Service Record – School Based Nursing Services
advertisement

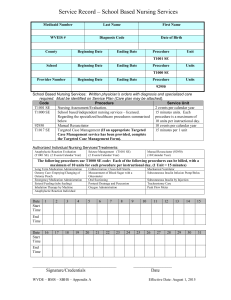
Service Record – School Based Nursing Services Medicaid Number Last Name First Name 00000000001 Doe Jane WVEIS # Diagnosis Code Date of Birth 590000001 F44.5 Conversion disorder with seizures or convulsion Beginning Date Ending Date County 01-01-1900 Procedure Unit 059 9-01-2015 9-01-2015 T1001 SE 1 School Beginning Date Ending Date Procedure Units 201 9-01-2015 9-31-2015 T1000 SE 21 Provider Number Beginning Date Ending Date Procedure Units Melanie Smith 9-22-2015 9-22-2015 92950 1 School Based Nursing Services: Written physician’s orders with diagnosis and specialized care required. Must be identified on Service Plan (Care plan may be attached). Code Procedure Service Unit T1001 SE T1000 SE Nursing Assessment/Evaluation. School based/independent nursing services – licensed. Regarding the specialized healthcare procedures summarized below 92950 T1017 SE Manual Resuscitator Targeted Case Management (If an appropriate Targeted Case Management service has been provided, complete the Targeted Case Management Form). 2 events per calendar year 15 minutes units. Each procedure is a maximum of 10 units per instructional day. 10 events per calendar year 15 minutes per 1 unit Authorized Individual Nursing Services/Treatments: Anaphylactic Reaction Evaluation (T1001 SE) (2 Events/Calendar Year) Seizure Management (T1001 SE) (2 Events/Calendar Year) Manual Resuscitator (92950) (10/Calendar Year) The following procedures use T1000 SE code: Each of the following procedures can be billed, with a maximum of 10 units for each procedure per instructional day, (1 Unit = 15 minutes) Long Term Medication Administration Ostomy Care: Emptying/Changing of Ostomy Pouch Emergency Medication Administration Enteral Feeding (tube feeding) Inhalation Therapy by Machine Anaphylactic Reaction Individual Catheterization: Clean-Self-Sterile Measurement of Blood Sugar with a Glucometer Oral Suctioning Postural Drainage and Percussion Oxygen Administration Date Start Time 1 11:00 2 11:00 3 11:00 4 11:00 End Time 11:15 11:15 11:15 11:15 Date Start Time 16 11:00 17 11:00 18 11:00 19 11:00 End Time 11:15 11:15 11:15 11:15 5 20 6 21 7 Subcutaneous Insulin by Injection Tracheostomy Care Peak Flow Meter 8 11:00 9 11:00 10 11:00 11 11:00 12 11:00 11:15 11:15 11:15 11:15 11:15 22 11:00 23 11:00 24 11:00 25 11:00 26 11:00 11:15 11:15 11:15 11:15 11:15 _____________________________________ Signature/Credentials WVDE – BMS – SBHS – Appendix A Mechanical Ventilator Subcutaneous Insulin Infusion Pump/Bolus 27 13 14 15 11:00 11:15 28 29 11:00 30 11:00 11:15 11:15 9-30-2015 Date Effective Date: August 1, 2015 31