Detection of Perfusion Defects in Murine Hearts with MRi at Low Magnetic Fields
by
Rushani T. Wirasinghe
Submitted to the Department of Electrical Engineering and Computer Science
in Partial Fulfillment of the Requirements for the Degree of
Master of Engineering in Electrical Engineering and Computer Science
at the Massachusetts Institute of Technology
etv
May 23, 2001 r
Copyright 2001 Rushani T. Wirasinghe. All rights reserved.
The author hereby grants to M.I.T. permission to reproduce and
distribute publicly paper and electronic copies of this thesis
and to grant others the right to do so.
Author
Department of EV ctrical Engi e
g and
mputer Science
May 23, 2001
Certified by
Deborah Burstein
Thesis Supervisor
Accepted by
Arthur e<Smith
Chairman, Department Committee on Graduate Theses
BARKER
MASSACHUSETTS INSTITUTE
OF TECHNOLOGY
JUL 112001
LIBRARIES
Detection of Perfusion Defects in Murine Hearts with MRI at Low Magnetic Fields
by
Rushani T. Wirasinghe
Submitted to the Department of Electrical Engineering and Computer Science
in Partial Fulfillment of the Requirements for the Degree of
Master of Engineering in Electrical Engineering and Computer Science
at the Massachusetts Institute of Technology
May 23, 2001
ABSTRACT
The goal of this study was to define a method to detect perfusion defects in murine myocardium with MRI
at low magnetic fields (2.0T). The detection method employed was blood volume imaging using the
intravascular contrast agent, gadolinium-DTPA bound to bovine serum albumin (Gd-BSA). This method
was used as opposed to others because of its good signal-to-noise ratio and its steady state nature, whereas
first-pass perfusion techniques are difficult to implement inside a magnet due to the difficulty of
maintaining a venous line in a mouse. An additional focus of the study was to evaluate the effectiveness of
various pulse sequences to define a fast sequence for detecting perfusion defects. Though preliminary
comparisons between RARE IR and turboFLASH IR, showed RARE IR with rare factor 2 to be preferable,
actual imaging on ischemic hearts with BSA seemed to favor an inversion recovery sequence with gradient
echo readout. Infarcts were induced in six mice by ligating the left coronary artery and the mice were
imaged after being administered with a dose of 0.1 mM/kg of Gd-BSA. The MR parameters used at a 2.0T
field for the mice were: axial slices with 1-1.25mm slice thickness, 200 pLm 2 in-plane resolution, trigger
delay of I ms. The sequence used was an inversion recovery sequence with gradient readout; inversion time
was set to null healthy myocardium (TI= 80-200ms), TE = 3-4ms and the repetition time (TR) was set to
1500ms. Results suggest a promising correspondence between MR images and TTC stains of the six mice.
Thesis Supervisor:
Deborah Burstein
Associate Professor of Radiology
Beth Israel Hospital
Harvard Medical School
2
Table of Contents
1.0 Acknowledgements ......
.............................
2.0 Motivation and Statement of Problem .........................
4
5
MRI theory:
3.0 Basic MRI Theory ......................................
4.0 Theory on Cardiac Pulse Sequences ....................................
7
19
Background Studies
5.0 Methods for Perfusion-defect Detection ................................. 28
6.0 Previous Studies done in Murine Heart Models ......................... 47
7.0 Tissue M odels............................................................
52
Experimental Procedures
8.0 Anatomy of the Mouse Heart ....................
....... 59
9.0 Electro physiology ...................................................
61
10.0 Experimental Setup & Procedures ........................
............
68
Results/ Discussion
11.0 Best dose of Gd-BSA to use .........................................
.
12.0 Optimal parameters for IR turboFLASH (GEFI IR) ...........
13.0 Optimal parameters for RARE IR .......................................
14.0 Comparison between histology and final infarct images .............
78
85
91
15.0 Overall Discussion of Study / Future Studies.........................
102
72
Reference
16.0 Bibliography ...................................
..
-3
106
1.0 Acknowledgements
I want to thank all those who contributed in teaching me about magnetic resonance imaging and
encouraging me during the process of my study. I came to the lab without any prior experience or
knowledge of MRI, only the desire to learn and to be able to contribute to the field of cardiac
study. I left with a wealth of information on MRI, a new perspective on science, and a reinforced
commitment to the study of medical science.
In particular I owe a great debt of gratitude to my supervisor Deborah Burstein. She had the
insight to keep a hawk's eye on me during my initial weeks with the lab and then to offer me the
space to grow and explore on my own once I was comfortable. She was also pivotal in teaching
me not just MRI, but healthy problem-solving techniques in science, a skill which I know shall
prove invaluable no matter which field I pursue.
My parents and brother were a spring of abundant support. Through the many hours of late night
experiments and writing, they were always on the phone to offer me a word of encouragement.
