This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this
material constitutes acceptance of that license and the conditions of use of materials on this site.
Copyright 2007, The Johns Hopkins University and Bruce Trock. All rights reserved. Use of these materials
permitted only in accordance with license rights granted. Materials provided “AS IS”; no representations or
warranties provided. User assumes all responsibility for use, and all liability related thereto, and must independently
review all materials for accuracy and efficacy. May contain materials owned by others. User is responsible for
obtaining permissions for use from third parties as needed.
What is the current evidence for
progress against cancer?
Bruce Trock, PhD
"As far as the laws of mathematics
refer to reality, they are not certain; as
far as they are certain, they do not
refer to reality.“
--Albert Einstein
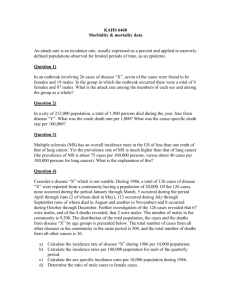
Change in the US Death Rates* by
Cause, 1950 & 2003
Rate Per 100,000
600
586.8
1950
500
2003
400
300
231.6
193.9
180.7
200
100
53.3
190.1
48.1
21.9
0
Heart
Diseases
Cerebrovascular
Diseases
Pneumonia/
Influenza
Cancer
* Age-adjusted to 2000 US standard population.
Sources: 1950 Mortality Data - CDC/NCHS, NVSS, Mortality Revised.
2003 Mortality Data: US Mortality Public Use Data Tape, 2003, NCHS, Centers for Disease Control and
Prevention, 2006
Lifetime Probability of Developing
Cancer, by Site, 1998-2000
Site
Male Risk
Female Risk
All sites
1 in 2
1 in 3
Prostate
1 in 6
n.a.
Breast
1 in 833
1 in 7
Lung & bronchus
1 in 13
1 in 17
Colon & rectum
1 in 17
1 in 18
565,000 deaths from cancer annually
Source: DevCan: Probability of Developing or Dying of Cancer Software, Version 5.1 Statistical Research and
Applications Branch, NCI, 2003. http://srab.cancer.gov/devcan
Progress Against Cancer
• NCI Goal in 1985: 50% decrease in cancer
mortality by year 2000*:
– 1985: 171 per 100,000
– 2000: 158 per 100,000 (7.6% decrease)
– 2004: 147 per 100,000 (14.0% decrease)
• How do you define progress against cancer?
• What has influenced progress?
• What will influence future progress?
* age-adjusted to 1970 population
Is overall mortality the best way
to define progress?
• Advantage:
– clinically most relevant; indicates biologic behavior
– less subject to artifact
• Disadvantage:
– obscures effects by age or tumor type
– have to balance against true increases in incidence
• Is the most important issue whether decreases in
mortality are due to improved treatment? Should the
measure of progress reflect government spending?
Measures of Progress
• Incidence – affected by:
– changes in risk factors
– increase in detection, treatment of premalignant lesions
– changes in definition of cancer
• Survival – affected by:
– changes in early detection
– changes in treatment
• Mortality – affected by:
– changes in incidence
– changes in survival
DEATHS PER 100,000
Mortality from All Malignant Neoplasms
1950 - 1982, by Race and Sex*
300
250
Nonwhite male
White male
Whole Population
White Female
Nonwhite Female
200
150
100
50
0
1950 1955
1960 1965 1970 1975 1980
YEAR
* Bailar, NEJM 1986; 314:1226
Cancer Incidence Rates*, All Sites, All
Races, 1975-2002
Incidence Rate Per 100,000
700
600
Men
500
Both Sexes
400
Women
300
200
100
0
1975
1978
1981
1984
1987
1990
1993
1996
*Age-adjusted to the 2000 US standard population and adjusted for delay in reporting.
Data from American Cancer Society website, www.cancer.org: Cancer_Statistics_2006_Presentation.ppt
1999
2002
Bailar’s Arguments (1950-1982)
Failures:
• increase in overall mortality, and in most race-sex groups.
• no decrease in breast, prostate or lung cancer mortality
• some decreases not due to treatment or to programmatic
efforts at prevention (stomach, colorectum, cervix)
• should some cancers be excluded from the evaluation?
Even excluding lung, stomach, cervix, < 1% decrease in
overall cancer mortality (in 1986), i.e. not “progress”
Cancer Death Rates* in US Men 1930-2002
(1950-1982 period covered by Bailar)
100
80
60
Stomach
Prostate
Colon & rectum
40
20
Pancreas
*Age-adjusted to the 2000 US standard population and adjusted for delay in reporting.
