INTRODUCTION RESULTS
advertisement

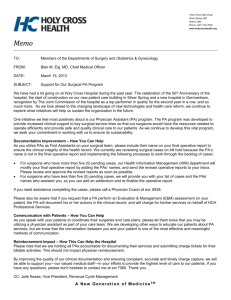
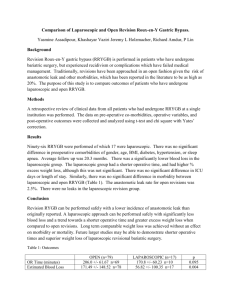
Single Institution Robotic vs Laparoscopic Nissen Fundoplication Surgical Time and Total Operating Time Comparison as a Measure of Cost Analysis 1 BS , 1 MD , 1 MD , Colin McGuire, Jorge Uribe, Lawrence Greenawald, Francisco Couto, 1 1, 2,3 1 D. Scott Lind, MD , Patricia A. Shewokis, PhD , Andres Castellanos, MD 1 MD , 1. Department of Surgery, Drexel University College of Medicine. Philadelphia, PA 2. Nutrition Sciences Department, College of Nursing and Health Professions, Drexel University, Philadelphia, PA 3. School of Biomedical Engineering, Science and Health Systems, Drexel University, Philadelphia, PA RESULTS INTRODUCTION The current surgical therapy for correcting gastroesophageal reflux disease is laparoscopic Nissen fundoplication (LNF). This surgical method has been standard in the United States since 1992 (Rothenberg, 2013). The utilization of robotic Nissen fundoplication (RNF) has been increasing. However, its role in the management of gastroesophageal reflux disease remains unclear. The reason for this distinction is due to RNF having similar outcomes as LNF but with a higher cost. RESULTS RNF has a lower surgical time compared to LNF (83 vs 155; p < 0.005), a lower total operative time (122 vs 219; p < 0.001), lower surgical cost (1441 vs 2779; p < 0.005), and lower total operative cost (1723 vs 3671; p < 0.001). The lower operative times are associated with a surgeon who has passed the learning curve. 350 240 300 180 250 200 120 150 CONCLUSION 100 60 We hypothesize that refinement of surgical technique with resultant lower total operative time for RNF will reduce cost low enough that RNF will be priced similar to LNF. DESIGN 50 0 0 Robotic (n = 46) Laparoscopic (n = 9) Laparoscopic (n = 9) Figure 1A,B: Comparison of A. median surgical time (min) and B. median total operative time (min) between robotic and laparoscopic Nissen fundoplication. p < 0.005 for surgical time; p < 0.001 for total operative time 4500 A single institution retrospective review of patients undergoing anti-reflux surgery from May 2013 to September 2014 was conducted. Patients were divided into two groups based on whether they received an RNF (n=46) or LNF (n=9). RNF cases were conducted by one surgeon while LNF cases were performed by two different surgeons. The total surgical operating time (from incision to closure) and total operating time (from the moment the patient enters the operating room to when the patient leaves the operating room) were calculated in minutes. Time and costs were compared between RNF and LNF using a Mann-Whitney U test for non-parametric distributions. Robotic (n = 46) Ongoing efforts include replicating the study at other institutions to gain more laparoscopic and robotic cases. Furthermore, elucidating the learning curve for RNF and LNF may lend further insight into the time/cost tradeoff. Finally, cost must be standardized across institutions for accurate comparisons. 6000 4000 5000 3500 3000 We demonstrate that a surgeon’s experience with RNF can have a large impact on the time and the cost associated with the surgery. The greater the surgeon’s experience the shorter the operative time and the lower the operative cost. 4000 2500 3000 2000 1500 2000 REFERENCES 1000 1000 500 0 0 Robotic (n = 46) Laparoscopic (n = 9) Robotic (n = 46) Laparoscopic (n = 9) Figure 2A,B: Comparison of A. median surgical cost (USD) and B. median total operative cost (USD) between robotic and laparoscopic Nissen fundoplication. p < 0.005 for surgical time; p < 0.001 for total operative time 1. Rothenberg S.S. (2013). Two decades of experience with laparoscopic Nissen fundoplication in infants and children: A critical evaluation of indications, technique and results. J Laparoendosc Adv Surg Tech A. 23(9):791-4. Doi: 10.1089/lap.2013.0299