Both my friends and lab mates deserve my hearty thanks too for their kindness during the
moments of frustration every research student must encounter. In particular Jeeva Munasinghe,
the lab manager, was invaluable in my education of MRI. Despite his workload he always took
the time to explain obscure concepts to me and give me a hand when the hardware systems would
fail.
To all these people I offer my heart-felt thanks.
4
2.0 Introduction
Motivation:
The need to detect underperfused myocardial tissue is motivated by two reasons mainly:
1)
Reparative efforts: Many therapeutic decisions (such as revascularization) depend on the
extent of damage in the myocardium. Furthermore infarct detection can help scientists
gauge the effectiveness of various pharmacological interventions in preventing and
reversing myocardial necrosis.
2)
Understanding mechanisms underlying the heart's natural recovery: With advances in our
ability to modify the genetics of mammals, cardiologists are now better able to
understand the effect of different genes on cardiovascular function and disease. Typically
the gene being studied is either ablated ("knocked out") or modified and the development
of the resulting phenotype studied over the course of its lifetime. This technique enables
scientists not only to model and understand a particular heart disease but to also
scrutinize the biochemical mechanisms underlying the heart's recovery from this disease
or a heart attack for that matter. [Ruff, 1998 #20]
While analytical tools for in-vivo cardiac measurements have evolved extensively for large
mammals such as humans and pigs, the techniques remain less developed for smaller animals
such as rats and mice; this is not due because smaller animals are unpopular. In fact murine
models are heavily used in modeling cardiac conditions because of their technical and economic
advantages in genetics studies. The limiting factor in developing tools for smaller animals lies in
the technical difficulties posed by their size (heart size 5-8mm) and rapid heart rates (ten times
that of humans, meaning 600-700 bpm).
5
Because MRI offers the flexibility in choosing the imaging plane, multi-slice acquisition, and
most importantly high spatial and temporal resolution, it stands out as a powerful imaging tool for
evaluation of the myocardium in mice. [James, 1998 #33]
Goal of Study
Among the physiologic parameters that scientists aim to quantify in order to determine the status
of the myocardium is perfusion. Perfusion is defined as milliliters of arterial blood entering I Og
of tissue per minute.
Infarcted and ischemic tissue both have low perfusion numbers relative to healthy myocardium.
The goal of this study is to be able to detect perfusion defects in murine myocardium with MRI.
The main focus is on evaluating the effectiveness of various pulse sequences and parameters in
imaging perfusion defects. In order to improve differentiation between perfusion defects and
healthy myocardium, the hearts were enhanced with the contrast agent, gadolinium-DTPA bound
to bovine serum albumin (Gd-BSA). We opted to use a blood volume technique as opposed to
other perfusion imaging methods such as first pass, ASL, magnetic transfer, BOLD or IVIM
because of the better signal to noise ratio at a 2.OT field as well as the steady-state nature of this
imaging technique. Gd-BSA was chosen specifically because of its intravascular nature and its
growing popularity as a blood contrast agent in recent times.
6
3.0 Basics of MRI Theory
Skeleton
3.0 Introduction
3.1 The Semi-classical Model
3.2 Understanding TI, T2, and T2* and How to Measure Each
3.3 2-D Image Acquisition
3.4 Averaging, Spatial Resolution, Matrix Size, and FOV
3.0 Introduction
This section introduces the basic concepts of Magnetic Resonance Imaging. Emphasis is placed
on the concepts most relevant to the topic of this thesis. For a more in-depth explanation of the
concepts, the reader is referred to the texts cited in the bibliography. The theory underlying MR
imaging can be explained in terms of a quantum model, however for the sake of simplicity, most
texts choose to explain MR behavior via a semi-classical model. In this section we shall rely
mainly on the semi-classical model, touching only briefly on some quantumn concepts.
3.1 The Semi-classical Model
Equilibrium State
Magnetic resonance imaging relies on the inherent magnetic properties at the nuclear level,
specifically only nuclei with an odd number of protons or neutrons. Among the atomic isotopes
that can be imaged with magnetic resonance techniques are Hydrogen-1, Carbon-13, Fluorine-19,
and Phosphorous-3 1. In imaging anatomical structures hydrogen-I is often the atomic nuclei of
choice because of its sensitivity and abundance in biological samples. Hydrogen nuclei have a
spin number equal to
/2. The
spin number is a simple way to describe the number of energy states
and geometry of a nucleus; in this case hydrogen nuclei have two energy states.
Under normal conditions, a population of spins are randomly oriented and split relatively evenly
between the two energy states. However when subjected to a magnetic field B0, the atoms act in
coherence. A spin % nucleus (1H nucleus) precesses around the B in two possible orientations
7
(see Fig 3. 1 a) where each orientation is associated with an energy state. The motion is similar to
that of a spinning top and has an angular momentum, A.