Data from American Cancer Society website, www.cancer.org: Cancer_Statistics_2006_Presentation.ppt
2000
1995
1990
1985
1980
1970
1965
1960
1955
1950
1945
1935
1930
1975
Liver
Leukemia
0
1940
Death Rate Per 100,000
Lung
Cancer Incidence Rates* US Men, 1975-2002
Incidence Rate Per 100,000
250
Prostate
200
150
Lung
100
Colon and rectum
50
Urinary bladder
Non-Hodgkin lymphoma
Melanoma of the skin
0
1975
1978
1981
1984
1987
1990
1993
1996
1999
*Age-adjusted to the 2000 US standard population and adjusted for delay in reporting.
Data from American Cancer Society website, www.cancer.org: Cancer_Statistics_2006_Presentation.ppt
2002
Cancer Death Rates* in US Women 1930-2002
(1950-1982 period covered by Bailar)
100
Death Rate Per 100,000
80
60
Lung
40
Uterus
Breast
Stomach
20
Colon & rectum
Ovary
Pancreas
*Age-adjusted to the 2000 US standard population and adjusted for delay in reporting.
Data from American Cancer Society website, www.cancer.org: Cancer_Statistics_2006_Presentation.ppt
2000
1995
1990
1985
1980
1975
1970
1965
1960
1955
1950
1945
1940
1935
1930
0
Cancer Incidence Rates* US Women, 1975-2002
Incidence Rate Per 100,000
250
200
150
Breast
100
Colon and rectum
Lung
50
Uterine Corpus
Ovary
0
1975
Non-Hodgkin lymphoma
1978
1981
1984
1987
1990
1993
1996
1999
*Age-adjusted to the 2000 US standard population and adjusted for delay in reporting.
Data from American Cancer Society website, www.cancer.org: Cancer_Statistics_2006_Presentation.ppt
2002
100
4500
90
4000
80
3500
70
Per capita cigarette
consumption
3000
60
2500
50
Male lung cancer
death rate
2000
40
1500
30
1000
20
Female lung cancer
death rate
500
2000
1995
1985
1990
1980
1975
1970
1960
1965
1955
1950
1945
1935
1940
1930
1925
1920
1910
1915
1905
0
1900
0
10
Year
*Age-adjusted to 2000 US standard population. Source: Death rates: US Mortality Public Use Tapes, 1960-2000,
US Mortality Volumes, 1930-1959, National Center for Health Statistics, Centers for Disease Control and
Prevention, 2002. Cigarette consumption: US Department of Agriculture, 1900-2000.
Age-Adjusted
Lung Cancer
Death
Lung Cancer
Death Rates
Rates* per 100,000)
(age-adjusted,
5000
Per Capita Cigarette Consumption
Per Capita Cigarette Consumption
US Tobacco Use vs. Lung Cancer Deaths,
1900-2000
Mortality from All Malignant Neoplasms
1970 - 1994, by Race and Sex*
Deaths per 100,000
Death Rate (per 100,000)
450
400
350
Black Males
White Males
Total
Black Females
White Females
300
250
200
150
100
50
0
1970 1975 1980 1985 1990 1994 2000
* vertical lines: last years of data
in 1986 and 1997 Bailar papers
SEER*Stat Database: Mortality - Public-Use, Total U.S. (1969-2001)
NCI, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2004
Mortality from All Malignant Neoplasms
1970 - 2004, by Race and Sex*
Deaths per 100,000
Death Rate (per 100,000)
450
400
350
Black Males
White Males
Total
Black Females
White Females
300
250
200
150
100
50
0
1970 1975 1980 1985 1990 1994 2000 2004
* dotted lines: last years of data
in 1986 and 1997 Bailar papers
SEER*Stat Database: Mortality - Public-Use, Total U.S. (1969-2001)
NCI, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2004
Percentage of 1970 Death Rate
Mortality from All Cancers except Lung,
Oral/Larynx, Stomach, Cervix,1970-2000*
120
110
100
Males
Females
Both Sexes
90
80
70
60
1970
1975
1980
1985
1990
1995
2000
* SEER*Stat Database: Mortality - Public-Use, Total U.S. (1969-2001)
NCI, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2004
Annual percentage change in overall cancer
mortality rates (1975-2004) *
1975-1990 1990-1993 1993-2002 2002-2004
- 0.3% **
Both Sexes
0.5 %
Males
0.9 %
0.3%
Females
0.6 %
- 0.2%
- 1.1%
- 2.1%
- 1.5%
- 2.6%
-
- 1.8%
0.8%
* Espey DK, et al. Cancer 2007.
