This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this
material constitutes acceptance of that license and the conditions of use of materials on this site.
Copyright 2007, The Johns Hopkins University and Ronald Gray. All rights reserved. Use of these materials
permitted only in accordance with license rights granted. Materials provided “AS IS”; no representations or
warranties provided. User assumes all responsibility for use, and all liability related thereto, and must independently
review all materials for accuracy and efficacy. May contain materials owned by others. User is responsible for
obtaining permissions for use from third parties as needed.
LECTURE 3.a.
Female and Male
Infertility
Lecture Objectives
Different definitions of infertility
Time trends and geographic variations in
infertility
Etiology and treatment of male and female
factor infertility
Adverse effects of infertility treatment
3
Definitions of infertility
Inability to achieve a recognized pregnancy after trying to
conceive for:
– > 1 year (U.S. ACOG) or
– > 2 years (WHO)
Primary infertility: no prior pregnancy
Secondary infertility: Prior pregnancy by woman or man
Infecundity: Inability to achieve a live birth
4
Prevalence of Infertility
Depends on the question
Definition
Prevalence (%)
Ever waited > 24 months
20.6
Tried for > 24 months
12.5
Consulted a physician
9.6
Diagnosed infertility
6.1
Prevalence of infertility depends on the
specificity of the question asked
5
Demographic Definitions
Primary infertility: Absence of a live birth at
specific ages (e.g. > age 30) in noncontracepting population
Secondary infertility: Absence of a live birth
> 5 years in persons with prior births
6
Prevalence of Infertility in U.S.
1965 - 1995
U.S. Married Women Aged 15 – 44 years
1965
1982
1988
1995
All
13.3
13.9
13.7
11.9
Primary
2.2
5.8
6.0
5.7
Secondary
11.1
8.1
7.7
6.2
Definition: Inability to conceive >1 year, within past 3
years. NSFG 1965 – 1995.
Source: Chandra. Infertil Repro Clin North Amer 1994;5:283.
7
Numbers of Infertile Women in US
1965
1982
1988
1995
3.0
2.4
2.3
2.1
Number
(millions)
Excludes sterilized couples.
Source: NSFG 1995.
8
U.S. trends in primary infertility
Demographic:
– Delay in marriage (1968 24.9 vs 2002
25.1 yrs)
– Delay in first birth 1968 21.4 vs 2002
25.1 yrs
– Delayed childbearing → shifts first births
to later ages when fertility is lower
Biologic:
– Possible effects of STDs and PID?
9
U.S. Trends in secondary infertility
Decrease in Secondary Infertility
– Decrease in family size since 1960’s
– More couples adopt sterilization to
terminate reproduction and do not
recognize secondary infertility
10
11
Developing Country trends
Most data come from demographic sources
– Proportions childless age 25-34
– Proportions with no birth in past 5 years
Range of primary infertility, 3-20+%
Regional variation: Historic “Infertility Belt”
in central Africa
– Cameroon, Congo, Uganda
12
Trends in Developing Countries
Infertility in Africa decreased in recent
decades
– Difficult to determine trends from
surveys due to selective inclusion of
currently married women (e.g. infertile
women may often be divorced)
– Variation in survey samples over time
13
Trends in Developing Countries
Papua New Guinea
– Tabar infertility 45% in 1940’s decreased to
18.5% in one generation following use of
penicillin for presumptive therapy
Zaire
– Equater province infertility 42% in1955,
decreased to 9.7% in 1975
Source: WHO Technical Report 1975; No. 582
14
Etiology of Infertility
Etiologic studies require invasive procedures and
clinical evaluation
Variability between clinics
– Type of service (general, specialization)
– Triage (selective referral)
– Costs and socioeconomic barriers
– Lack of standardization
Female cause ∼ 50-60%
Male cause ∼ 40-50%
15
Etiology of Infertility in Women
Tubal oculsion due to Pelvic Inflammatory
Diseases (PID)
– Industrialized countries 33%
– Africa 75%
Ovulatory disorders
– ∼ 30%
Endometriosis
HIV
Toxic exposures:
– smoking, glycol ethers, nitrous oxide,
pesticides
16
Pelvic Inflammatory Disease and Infertility
1. Cervical infection (C. trachomatis and/or N. gonorrhoeae)
17
Pelvic Inflammatory Disease and Infertility
2. Alteration of cervicovaginal microenvironment, increased pH
18
Pelvic Inflammatory Disease and Infertility
3. Overgrowth of vaginal and anaerobic flora, resulting in BV.
19
Pelvic Inflammatory Disease and Infertility
4. Progressive ascent of original cervical pathogen and/or BV
anaerobes into the endometrium, fallopian tubes, and the
peritoneal cavity.
20
Sequence of Extension
1.
2.
3.
4.
Cervix
Uterine Cavity
Fallopian Tubes
Abdominal Cavity
21
Clinical Features
Endocervicitis: May be asymptomatic; vaginal
discharge, cervical inflammation, or infection;
local tenderness
Endosalpingitis: Constant bilateral lower
quadrant abdominal pain aggravated by body
motion. Tenderness in one or both adnexal
areas. Abscess formation may occur.
Endometriosis: Menstrual irregularity
Peritonitis: Nausea, emesis, abdominal
distention, rigidity, tenderness. Pelvic or
abdominal cavity abscess formation may follow.
22
Tubal Factor Infertility & PID
Percent of women with tubal factor infertility following PID,
by number of episodes
50
45
40
Percent
35
30
25
20
15
10
5
0
0
1
2
3+
Number of PID Episodes
Source: Westrom LV. Sex Trans Dis 1994;24(2 Suppl):S32-37.
23
Pelvic Inflammatory Disease
Hospitalizations of Women 15 to 44 years United
States, 1980–2003
Hospitalizations (in thousands)
200
Acute, Unspec.
Chronic
160
120
80
40
0
1980
82
84
86
88
90
92
94
96
98
2000
02
Note: The relative standard error for these estimates of the total number of acute and
chronic PID cases ranges from 6% to 18%. Data available through 2003.
SOURCE: National Hospital Discharge Survey (National Center for Health Statistics, CDC)
24
Pelvic Inflammatory Disease
Initial Visits to Physicians’ Offices
Women 15-44 : US, 1980-2004
Visits (in thousands)
500
400
300
200
100
0
1980
82
84
86
88
90
92
94
96
98
2000
02
04
Note: The relative standard error for these estimates ranges from 19% to
30%.
SOURCE: National Disease and Therapeutic Index (IMS Health)
25
Ectopic Pregnancy
Hospitalizations of Women 15 to 44 United
States, 1980–2003
Hospitalizations (in thousands)
100
80
60
40
20
0
1980
82
84
86
88
90
92
94
96
98
2000
02
Note: Some variations in 1981 and 1988 estimates may be due to changes in sampling
procedures. The relative standard error for these estimates ranges from 8% to 12%. Data
available through 2003.
SOURCE: National Hospital Discharge Survey (National Center for Health Statistics, CDC)
26
Smoking and Subfertility
Risks of subfertility > 1 year
– Mother smoker
• RR = 1.5 (1.2-2.0)
– Father smoker, mother non-smoker
(passive smoking)
• RR = 1.2 (1.0-1.4)
Source: Hull et al. Fertil Steril 2000;74:725
27
Microchip Manufacturing: Female Workers
Exposure to Ethylene Glycol Ethers (EGE)
EGE
Exposure
Subfertility
(Inability to conceive > 1year)
(%)
RR (CI)
None
9.2
1.0
Low
13.3
1.5 (0.7-3.1)
Medium
13.3
1.8 (0.8-4.3)
High
27.3
4.6 (1.6-13.3)
Source: Correa A, et al. Ethylene glycol ethers and risks of spontaneous
abortion and subfertility. Am J Epidemiol 1996;143:707-17
28
Treatment of Female Infertility
Tubal Oculsion
– Assisted Reproductive Technologies
(ART)
• In vitro fertilization (IVF)
• Gamete intrafallopian transfer (GIFT)
• Zygote intrafallopian transfer (ZIFT)
– Tubal surgery
29
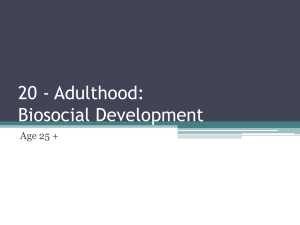
In vitro fertilization (IVF)
(1) Once mature, the eggs
are suctioned from the
ovaries and (2) placed in a
laboratory culture dish with
the man's sperm for
fertilization. (3) The dish is
then placed in an incubator.