(b)
(a)
Figure 3.1 : Spinning top model (a) and M, (b)
Given that the nucleus has a charge, it also has magnetic moment p, which can be related to the
angular moment (A) by a constant known as the gyromagnetic ratio, y (Eq 3.1). The
gyromagnetic constant for Hydrogen-I is 4258 Hz/G. The torque equation basically states that the
angular momentum is the result of the torque exercised by BO on the magnetic moment (Eq 3.2):
(Eq 3.1)
=yA
dA = p x B
(Eq 3.2)
dt
The magnetic moment precesses about the axis of the B0 field at wo, called the Larmour
frequency, which can be derived from Eq 3.1 and Eq 3.2
w. = yB0
(Eq 3.3)
As mentioned earlier, in a population of atoms influenced by B0 , each hydrogen spin aligns itself
in one of two possible orientations depending on its energy level. The exact proportion of spins
8
oriented parallel and anti-parallel to B0 is a function of the thermal energy in the system and can
be described by the Boltzmann distribution. At equilibrium the distribution of spins is:
Nu = e -(yhBo/kT)
N,
(Eq 3.4)
where N, and N, correspond to respectively the spin population in the upper and lower energy
levels, k represents the Boltzman constant and T is the sample temperature in Kelvin. At room
temperatures in a magnetic field of 2.OT, the ratio of spins in each state is close to unity with the
small excess of spins being in the lower energy level NI; though the population difference is
small, it is still sufficient to be detectable. Conventionally we represent the equilibrium bulk
magnetization MO in an external field as a vector in parallel with B" (see Fig 3.1 b). [Horowitz,
1994 #53]
Relaxation
It is necessary to perturb MO away from B0 in order to measure MO independently. This is
achieved by sending in an RF pulse with frequency close to w, that flips M0 90 degrees into the
x-y plane. Mo then precesses in this plane such that we can measure the magnetization by placing
a surface coil (receiver coil) as shown in Fig 3.2. This makes use of Faraday's law to generate an
electric signal known as the free induction decay signal (FID), from the rotating magnetization.
Receiver
MO
Fig 3.2 M(, and receiver coil
9
As soon as the RF pulse ends, three things will happen: 1) M, rotates about B,, and generates an
FID 2) the transversal component of MO will decay and 3) the longitudinal component of the
magnetization will recover to its original strength. Transversal relaxation is known as spin-spin
relaxation and results from the spins interacting in such a way that they de-phase. The time for the
transversal component to decay is known as T2, hence the term T2 relaxation. The transversal
component can also dephase due to inhomogenities in the Bo field, which results in an even faster
relaxation time described by the constant T2*. In order to acquire an FID it is necessary to
refocus de-phased spins via a 180-degree pulse, known as a spin echo. Typically in an experiment
one may see a 90 degree RF pulse followed by a 180-degree pulse before which an echo can be
acquired.
Longitudinal relaxation is known as spin-lattice relaxation because spins exchange energy with
their environment as they return to their equilibrium state. The time constant associated with this
process is T1. The specific time kinetics of both TI and T2 relaxation can be described by the
Bloch equations. When the magnetization is tilted into the xy-plane, the return to equilibrium of
the magnetization along the z-axis is:
(Eq 3.5)
M,(t) = M, [1-e""")]
In MRI experiments, signals are repeatedly generated at a constant repetition time (TR), thus
establishing a steady state magnetization described by M\, = M I -e(-TRTI
1. if we wish to measure
the magnetization as an echo (while M in the transverse plane), then we have to take into account
T2 effects and the time to the echo, TE. Eq 3.5 then takes on the form:
MY
M[1-e
)] e(-
(Eq 3.6)
'E
10
3.2 Ti-Weighted Images, T2-Weighted Images, And Spin Density Images
Within any sample being imaged, different components ex. tissue vs blood, have different
relaxation constants and spin densities. By manipulating the MR pulse sequences, it is possible to
make use of a sample's inherent MR properties to create contrast between the components within
the sample being imaged. For instance in TI-weighted images, the intensity contrast between any
two tissues in an image is due mainly to the TI relaxation properties of the tissues. T2-weighted
images are weighted on T2 properties and spin density images are weighted on which substances
have more hydrogen nuclei.
To produce a TI weighted image, we use a short TE to eliminate the effect of T2 and a short TR
in order not to eliminate the effect of Ti. The topic of how to generate Ti -weighted images will
be covered in more depth later since our study relies heavily on this method. With respect to T2weighted images, these can be generated by using a long TR to eliminate the effect of TI and a
long TE in order not to eliminate the effect of T2. The third kind of image, a balanced or spin
density image, uses a long TR and a short TE thus eliminating TI and T2 effects.
Methods to Measure Ti
Two popular methods exist for measuring the TI of a biological sample, the saturation recovery
method and inversion recovery method. The main objective behind TI measurements is to
monitor the growth of M,; this can be done with from the case where M, begins at some value
other than M, or -M (saturation recovery) or the case where Mz begins at -M (inversion
recovery). Methods exist likewise to measure T2, however they are not covered here since they
were not implemented in our study.
