outcomes in neighboring jurisdictions and, with October 2014, Vol 104, No. 10 | American Journal of Public Health the exception of a probable spillover effect in Alberta, found no evidence of a reduction in total fatal crashes. Another possible explanation for our findings is that changes in reporting practice occurred that coincided with implementation of the new traffic laws. Police reports, in particular, may be affected by changes in reporting practice because police do not report all crashes,25,26 and police classification of the cause of crashes may be somewhat subjective. However, we found no evidence of a change in police reporting practice around the time of this study. Moreover, we studied only fatal crashes, which police are obligated to investigate and which are reconciled with coroners’ data to ensure no cases are missed. In addition, we found reductions in outcomes reported from 3 independent sources (police, ambulance, and hospital). Ambulance dispatch reports and hospital admissions for road trauma capture all events that are correctly classified, and we found no evidence of a change in reporting of these events. In particular, the Advanced Medical Priority Dispatch System codes used to classify ambulance dispatches and the ICD-10, injury codes for hospital admissions had not changed during the time of the study. Considering all these factors, our findings are highly unlikely to be explained by changes in reporting practice. Other researchers have also found that both criminal and administrative traffic laws reduce drunk driving fatalities. Asbridge et al. studied drunk driving fatalities and found an 18% reduction after Canada criminalized driving with a BAC of 0.08% or more in 196627 and a 14.5% reduction after Ontario implemented license suspensions for drivers with a BAC of 0.08% or more.28 In a study of US state laws, Wagenaar and Maldonado-Molina29 found that administrative license suspension reduced alcohol-related fatal crash involvement by 5%, whereas postconviction policies (e.g., mandatory jail time for those convicted of driving while impaired) had no discernible effects. Similarly, Traynor30 reviewed US traffic laws and found that states with more restrictive laws regulating teen driving and driving under the influence had lower road fatality rates. The benefits of British Columbia’s new laws are likely primarily the result of prevention of crashes caused by drinking and driving. Brubacher et al. | Peer Reviewed | Research and Practice | e93 RESEARCH AND PRACTICE TABLE 2—Effects of the New British Columbia Legislation Intervention Effect Error Model Estimate (SE)a P % Change (95% CI) Change in Monthly Rate per 1 000 000 British Columbia ARIMA (0,0,0)(2,0,0)12 –0.236 (0.036)b < .001 –21.0 (–26.4, –15.3) –2.21 Alberta Saskatchewan ARIMA (0,0,0)(3,1,1)12 ARIMA (0,0,0)(0,1,1)12 –0.140 (0.035)b 0.087 (0.892) < .001 .922 –13.1 (–18.9, –6.9) 0.6 (–10.7, 11.8) –1.55 0.09 Washington State ARIMA (3,0,0)(1,1,1)12 –0.549 (0.477) .25 –5.7 (–15.4, 4.0) –0.55 British Columbia ARIMA (2,0,0)(0,1,1)12 –1.408 (0.241) < .001 –52.0 (–69.5, –34.5) –1.41 Alberta ARIMA (0,0,0)(0,1,1)12 –0.396 (0.103)b < .001 –32.7 (–45.0, –17.6) –1.03 Saskatchewan ARIMA (0,0,0)(1,1,1)12 –0.069 (0.840) .935 –1.2 (–29.8, 27.4) –0.07 Washington State ARIMA (0,0,3)(0,1,1)12 –0.374 (0.344) .276 –9.8 (–27.4, 7.8) –0.37 –46.5 (–70.0, –23.1) –0.59 –24.3 (–48.7, 0.1) –0.44 Event All-cause fatal MVCs Alcohol-related fatal MVCs Alcohol-only related fatal MVCs British Columbia Normal –0.594 (0.153) < .001 Alberta ARIMA (2,0,0) –0.436 (0.224) .051 Saskatchewan ARIMA (0,0,0)(2,0,2)12 –0.214 (0.571) .708 –6.4 (–39.9, 27.1) –0.21 Washington State ARIMA (0,0,2)(0,1,1)12 –0.139 (0.197) .48 –7.7 (–29.1, 13.7) –0.14 British Columbia ARIMA (0,0,0)(2,0,0)12 –1.264 (0.279) < .001 –33.3 (–47.7, –18.9) –1.26 Alberta ARIMA (0,0,0)(0,0,1)12 –0.156 (0.091)b .085 –14.4 (–28.4, 2.2) –0.45 