(4) About 2 days later, 3 to
5 embryos are transferred
to the woman's uterus.
Public Domain
United States: 1 in 80-100 births now IVF conceptions;
100,000 IVF cycles; 48,000 births
30
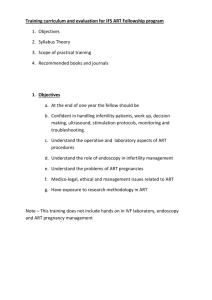
Live births per embryo transfer, by
age of mother and age of donor
Figure 2. Van Vorhiss BJ. Clinical practice. In vitro fertilization. NEJM 2007 Jan 25;356(4):379-86.
Copyright © 2007 Massachusetts Medical Society. All Rights Reserved.
31
Preconception genetic diagnoses
One or two balstomeres are removed from
the embryo
Chromosome identification and evaluation
by fluorescence in situ hybridization (FISH)
Current techniques allow evaluation of up
to 10 chromosomes in a single cell
32
Treatment of Female Infertility
Ovulation Disorders
– Ovulation induction by Clomid, GnRH
Endometriosis
– Drug treatment (Danazol)
– Surgery
33
Prognosis of Infertility
Prognosis varies with:
– Age
– Primary vs. secondary infertility
– Duration of infertility
– Type and severity of pathology
– Single vs. multiple causes
– Male, female, or both affected
– Smoking, caffeine, nutrition
34
Delivery Rates with IVF
No male factor
Age
Delivery %
<35
35.7
35-39
33.5
40+
10.3
Male factor infertility
Age
Delivery %
<35
35.1
35-39
33.5
40+
12.8
ASRM/SART Registry Fertil Steril 2002;77:18-31
35
Outcomes of IVF: U.S.
Live births per embryo transfer ~50%
Pregnancy loss ~ 18%
Multiple births per delivery
– 31% twins
– 3% triplets or more
– (normal conception, 1% multiple gestations)
Source: Society for Assisted Reprod Technol. Fertil Steril 2000;74:641.
Bradley NEJM 2007;356:379
36
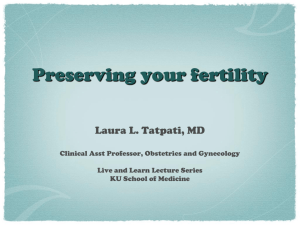
Percentage of twins after in vitro fertilisation by
year of birth in Europe
Kallen, B. et al. BMJ 2005;331:382-383. All Rights Reserved.
Copyright ©2005 BMJ Publishing Group Ltd.