Saturation Recovery
11
The saturation recovery technique involves flipping M,, into the transversal plane with a 90
degree pulse, then measuring the progressive re-growth of the longitudinal magnetization from 0
to M,. Measurements are made by successive steady-state experiments in which TR is varied. The
measured magnetization is fitted to the Bloch equation as shown by Eq 1.6 in order to get TI.
Inversion Recovery
With the inversion recovery method of measuring TI, the magnetization is initially flipped by
180 degrees such that M, = -M. Once perturbed M, will recover exponentially to reach
equilibrium, M. The exponential recovery of the magnetization is expressed by the following
Bloch equation:
Mz = M(
- 2 e")
(Eq 3.7)
At various times during this recovery process, Mz can be measured by flipping the magnetization
into the x-y plane and measuring it. The time between the 180-degree pulse and time at which the
M, is flipped into the transversal plane is referred to as the inversion time, TI. The inversion
recovery method requires several acquisitions over which TI is varied. The advantage over the
saturation recovery technique is the increased dynamic range of magnetization that is available
because the magnetization varies from - M, to M0 (in contrast to 0 to Mo). However the
disadvantage of the technique is that TR must be close to 5*TI in order to allow full relaxation
between experiments. Fig 3.3 shows a comparison of the data curves generated by the inversion
recovery method vs. saturation recovery method.
12
Fig 3.3 : Inversion Recovery
curves (Left), Saturation Recovery Curves (Right).
3.3 Two Dhmensional Imaging
The subject of translating a FID to a 2 dimensional image is intricate and is best understood by
breaking the discussion down into 2 main sections: K-space construction and the general format
of pulse sequences. Our discussion introduces the concepts of 2-D imaging from a mathematical
perspective and in a very brief manner; the reader is once again referred to the bibliography for a
more in-depth discussion.
K-Space & Gradients
With some basic math we can relate the spin density of a sample to the signal. We define the
following variables for our discussion:
p(r) = local spin density as a function of location r
dV = volume element
w(r)= frequency of precession as a function of location r
S(t)= total signal from sample as a function of time
Ignoring constants of proportionality and relying on a simple spin-density image, we know
dS = p(r) dV e i
13
(Eq. 3.8)
If we can manipulate the frequency w(r) in such a way that it encodes spatial location, then the
total signal S becomes a function of both space and time; this idea is achieved by using magnetic
field gradients. Instead of having one homogeneous external field B0, the field has a gradation
such that B = B 0 + Ge r, where G describes the slope of the gradient. We know w= yB (Eq 3.3),
therefore
w(r)= yB = y(Bo + G * r)
(Eq. 3.9)
Note that r represents the x, y, and z directions, and thus G can have a unique value in each of the
3 directions. Now that we have an FID that contains spatial information about the sample, the
next goal is to process the signal to construct an image.
The total on-resonance signal S(t)
p(r)e "r
=
dr
V
We define variable k = yGt/2n, so we can re-write the signal S as S(k) =
p(r)e
i2nk.rt
dr
A close inspection of the expression for S(k) shows that it is the inverse Fourier transform of the
spin density p(r). In other words by taking the Fourier transform of the total signal we can get p(r)
which allows us to construct our two dimensional image. Note that the raw signal S(k) as
represented in a two dimensional matrix is referred to as k-space; it is the inverse Fourier
transform of the final image. [Callaghan, 1993 #9]
General Format of Pulse Sequences
Gradients are necessary to spatially encode the frequencies in an FID. How the gradients are
arranged in a pulse sequence though is another topic. In an x-y-z coordinate system, 3 gradients
are necessary in MR imaging. The first gradient is referred to as the slice excitation gradient; it
defines the slice which will be imaged. The other two gradients are the "frequency encoding" and
"phase encoding" gradients. They define the two directions (e.g. x and y directions) within the
14
slice to be imaged. Figure 3.4 lists the behavior of the 3 gradients with respect to the pulse
sequence (here we show a simple spin-echo sequence).
PHASE()
()()())(0
-
(I)h, I
SLICE
|
(0
It 6 4.,;)
14 1.3)
1()()(")
(
)r
d
7-4.3)
1.5 1.3
It3 -1.4)
01
1.11 In
sinc3
TIeMt
th4S
d4
L( MPS 3 1-11.4
9 B
since
gdu e4
12fru t2
2 12111
d14
p1
d14
.4 1bt dr
litde
4 po 4 12 seltion
4 1.1 12gr ad
and4 1.1
d4 -1.6 12IN 2 1211n 14 2.4 1211u 12 (14 5.1 1211n d4 2.4 12 ou d!
lo to echo l imres NAECHOES j
-lo to slice times N,4]WCES ;I
lo to start times NA -1
111.4 (it
12u 2.5u 2t5
d14
vi. 2.511
-oto statrf
Fig 3.4 - Pulse sequence of a spin echo sequence
Note that the first gradient to be turned on is the slice selection gradient and it occurs during the
90-degree pulse. This ensures that the RF pulse excites only those spins within the slice of
interest, and any signal we see in the x-y plane is from this slice. To understand this concept
better, imagine we wish to excite a slice of thickness r centered at zo,. The RF pulse is designed to
have yG zo as the center frequency and a bandwidth of yG,'r. When the RF pulse is turned off, the
spins have de-phased relative to one another and must be rewound prior to measuring the signal.