Saskatchewan Washington State ARIMA (0,0,6)(0,1,1)12 ARIMA (1,0,0)(1,0,1)12 0.090 (0.511) –0.365 (0.091)b .861 < .001 2.5 (–25.1, 30.1) –30.6 (–41.9, –17.0) 0.09 –1.13 Speeding-related fatal MVCs Speeding-only-related fatal MVCs British Columbia ARIMA (0,0,2)(2,0,0)12 –0.500 (0.308) .105 Alberta Normal –0.006 (0.181) .972 –21.1 (–46.7, 4.4) –0.4 (–21.0, 20.3) –0.01 –0.50 Washington State Normal –0.277 (0.115)b .016 –24.2 (–39.5, –5.0) –0.41 Road trauma related hospital admissions: British Columbia ARIMA (2,1,1)(0,1,1)12 –0.083 (0.040)b .036 –8.0 (–14.9, –0.6) –5.71 Road trauma related ambulance calls: British Columbia ARIMA (0,1,1)(3,1,1)12 –0.075 (0.033)b .022 –7.2 (–13.0, –1.1) –47.29 Note. ARIMA = autoregressive integrated moving average; CI = confidence interval; MVC = motor vehicle crash. a Estimates are expressed in monthly rate per 1 000 000 or, if the data were log-transformed, as log rate per 1 000 000. In all cases, the estimated effect is also expressed as % change and as change in monthly rate per 1 000 000. b Data were log-transformed. Consistent with this premise, we found a marked reduction (52.0%) in fatal alcoholrelated crashes. The segmented regression analysis finding that alcohol-related fatal crashes began to decline more rapidly in 2010 strengthens the evidence linking the new law to a reduction in alcohol-related MVC fatalities. Neither Saskatchewan nor Washington had declines in fatal alcohol-related crashes. Alberta, however, had a 32.7% reduction in fatal alcohol-related crashes that we attribute to a spillover effect from the changes in British Columbia. Spillover effects are common in studies of law and public policy and are closely related to the degree of population mobility between jurisdictions.31 At the time British Columbia’s new laws were put into effect, Alberta politicians were debating similar laws.32 In December 2011, in an example of policy diffusion,33---35 Alberta passed laws with immediate roadside penalties for drunk drivers. Alberta’s new laws were put into effect incrementally between July and September 2012. It is not surprising that British Columbia’s laws received considerable media coverage in Alberta, with headings such as “Alta. May Stiffen Drinking and Driving Laws”32 and “B.C. Drunk Driving Law Sobers Alberta.”36 Many Albertans likely changed their drinking and driving behavior as a result of press coverage. In addition, several municipalities in Alberta have programs that encourage citizens e94 | Research and Practice | Peer Reviewed | Brubacher et al. to report impaired drivers.37,38 Increased news coverage of drinking and driving may have encouraged greater participation in those programs. Furthermore, the adjacent nature of the 2 provinces, and easy migration of workers between British Columbia and Alberta, suggests that many drivers might have carried their knowledge of British Columbia laws into Alberta either from habit or from not knowing the policy differences between the 2 provinces. Finally, it is possible that Alberta police informally increased their own enforcement efforts in response to reports from British Columbia. British Columbia’s new laws also targeted speeding, with harsher penalties for excessive speeding, street racing, and stunt driving. We American Journal of Public Health | October 2014, Vol 104, No. 10 RESEARCH AND PRACTICE a Rate/1 000 000 BC Residents Intervention 850 800 750 700 650 600 2005 2006 2007 2008 2009 2010 2011 2012 Time b Rate/1 000 000 BC Residents Intervention 90 80 70 60 50 40 30 2005 2006 2007 2008 2009 2010 2011 2012 Time Note. BC = British Columbia. The vertical line indicates the first full month of implementation of immediate roadside prohibition programs in October 2010 (intervention effect = –5.7 admissions for road trauma per 1 000 000 BC residents). The dotted curve represents the smoothed annual average of monthly rates from observed