37
IVF Pregnancy Outcomes
(Shevell Obstet Gybecol 2005;106:1039)
Odds of adverse outcomes IVF vs no ART
– Preeclampsia
OR 2.7 (1.7-4.4)
– Preterm labor
OR 1.5 (1.0-2.2)
– Placental abruption OR 2.4 (1.1-5.2)
– Placenta previa
OR 6.0 (3.4-10.7)
– Cesarean section OR 2.3 (1.8-2.9)
38
Low Birth Weight and ART (US)
Schieve NEJM 2002;346:731-7
– N = 42,463 ART vs 3,389,098 natural
conceptions
– Risk of low birth weight with ART RR = 2.6
(2.4-2.7)
– Very low birth weight (<1500 gm) RR = 1.8
(1.7-2.0)
– 4.3% of very low birth weight attributable to
ART
39
Birth Defects and ART
N = 837 IVF; 301 ICSI; 4000 natural conceptions
All Major Defects:
– IVF = 9.0%, ICSI = 8.6%, natural = 4.2%
– IVF RR = 2.0 (1.5-2.9); ICSI RR = 2.0 (1.33.2)
– Musculoskeletal defects: IVF = 3.3%, ICSI =
3.3%, natural = 1.1%
– Chromosomal defects: IVF = 0.7%, ICSI =
1.0%, Natural = 0.2%
VLBW: IVF = 4%, ICSI = 1%, natural= 1.0%
–
Hansen NEJM 2002;346:725-30
40
Costs of in vitro Fertilization
Ovulation induction
$1500-5000
Artificial insemination
$1000-2000
IVF woman’s own eggs
$12,500-25,000
IVF donor eggs
$20,000-35,000
41
Insurance Coverage and IVF: USA 2001
IVF primarily privately funded
– 3 states full coverage
– 5 states partial coverage
– 37 states no coverage
IVF per 1000 women
– Full coverage
– Partial coverage
– No coverage
Jain NEJM 2002;347:661
3.8/1000
1.8/1000
1.4/1000
IVF procedures 1996 = 64,036 vs 2001 = 107,587
42
Infertility and Pregnancy Loss
Women with recurrent EPLs have no
recognized pregnancy and report delayed
conception. If delay >1 year classified as
infertile.
Increased SABs in women with infertility may
reflect a common mechanism of damage to
ovum and fetus such as toxic exposures.
– e.g., Glycol ethers increase SAB (RR=
2.8) and infertility (RR = 4.6)
43
Infertility and Pregnancy Loss
Early Pregnancy Loss (EPL)
– No Infertility history
– Infertility history
EPL = 21.1%
EPL = 69.7%
Spontaneous Abortion (SAB)
– No Infertility history
– Infertility history
SAB = 14%
SAB = 23%
Women with delays in conception have higher rates
of EPLs and SABs
44
Microchip Manufacturing: Female Workers
Exposure to Ethylene Glycol Ethers (EGE)
EGE
Exposure
Spontaneous
Abortion
(%)
RR (CI)
Subfertility
(%)
RR (CI)
None
14.8
1.0
9.2
1.0
Low
16.0
13.3
Medium
18.9
High
33.3
1.0
(0.6-0.7)
1.4
(0.8-2.6)
2.8
(1.4-5.6)
1.5
(0.7-3.1)
1.8
(0.8-4.3)
4.6
(1.6-13.3)
13.3
27.3
45
Infertility, SABs, and Age
Infertility increases with age
SABs increase with age
Due to ovum deterioration with age
IVF with donation of an ovum from young
women to an older recipient increases
pregnancy rates and decreases SABs
46
Male Infertility
GNU Free Documentation License
47
Etiology of Male Infertility
Varicoele ∼ 20-40% (importance?)
Infections (e.g. mumps, STD orchitis &
epididymitis, HIV)
Undescended testis
Toxins (e.g. DPCP, glycol ethers)
48
Treatment of Male Infertility
Varicocelectomy
– 7 Randomized trials no benefit
– Pregnancy RR = 1.04 (0.7-1.4)
– Evers & Collins Lancet 2003;361:1849
Artificial insemination by donor or self
Hormone supplements
Intracytoplasmic sperm injection (ICSI)
49
Male fertility and time trends in semen
quality
Factors influencing male fertility
Male fertility and age, effect of endocrine
status
Secular trends in semen quality
Testicular development and testicular cancer
as a marker of adverse effects
Possible effects of environmental factors
including environmental estrogens, endocrine
disruptors hypothesis
51
Male Fertility and Age
Sexual activity declines with age
Testosterone decline with age
Semen quality and age
Difficult to estimate male fertility with age,
independent of female age-specific fertility
– Correlation of partner’s age
– Only women become pregnant
Ireland and Bangladesh data suggest decline in male
fertility > age 50
52
Number of sexual events per 5 years
Male Sexual Activity and Age
700
600
Any sexual activity
500
400
300
Sexual intercourse
200
100
0
20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79
Age groups
53
Testosterone Level and Age
Plasma Testosterone (mg/ml)
12
10
95th
8
75th
6
Median
25th
4
5th
2
0
20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59
Age (years)
Data Source: Simon D, et al. The influence of aging on plasma sex hormones in men: the
Telecom Study. Am J Epidemiol 1992;135;783-91.