This is accomplished by reversing the polarity of the slice selective gradient. The frequencyencoding gradient is applied only when the signal is measured; and the phase encoding gradient is
applied briefly between the time the RF pulse is terminated and the signal is measured. The
15
frequency gradient and slice select gradient do not vary during an acquisition. On the other hand,
the phase encoding gradient varies during the acquisition by increasing steadily with each phase
shift repetition.
RF Pulses
RF pulses can be defined by their shape, amplitude, and pulse length. By varying these features
one can manipulate slice excitation. It is important to note that the RF pulse is actually generated
by a B, field which lies perpendicular to B. The flip angle induced by pulse is related to the B1
excitation profile by:
0= 7
BI(t)dt
(Eq 3. 11)
This means that if a 6-millisecond pulse that was used to achieve a 90-degree excitation is scaled
to last only 3-milliseconds, then the amplitude would have to be twice as much to maintain the
same excitation. Generating the correct flip angle is one aspect of an RF pulse; the second aspect
is exciting the correct slice.
RF pulses can be described as "hard" or "soft" pulses. Hard pulses excite the full sample whereas
soft pulses excite only a portion or slice of the sample. A hard pulse is shaped as a block or
square wave. The frequency representation or Fourier transform of a block wave is a sinc wave;
thus we see that a hard pulse gives energy to all frequencies with the majority of energy centered
around one frequency, w,. Typically there is no slice selective gradient on during a hard pulse,
therefore all the spins in the sample are centered around one frequency. In the case of soft pulses
the slice selective gradient is turned on to allow for spatial selectivity. The common RF pulse
shapes used for soft pulses are Gaussian or sinc pulses. In the time domain, the sine envelope has
its first zero-crossing at t = 1/(Bandwidth). Thus the wider the bandwidth, the narrower the sinc
envelope. A sine pulse in the time domain generates a block pulse in the frequency domain; thus
in theory all the targeted frequencies are uniformly excited. The profile of a Gaussian wave in the
16
time domain is a Gaussian in the frequency domain. A property of Fourier transforms is that the
shorter length of the wave in the time domain, the longer the length in the frequency domain;
hence a shorter Gaussian pulse excites a wider bandwidth. [Finn, 1999 #54]
3.4 Spatial Resolution, Averaging, Matrix Size and Field of View
Field of View
The field of view, FOV, is determined by the phase-encoding and frequency-encoding gradients.
Remember the slice select gradient only chooses the slice, while the other two gradients frame the
slice. In order to get a smaller FOV the gradients are made steeper, a state which carried to an
extreme could stress the gradient set. The FOV as related to the gradient strength is expressed by
the following equation (for phase-encoding gradient)
FOV=
2ni
(Eq 3.10)
XGrt
where t is the time in seconds for a phase encode.
Matrix Size
The matrix size defines the number of pixels that create the final image. The size is important in
determining the spatial resolution of an image as well as the acquisition time for an image. For
instance for a given FOV, going from a 64 x 64 matrix to a 128 x 128 matrix doubles our spatial
resolution but at the same time doubles our acquisition time. Decisions on the matrix size depend
on the priorities of an experiment.
Spatial Resolution
Spatial resolution is calculated as the FOV divided by the matrix size; it is in short the pixel size
of the final image. While greater spatial resolution is better, this also implies that there are fewer
17
spins within each voxel and therefore less signal, leading to what is termed low signal-to-noise
ratio (SNR). For instance if we reduce the pixel dimensions by half, the SNR drops by a factor of
4, and in order to attain the same SNR, it is necessary to acquire 16 times more scans (i.e. average
16 times). The other extreme of too high a resolhtion is too low a resolution which leads to many
details of the image being lost (known as volume averaging).
Averaging
Averaging refers to the number of times that the data is obtained. What the MR scanner does is to
utilize multiple RF pulses and signal measurements before going on to the next phase encoding
step. Images obtained through the use of multiple excitations have a greater signal to noise ratio
and usually appear "clearer" than those obtained with only one excitation. However, this comes at
a cost; the time required for acquisition becomes multiplied by the number of excitations chosen;
in other words, averaging twice would mean that acquisition time is doubled. The SNR however
is not doubled- it increases by vr2 since signal doubles but random noise increases by
IR
f.