rates in part a and from the fitted model in part b. FIGURE 3—Monthly hospital admissions per 1 000 000 population for (a) all trauma causes except road trauma and (b) road trauma: British Columbia, January 2004–March 2012. found a 33.3% reduction in fatal speeding crashes in British Columbia. In a subgroup analysis that excluded crashes related to both alcohol and speeding, the reduction in fatal speeding-related crashes was smaller (21%) and was not statistically significant at the nominal level. However, this analysis was based on half as many events, resulting in an imprecise estimate of the effect (i.e., wide confidence intervals), and important reductions in this subgroup cannot be ruled out. Other researchers found that both higher fines and visible enforcement reduce the incidence of speeding39,40 but that increased enforcement is more effective.41 British Columbia’s new laws did not include increased speed enforcement and did not increase sanctions for the majority of speeding drivers. This limited scope may explain why British Columbia’s laws had a smaller effect on speeding fatalities. Neither Alberta nor Saskatchewan had reductions in speeding-related fatal crashes. It is interesting to note that Washington State had a statistically significant reduction in speeding-related fatal crashes. Beginning in July 2010, Washington began to roll out “target zero teams.”42 These teams use a systems approach including education and increased enforcement to target speeding, impaired driving, and failure to use seatbelts. The reduction in speeding-related crashes seen in Washington may be related to this approach. Strengths and Limitations We used multiple data sources to examine the effects of British Columbia’s new laws on health outcomes and on fatal crashes. Most October 2014, Vol 104, No. 10 | American Journal of Public Health evaluations of traffic laws rely exclusively on police data,43---46 which often have limited information on injury severity and may not capture all injury crashes.25,26 To account for trends and unmeasured confounders, we used ARIMA models21 and internal controls. We also compared British Columbia traffic fatalities with those in adjacent jurisdictions. Because medical data do not include factors that caused the crash, we cannot confirm that the observed reduction in ambulance calls and hospital admissions for road trauma was attributable to fewer crashes caused by the targeted risk factors (alcohol, speeding). Finally, deterrencebased laws often have reduced effectiveness over time. Longer follow-up will be required to determine whether the beneficial effects of British Columbia’s new laws are long lasting. Brubacher et al. | Peer Reviewed | Research and Practice | e95 RESEARCH AND PRACTICE a Rate/1 000 000 BC Residents Intervention 1800 1700 1600 1500 2004 2005 2006 2007 2008 2009 2010 2011 2012 Time b Rate/1 000 000 BC Residents Intervention 900 800 700 600 500 400 2004 2005 2006 2007 2008 2009 2010 2011 2012 Time Note. BC = British Columbia. The vertical line indicates the first full month of implementation of immediate roadside prohibition programs in October 2010 (intervention effect = –47 calls for road trauma/1 000 000 BC residents). The dotted curve represents the smoothed annual average of monthly rates from observed rates in part a and from the fitted model in part b. FIGURE 4—Monthly ambulance calls per 1 000 000 population for (a) all trauma causes except road trauma and (b) road trauma: British Columbia, January 2004–March 2012. Conclusions Traffic laws that introduced immediate license suspension and vehicle impoundment for drunk drivers and vehicle impoundment for excessive speeding, stunt driving, or street racing were associated with significant reductions in fatal crashes and in hospital admissions and ambulance dispatches for road trauma. These findings suggest that laws calling for immediate sanctions