54
Birth rates by male age married to women
aged 20-29, Ireland 1911
Birth per 1000 by male age
450
425
411
400
356
350
293
Birth/1000
300
250
200
150
100
50
0
1
~40
2
~45
3
male age
~50
4
60~
55
Assessment of Semen
Requires sample from masturbation
Assessed by:
– Semen volume (normal 5 mL)
– Sperm count (normal > 20 million/mL)
– Motility (>40%)
– Morphology (50% typical forms)
56
Problems in assessment of Semen
Variation in semen quality
– Between laboratories and regionally
– Season (lower in hot months)
– Age (lower with age)
– Recent ejaculation (decreased if < 3
days)
57
Semen Quality and Age
Young (<39)
Volume
Count
Motility
Abnormal
morphology
Older men (> 59)
5.3 mL
325 mill
32.8%
11.0%
Chromosomal abnormalities
11.9%
Volume
Count
Motility
Abnormal
Morphology
2.3 mL
208 mill
23.8%
12.8%
Chromosmal abnormalities
4.8%
Sartorelli, Fertil Steril 2001;76:1119-23
58
Seasonal Variation in Sperm Count
Sperm concentration, millions/ml
170
160
150
140
130
120
MacLeod
80
60
50
80
120
Levine (New Orleans)
Levine (Calgary)
70
110
100
60
90
50
70
110
Tjoa
70
Mortimer
60
Spira
100
50
90
40
80
30
70
90
80
70
60
60
SL Pol
Politoff
50
40
J
F
M
A
M
J
J
Calendar Month
A
S
O
N
D
J
F
M
A
M
J
J
A
S
O
N
D
Calendar Months
Data Source: Levine et al. Male factors contributing to the seasonality of human reproduction.
Ann NY Acad Sci 1994;709:29-45.
59
Time Trends in Semen Quality
Meta-analysis and some longitudinal studies
suggest declines in sperm counts of “normal”
males over time
– Is this evidence for male reproductive
damage?
Are these trends real?
– Consistency between studies
– Selection effects
– Definition of “normal”
– Adjustment for recency of intercourse, age
and season
60
Trends in Sperm Count over Time
From Carlsen E, et al. Evidence for decreasing quality of semen during
past 50 years. BMJ 1992;305:609-613. Copyright © 1992 BMJ. All Rights
Reserved.
61
Hormonal Disruptors hypothesis
“Environmental Estrogen Hypothesis”
Environmental estrogens may act as
hormonal disruptors:
– Diet (fat, phytoestrogens)
– Synthetic hormones
– Estrogenic chemicals (e.g. pesticides,
organochlorine and benzene derivatives)
– Solvents
– Fungicide causing azoospermia (DBCP)
62
Concentration of Sperm by Birth Cohort
350
8
Sem en Volum e (m L)
7
250
6
Sperm Concentration (x 10 / mL)
300
200
150
100
50
0
*
*
*
*
*
*
*
*
*
*
6
5
4
3
2
1
*
*
0
1950- 1955- 1960- 1965
54
59
64
1950- 1955- 1960- 1965
54
59
64
Birth Cohort
B i r t h C ohor t
Data Source: Rasmussen et al. No evidence for decreasing semen quality in four birth cohorts
of 1,055 Danish men born between 1950 and 1970 Fertil Steril 1997:68(6):1061.
63
Problems with Time Trends in Semen
Quality
Studies inconsistent
Variations in definitions of “normal” (WHO
definition decreased from 60 to 20
million/mL over time)
Selection of “normal” men varies between
studies (e.g. sperm donors, vasectomy
cases)
64
Problems with Time Trends in Semen
Lack of control for time since last
ejaculation, season, and age
Variation in laboratory methods, and interobserver variation in sperm counts
Confounding between regions
65