4. Sequences Used in Cardiac Imaging
Skeleton
4.0 Introduction - Triggering a Sequence and Segmentation
4.1 TurboFLASH/GEFI
4.2 RARE
4.3 EPI
4.4 Flow Effects
Selective vs. non-selective inversion pulses
Gradient vs. Spin Echo
4.5 CINE loops
4.0 Cardiac Imaging : Triggering and Segmentation
Perhaps the most significant difference between imaging the heart and imaging another organ is
the fact that the heart is a moving object. If during the acquisition of phase encode lines, the heart
is each time in a different spatial location, then motion artifact is introduced into the image (seen
as smearing or banding of the signal in the phase encode direction). One option to overcome this
hurdle is to acquire each phase encode at the same point in the cardiac cycle, when the heart is
relatively in the same position. In other words if 64 phase encodes are required, each phase
encode would be acquired a given time t after the R wave of the EKG, thus requiring a total of 64
heart beats to create a full image. A variation on this method is to capture several phase encodes
at a relatively stationary point in the cardiac cycle, termed segmented k-space data acquisition.
For instance if an image echo took 5ms and the isovolumetric contraction period of a heart lasted
25 ms, one could get 4 phase encodes in one heart beat; in the case of our previous example,
instead of requiring 64 heart beats to create an image, we would only need 16. The acquisiton
time for a segmented sequence can be generalized as:
Acquisition time = (length of RR interval)*matrix size/segmentation
19
Typically triggering is tied to the
Q or R wave of the ECG because both provide the most distinct
amplitude change in the ECG thus avoiding noise from other sources such as muscular
contractions. In some experiments gating is tied to both the ECG and respiration in order to
minimize motion artifact further. For small rodents such as mice and rats, some studies consider
this unneceassary since the ratio of respiration to heart rate is 1:10 [Ruff, 2000 #2 1].
The decision as to how many phase encode lines one can capture per cardiac cycle depends on
several considerations. First we must know how long the stationary period of the heart lasts. As
shown in the section on Cardiac Cycle, the diastolic period of the heart is relatively stable and
lasts atleast 100ms in CB57 L/6 mice. Even though we may have a sequence that could acquire
20 phase encodes in this window of time, T2 decay can sometimes render this attempt useless (for
instance in RARE). Another consideration is also the sequence itself, whether it has the capability
to do multiple phase-encodes within one cardiac-cycle. These issues will be presented in the
context of a number of different fast imaging sequences in the sections below. Additionally flow
effects will be discussed. Among the popular fast sequences that will be covered are
turboFLASH, RARE, and EPI.
4.1 TurboFLASH
TurboFLASH is known by several other names such as gradient echo fast imaging (GEFI), SPGR
(spoiled GRASS), and RF-FAST (RF spoiled Fourier acquired steady state). The technique is not
as fast as echo-planar imaging (EPI), however it does not require the specialized hardware
associated with EPI. The essence of the sequence is that it employs a short TR (on the order of 210 ms) followed by a pulse with flip angle a and then a gradient echo. Because the TR is too
short to allow full relaxation of the longitudinal magnetization, it does not benefit the SNR to
have a flip angle of 90 degrees after each TR. Instead the flip angle is optimized to the Ernst
20
angle, a. The relationship between the flip angle a, TR, and TI of the samriple is shown below by
Equation 4.1.
(Eq 4.1)
cos -(e "")
a
Furthermore the relative signal can be estimated as
--
T
I
T
i
1-eSGR
=M
e
(Eq 4.2)
TE '2 *
-TRITI
With human hearts, turboFLASH has enabled researchers to complete acquisition of a full image
in one cardiac cycle. One of the earliest studies to utilize a turboFLASH sequence to image the
heart was conducted by Frahm et al. At a field strength of 2.OT, the TR was made as short as
4.8ms and a = 10
0.
The result were heart images that could be acquired in 4.8ms * 64 phase
encodes = 307 ms, which meant one could afford a time resolution of one image per heart beat. In
rodent imaging, the heart rates are often so fast that it is sometimes hard to acquire one image per
heart beat. The alternative is to use a segmented turboFLASH sequence [Frahm, 1990 #30].
An inversion recovery turboFLASH sequence is a small variation in the normal turboFLASH
sequence in that it is preceeded by a 180
0
inversion pulse. Figure 4.1 shows a diagram of the
pulse sequence used in our experiment.
21
Figure 4.1 - Pulse sequence for a IR turboFLASH pulse program.
4.2 RARE & Inversion Recovery RARE
RARE imaging which stands for Rapid Acquisition with Relaxation Enhancement, is also known
by other names such as turbo spin echo (TSE) or fast spin-echo (FSE). Compared with
conventional spin echo imaging, the most important feature of RARE imaging is that several
phase-encoding lines are collected with multiple echos. The pulse sequence is shown below in
Fig 4.2. As illustrated in the figure, the RF pulse scheme includes an excitation RF pulse,
typically using a flip angle of 90 degrees, followed by several refocusing RF pulses. One can also
note that the appropriate phase-encoding gradient for each echo is applied just before the datasampling period. Subsequently just after data sampling is complete, a phase-encoding gradient for
each echo with equal amplitude but opposite polarity is applied to rewind the effect of the first
gradient. In this way, all the echoes will be encoded equivalently. RARE imaging posses many of
22
the characteristics of conventional spine echo imaging but has the important advantage of much
shorter acquisition times, which can be traded for increased resolution. RARE sequences also
provide more T2 weighting as a result of the increased TE time.