for dangerous drivers can reduce road trauma and should be supported. j About the Authors Jeffrey R. Brubacher, Herbert Chan, Edi Desapriya, and Roy Purssell are with the Department of Emergency Medicine, Faculty of Medicine, University of British Columbia, Vancouver. Roy Purssell is also with the British Columbia Centre for Disease Control, Vancouver. Penelope Brasher is with the Centre for Clinical Epidemiology and Evaluation, University of British Columbia. Shannon Erdelyi is with the Department of Statistics, University of British Columbia. Mark Asbridge is with the Department of Community Health and Epidemiology, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia. Scott Macdonald is with the Centre for Addictions Research of British Columbia, University of Victoria, British Columbia. Nadine Schuurman is with the Department of Geography, Faculty of Environmental Studies, Simon Fraser University, Burnaby, British Columbia. Ian Pike is with the British Columbia Injury Prevention and Research Unit, Faculty of Medicine, University of British Columbia. Correspondence should be sent to Jeffrey R. Brubacher, Vancouver Coastal Health Research Pavilion, Room 719, 828 West 10th Avenue, Vancouver, BC, Canada V5Z 1M9 (Jbrubacher@shaw.ca). Reprints can be ordered at http://www.ajph.org by clicking the “Reprints” link. This article was accepted April 24, 2014. access and assisted with methodology. P. Brasher oversaw statistical analysis and helped with interpretation of results. S. Erdelyi performed statistical analysis under supervision of P. Brasher and prepared figures and tables. E. Desapriya contributed relevant background information on the importance of media awareness campaigns and on driver surveys showing that drivers are aware of the new laws. M. Asbridge contributed to the section on policy diffusion and helped with interpretation of results. R. Purssell provided background information on details of British Columbia’s new laws. S. Macdonald provided background information on deterrence theory and its application to traffic laws. N. Schuurman assisted with data access and mapping. I. Pike assisted with access to hospital admission data and with interpretation of hospital admission data. All authors reviewed and contributed to the final article. Acknowledgments Contributors J. R Brubacher oversaw the project as a whole and was primary author of the article. H. Chan coordinated data e96 | Research and Practice | Peer Reviewed | Brubacher et al. This research was funded by a grant from the Canadian Institutes of Health Research and the Canadian Institute for Health Information. J. R. Brubacher is funded through American Journal of Public Health | October 2014, Vol 104, No. 10 RESEARCH AND PRACTICE a Scholar Award from the Michael Smith Foundation for Health Research. We thank the Insurance Corporation of British Columbia for providing access to the data from the British Columbia Traffic Accident System used in this article; Julie Wei, Randy Slemko, and the British Columbia Ambulance Service for providing access to the ambulance dispatch data used in this article; and Neil Arason (British Columbia Office of the Superintendent of Motor Vehicles) for providing a detailed explanation of British Columbia’s old and new traffic laws. general deterrence: theory and evidence. Criminology. 2001;39(4):865---892. at: http://www.edmontonsun.com/news/alberta/2010/ 11/16/16174126.html. Accessed November 23, 2013. 14. Beccaria C. On Crimes and Punishment. New York, NY: MacMillan; 1963. 