** Red font indicates change is not statistically significant
Mortality from All Cancers 1970-2000,
by Age & Sex*
Percentage of 1970 Death Rate
(extends Figure 2 from Bailar, NEJM 1997)
120
110
100
Male <55
Female <55
Male 55+
Female 55+
90
80
70
60
1970
1975
1980
1985
1990
1995
2000
* SEER*Stat Database: Mortality - Public-Use, Total U.S. (1969-2001)
NCI, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2004
Mortality from Lung Cancer 1970-2000,
by Age & Sex*
Percentage of 1970 Death Rate
(extends Figure 4 from Bailar, NEJM 1997)
450
400
350
Male <55
Female <55
Male 55+
Female 55+
300
250
200
150
100
50
1970
1975
1980
1985
1990
1995
2000
* SEER*Stat Database: Mortality - Public-Use, Total U.S. (1969-2001)
NCI, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2004
Breast cancer mortality trends in countries
that have introduced screening*
Mortality from Breast Cancer
1970-2000, by Age & Sex*
Percentage of 1970 Death Rate
(extends Figure 3 from Bailar, NEJM 1997)
120
110
100
Female < 55
All Women
Female 55+
90
80
70
60
1970
1975
1980
1985
1990
1995
2000
* SEER*Stat Database: Mortality - Public-Use, Total U.S. (1969-2001)
NCI, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2004
Cancer Incidence Rates* US Women, 1975-2004
200
150
Breast
100
Colon & rectum
50
Lung & bronchus
Uterine corpus
*American Cancer Society website:
Age-adjusted to 2000 US standard population (Source: SEER 2004).
2001
1999
1997
1995
1993
1991
1987
1985
1983
1981
1979
1977
1989
Ovary
0
1975
Incidence Rate Per 100,000
250
Breast cancer incidence rates 1999-2004*
150
140
8%
decrease
130
120
110
100
1999
* SEER data
2000
2001
2002
2003
2004
Breast cancer incidence 1975-2004, by
age group
Breast cancer incidence vs. HRT prescriptions 2000-2004*
Bailar’s claims of failure (1986-1994)
vs. updated mortality data
• Large increases in breast and prostate 1974-1990 are
overdiagnois so don’t balance mortality [mortality now
decreasing faster than incidence: treatment, early detection]
• 1986-1991: increase in mortality stopped in 1991, 1%
decrease 1991-1994; likely to continue due to smoking change
[Yes: 9% decrease from 1994-2002. But decreases since
1990 in leukemia, myeloma, brain, bladder and NHL (since
1996) – likely due to treatment]
• 1970-1994 decreases in stomach, cervical and colorectal
mortality due to decreased risk factors, early detection, but
not to treatment or prevention programs [mortality continues
to decrease without major treatment advances]
What Bailar Ignores
• Mortality decreased dramatically in ages < 55 (197390) or < 65 (1991-2004), not all due to early detection
or cohort effects (breast).
• Different trends by age group represents a statistical
interaction – in such a setting, overall age-adjusted
rates are misleading
• Treatment advances (chemotherapy) slower to occur in
elderly (other illnesses, less aggressive treatment,
cohort effects).
• Since 1991, decreases in all of 10 biggest cancer killers
Where are we Now?
• Mortality was increasing through early 1990’s, is now
decreasing or flat in all major cancers except liver (males),
lung (females - may be starting to decrease)
• Annual percentage changes in mortality:
2000-2004 (2.1% decrease) vs. 1970-1990 (0.5% increase)
• Decreases in mortality have been influenced more by risk
factor reduction and early detection than treatment
• Some mortality increases have clearly identifiable risk
factors (melanoma, non-Hodgkin’s lymphoma, liver)
• Some increases are unexplained (testis, esophageal
adenocarcinoma, multiple myeloma)
Trends in Overweight (BMI>25) Prevalence (%), Adults
18 and Older, US, 1992-2002
1992
1995
2002
1998
Less than 50%
50 to 55%
More than 55%
State did not participate in survey
Source: Behavioral Risk Factor Surveillance System, National Center for Chronic Disease Prevention and Health
Promotion, Centers for Disease Control and Prevention, 1997, 2000, 2003.
Cancer in the absence of screening
Death
Birth
cancer
appears
clinically
Survival Time
Appropriate diagnosis due to screening
Death
Birth
cancer
appears
clinically
Survival Time
Death
Birth
cancer
detected
by screen
cancer
appears
clinically
Pre-clinical Phase
Screening effective, life extended
Death
Birth
cancer
appears
clinically
Survival Time
Death
Birth
cancer
detected
by screen
cancer
appears
clinically
Increased Survival Time
Death
Lead-time bias, life not extended:
treatment doesn’t cure screened cancers
Death
Birth
cancer
appears
clinically
Survival Time
Death
Birth
cancer
detected
by screen
cancer
appears
clinically
Survival Time
Overdiagnosis, life not extended:
screening identifies tumors of low lethality
Death
Birth
cancer
detected
by screen
Survival Time
cancer
would have
appeared
clinically