Figure 4.2 - Pulse sequence for RARE IR
Inversion Recovery RARE only differs from the normal RARE sequence by having a 180 degree
inversion pulse at the start. Like with IR turboFLASH, this adds greater TI-weighting to the
image.
4.3 EPI/ Multi-echo spoiled gradient-echo imaging
Because EPI was not implemented in this study, the sequence is discussed only briefly here.
Single-shot EPI was first introduced by Peter Mansfield in 1977. In his work, Mansfield
described the collection of the entire k-space dataset by alternating the gradient set during a single
echo after 90 degree-180 degree (spin-echo) excitation. This allows for a very rapid collection of
23
datasets with very high sequence efficiency. Gradient-echo EPI is an alternative form of EPI that
plays the readout train immediately after slice selection, increasing sequence efficiency and
reducing acquisition times. EPI has very low imaging times; sometimes entire images are taken in
40-120 ms. However it is prone to substantial image artifacts from field inhomogenities, and
susceptibility interfaces and fat [Reeder, 2000 #44].
24
4.4 Flow Effects
Selective vs. Non-selective Inversion Pulse
Inversion recovery serves to provide more TI-weighting than a regular gradient-echo or spinecho sequence. Note in Figure 4.1 of the turboFLASH sequence, that the the 180-degree pulse is
nonselective while the a -degree pulse is selective. The reason for this difference lies in
manipulating the signal of the blood. If both pulses were selective (i.e. the spins in only a given
slice were excited) then by the time the a -degree pulse were applied to the sample, some of the
spins in the blood affected by the inversion pulse would have flown out of the slice and the a degree pulse would affect fresh fully-relaxed blood entering the slice. The result is that blood may
appear brighter in an image. The assumption made here is that the time between the 180-degree
pulse and a -degree pulse (inversion time, TI) is long enough to allow non-inverted blood to flow
into the slice.
Blood in the macrovascular structures such as the ventricles and atria tends to flow rapidly during
the cardiac cycle, thus blood almost always appears bright in these structures. What about
microvascular structures? Myocardial perfusion rates in mice have been shown to be around
0.06ml/s/g, thus if we have a TI of 500ms, we lose 50% of the inverted blood spins in a slice if
we use two selective pulses.
What if were to use a non-selective inversion pulse followed by a selective a -degree pulse as
suggested in Figure 4.1? Then all the blood in the sample is excited, so that the a -degree pulse
sees no difference in the blood it affects within a given slice. The signal enhancement previously
seen in both myocardium and macrovascular structures due to blood flow is omitted with this
technique [Pettigrew, 1999 #31].
25
Gradient Echo vs. Spin Echo
Another important consideration is whether flow effects manifest themselves over the time of TE.
Because gradient echos provide short TEs (on the order of 4-5ms), we see relatively little flow
effect in the myocardium due to perfusion. The same applies to macrovascular structures if the
heart is at a quiet point in its cardiac cycle. If the heart however is in peak systole and blood is
being ejected during the time of the gradient echo, there will be some signal loss in the ventricles,
seen often times as dark spots in the ventricle.
Pulse sequences make use of either a gradient echo or spin echo in order to acquire the signal.
Each type of echo emphasizes different aspects of a cardiac image. In the case of a spin echo, the
signal is significantly less sensitive to field inhomogenities (i.e. T2* effects). Gradient echoes
though sensitive to T2* decay usually have short echo times, which minimize the effects of short
T2* commonly observed in the heart and minimize the effect of motion.
4.5 CINE imaging
In cine imaging snapshots of a particular slice of the heart are taken throughout the cardiac cycle
such that they can be strung together to create a picture of the muscle dynamics within a slice. To
make a "cine loop", images of a slice are taken at differing times in the cycle by varying the
sequence's trigger point relative to the R wave. To get a sense of the acquisition times required to
make a cine movie, assume we use a single gradient-echo sequence with TR equal to the RR
interval. If we wish to fill a square matrix of dimension N and gather P number of images of the
cardiac cycle, then the acquisition time would be
Acquisition time = N * P * (RR interval)
26
Typically the interest is to create a cine movie of several slices of the heart rather than one. We
can excite a single slice, acquire a signal from it, and then wait TR for it to recover before
repeating the process. If we have S slices, the acquisition time becomes
Acquisition time = S * N * P * (RR interval)
A more efficient method for multi-slice CINE imaging is to interleave the acquisition. During the
TR for one slice, it is possible to excite another slice or multiple slices such that the acquisition
points for all the slices will be interspersed throughout the cardiac cycle. This method can
sometimes drop the acquisition time to N * P * (RR interval). One important consideration is that
adjacent slices should not be imaged consecutively since excitation of one slice may bleed into
the other (due to imprecise slice excitation by RF pulse).