33. Grattet R, Jenness V, Curry TR. The homogenization and differentiation of hate crime law in the United States, 1978 to 1995: innovation and diffusion in the criminalization of bigotry. Am Sociol Rev. 1998;63(2):286---307. Human Participant Participation 17. Ministry of Justice, Road Safety Unit, Police Services Division. Public attitude survey 2012: British Columbia. Available at: http://www.pssg.gov.bc.ca/policeservices/ publications-index. Accessed February 15, 2014. This study was approved by the University of British Columbia Clinical Research Ethics Board. References 1. World Health Organization. Global Status Report on Road Safety 2013: Supporting a Decade of Action. Geneva, Switzerland: World Health Organization; 2013. Available at: http://www.who.int/violence_injury_prevention/ road_safety_status/2013/en/index.html. Accessed February 15, 2014. 2. World Health Organization. Global Status Report on Road Safety: Time for Action. Geneva, Switzerland: World Health Organization; 2009. Available at: http://www. who.int/violence_injury_prevention/road_safety_status/ 2009. Accessed February 15, 2014. 3. Borkenstein RF, Crowther RF, Shumate RP, Ziel WB, Zylman R. The role of the drinking driver in traffic accidents (the Grand Rapids Study). Blutalkohol. 1974; 11(suppl):7---13. 4. Blomberg RD, Peck RC, Moskowitz H, Burns M, Fiorentino D. The Long Beach/Fort Lauderdale relative risk study. J Safety Res. 2009;40(4):285---292. 5. Blows S, Ameratunga S, Ivers RQ, et al. Risky driving habits and motor vehicle driver injury. Accid Anal Prev. 2005;37(4):619---624. 6. Grundy C, Steinbach R, Edwards P, Green J, Armstrong B, Wilkinson P. Effect of 20 mph traffic speed zones on road injuries in London, 1986-2006: controlled interrupted time series analysis. BMJ. 2009;339:b4469. 7. Asbridge M, Brubacher J, Chan H. Cell Phone Use and Traffic Crash Responsibility: A Culpability Analysis of Motor Vehicle Collisions in British Columbia. Paper presented at: Canadian Multidisciplinary Road Safety Conference XXI; May 8-- 11, 2011; Halifax, Nova Scotia, Canada. 15. Houston DJ, Richardson LE Jr. Drinking-and-driving in America: A test of behavioral assumptions underlying public policy. Polit Res Q. 2004;57(1):53---64. 16. Beirness DJ, Beasley EE. An evaluation of immediate roadside prohibitions for drinking drivers in British Columbia: findings from roadside surveys. Traffic Inj Prev. 2014;15(3):228---233. 18. The Road Safety Monitor 2012: Drinking and driving in Canada by region: trends. Available at: http://tirf.ca/publications/project_show.php?pid=16. Accessed February 15, 2014. 19. Macdonald S, Zhao J, Martin G, et al. The impact on alcohol-related collisions of the partial decriminalization of impaired driving in British Columbia, Canada. Accid Anal Prev. 2013;59:200---205. 20. International Classification of Diseases, 10th Revision. Geneva, Switzerland: World Health Organization; 1992. 21. Box GEP, Jenkins GM. Time-Series Analysis: Forecasting and Control. 2nd ed. San Francisco, CA: Holden-Day; 1976. 22. Mulgrew I. B.C.’s tough new impaired-driving rules declared unconstitutional in part, judge rules. Vancouver Sun. November 30, 2011. Available at: http://www. vancouversun.com/news/tough+impaired+driving+ rules+declared+unconstitutional+part+judge+rules/ 5790600/story.html. Accessed December 3, 2011. 23. Muggeo VMR, Adelfio G. Efficient change point detection for genomic sequences of continuous measurements. Bioinformatics. 2011;27(2):161---166. 24. Muggeo VM. Estimating regression models with unknown break-points. Stat Med. 2003;22(19):3055---3071. 25. Amoros E, Martin J-L, Lafont S, Laumon B. Actual incidences of road casualties, and their injury severity, modelled from police and hospital data, France. Eur J Public Health. 2008;18(4):360---365. 26. Amoros E, Martin J-L, Chiron M, Laumon B. Road crash casualties: characteristics of police injury severity misclassification. J Trauma. 2007;62(2):482---490. 8. Caird JK, Willness CR, Steel P, Scialfa C. A metaanalysis of the effects of cell phones on driver performance. Accid Anal Prev. 2008;40(4):1282---1293. 27. Asbridge M, Mann RE, Flam-Zalcman R, Stoduto G. The criminalization of impaired driving in Canada: assessing the deterrent impact of Canada’s first per se law. J Stud Alcohol. 2004;65(4):450---459. 9. Office of the Superintendent of Motor Vehicles. Road safety rules and consequences of unsafe driving. Available at: http://www.pssg.gov.bc.ca/osmv/roadsafety/index.htm. Accessed November 23, 2011. 28. Asbridge M, Mann RE, Smart RG, et al. The effects of Ontario’s administrative driver’s licence suspension law on total driver fatalities: a multiple time series analysis. Drugs Education Prev Policy. 2009;16(2):140---151. 10. British Columbia Motor Vehicle Act. Available at: http://www.bclaws.ca/EPLibraries/bclaws_new/document/ ID/freeside/96318_00. Accessed November 23, 2011. 29. Wagenaar AC, Maldonado-Molina MM. Effects of drivers’ license suspension policies on alcohol-related crash involvement: long-term follow-up in forty-six states. Alcohol Clin Exp Res. 2007;31(8):1399---1406. 11. Shepherd JP. Criminal deterrence as a public health strategy. Lancet. 2001;358(9294):1717---1722. 12. Wright V. Deterrence in criminal justice: evaluating certainty vs severity of punishment. Available at: http://www.sentencingproject.org/doc/Deterrence% 20Briefing%20.pdf. Accessed November 11, 2011. 13. Nagin DS, Pogarsky G. Integrating celerity, impulsivity, and extralegal sanction threats into a model of 34. Asbridge M. Public place restrictions on smoking in Canada: assessing the role of the state, media, science and public health advocacy. Soc Sci Med. 2004;58(1):13---24. 35. Shipan CR, Volden C. Policy diffusion: seven lessons for scholars and practitioners. Public Adm Rev. 2012;72 (6):788---796. 36. Platt M. B.C. drunk driving law sobers Alberta. Toronto Sun. September 22, 2010. Available at: http://www.torontosun.com/news/canada/2010/09/ 23/15447056.html. Accessed November 12, 2013. 37. Edmonton Police Services. Camrose adopts Curb the Danger. Available at: http://www.edmontonpolice.ca/ News/SuccessStories/CamroseAdoptsCurbTheDanger. aspx. Accessed November 15, 2013. 38. Drivers RI. Be the difference: community action for safe roads. Available at: http://bethedifferencealberta.com/ report-impaired-drivers. Accessed November 23, 2013. 39. Jones B, Haas K, Kirk A, Griffith A. Self-reported effectiveness of double-fine zones as a speed control measure. Appl Health Econ Health Policy. 2004;3(1):17---28. 40. Vaa T. Increased police enforcement: effects on speed. Accid Anal Prev. 1997;29(3):373---385. 41. Ryeng EO. The effect of sanctions and police enforcement on driver’s choice of speed. Accid Anal Prev. 2012;45:446---454. 42. Target Zero—Washington State strategic highway safety plan 2013. Available at: http://www.targetzero. com. Accessed February 11, 2014. 43. Wagenaar AC, Maldonado-Molina MM, Erickson DJ, Ma L, Tobler AL, Komro KA. General deterrence effects of US statutory DUI fine and jail penalties: long-term follow-up in 32 states. Accid Anal Prev. 2007;39:982---994. 44. Andreuccetti G, Carvalho HB, Cherpitel CJ, et al. Reducing the legal blood alcohol concentration limit for driving in developing countries: a time for change? Results and implications derived from a time-series analysis (2001---10) conducted in Brazil. Addiction. 2011;106(12):2124---2131. 45. Blais E, Gagne M-P. The effect on collisions with injuries of a reduction in traffic citations issued by police officers. Inj Prev. 2010;16(6):393---397. 46. Friedman LS, Barach P, Richter ED. Raised speed limits, case fatality and road deaths: a six year follow-up using ARIMA models. Inj Prev. 2007;13(3):156---161. 30. Traynor TL. The impact of state level behavioral regulations on traffic fatality rates. J Safety Res. 2009; 40(6):421---426. 31. Baicker K. The spillover effects of state spending. J Public Econ. 2005;89(2---3):529---544. 32. Landry F. Alta. may stiffen drinking and driving laws. Edmonton Sun. November 17, 2010. Available October 2014, Vol 104, No. 10 | American Journal of Public Health Brubacher et al. | Peer Reviewed | Research and Practice | e97