27
5. Methods in Myocardial Perfusion Analysis
Skeleton
5.0 Introduction - what is perfusion? What are perfusion-defects?
5.1 Where we currently are in perfusion defect detection in large mammals such as humans. A
break down of the various methods.
Exogenous Methods
5.1.1 First Pass -- Theory. Experimental needs. Qualitative & quantitative studies.
5.1.2 Blood Volume - Theory & Experimental concerns. Data. Contrast Agents.
5.1.3 Other Recent Exogenous Methods - Necrotic-avid tracers & ion contrast media
Endogenous Methods
5.2.1 T2 weighted images - brief theory.
5.2.2 MTC - magnetization transfer contrast- theory & most pertinent study so far.
5.2.3 BOLD - theory and explanation of myocardial studies.
5.2.4 ASL & FAIR - theory
5.2.5 Intravoxel Incoherent Method (IVIM) - brief description. No theory this time.
5.3 Where we are with smaller animals such as rats and mice. A breakdown of methods used in
small mammals.
5.0 Introduction
Since scientists aim to investigate the viability and function of a tissue, being able to study the
perfusion level in myocardial tissue is of great interest to those in cardiology. Perfusion is defined
as milliliters of arterial blood entering 1 OOg of tissue per minute and is in essence a process which
controls the delivery of nutrients to tissue. Perfusion, f, can be calculated as :
f= F/V where
F
arterial blood rate (ml/min)
V
tissue volume (ml).
(Eq 5.1)
Often times the strict meaning of perfusion has been relaxed so that in some literature, the term
refers to the degree of normal or abnormal vasculature in a tissue. Perfusion has sometimes been
confused also for referring to blood-tissue exchange. An analogy is helpful in steering clear from
confusion on this point. Imagine a radiator in a room. Perfusion is similar to measuring the water
flow through the radiator. It is not to be confused with the amount of heat transferred from the
radiator to the surrounding enviromnent nor the number of pipes- though these parameters are
related to perfusion [Pettigrew, 1999 #31].
This section covers the current techniques implemented to detect perfusion defects in the
myocardium. By perfusion defects we mean regions of the myocardium where the perfusion level
is lower than normal/healthy myocardium for the particular species under investigation; note this
definition encompasses ischemic and infarcted myocardium. The summary of current MR
techniques is broken down into those utilized for larger manunals such as humans and pigs and
those that have been applied to smaller animals such as rats and mice. This separation is
necessary since many of the techniques described for large animals are hard to apply to rats/mice
at a given field strength due to their smaller heart sizes and faster heart rates.
5.2 Current Perfusion Analysis Methods for Large Mammals
Perfusion imaging techniques can be broken down into two main categories: exogenous contrast
techniques and endogenous contrast techniques. In exogenous contrast techniques a relaxivity
agent is injected into the region of interest and the region then imaged either for tracer timekinetics or for the tissue's state under steady-state conditions to ascertain useful physiologic
information. A relaxivity agent is a drug that reduces the relaxation time (TI and T2) of water
protons in the sample being imaged. Typical relaxivity agents used are paramagnetic chelates,
most notably gadolinium-DTPA (Gd-DTPA). Gd-DTPA decreases both TI and T2 rates but is
29
known as a TI agent because rate constant changes based on a percentage are much greater for
TI compared to T2. Among the most popular imaging methods for measuring perfusion with
exogenous agents are first-pass and blood volume methods, which are explained in detail in the
sections below. In first pass studies a bolus of contrast agent is injected and the time kinetics of
the contrast agent are studied in the tissue to determine perfusion. In blood volume studies, an
intravascular contrast agent is injected into the body and allowed to reach steady-state. Because
an intravascular agent does not leave the vascular space, one can equate blood volume to the
volume in which the agent is restricted. Though blood volume is not a direct parameter to
detecting perfusion defects, it is strongly correlated to perfusion levels [Pottumarthi, 1995 #28].
Endogenous contrast techniques make use of the tissue or blood's inherent properties to gather
physiologic information. There are a number of such techniques. One common technique known
as BOLD uses the blood as a contrast agent. Oxygenated blood is diamagnetic and becomes
paramagnetic when deoxygenated. A boundary interfacing the paramagnetic venous blood and
tissue generates susceptibility effects that can seen in an MR image. Therefore an increase in
regional blood flow means blood is better oxygenated which in turn will be reflected in the MR
scan. Another endogenous contrast technique is the intravoxel incoherent motion method (IVIM).
Based on its sensitivity to diffusion effects, IVIM assumes that the motion in capillaries is similar
to that of random diffusional motion and attempts to detect this. The method proves to be
complicated and indirect in its measurement of perfusion [James, 1998 #33]. A third approach
uses magnetically tagged endogenous water (sometimes referred to as FAIR, Flow-sensitive
Alternating Inversion Recovery, or ASL, Arterial Spin Labelling). In this method a flow-sensitive
image is subtracted from a flow insensitive image [Andersen, 2000 #55].
Below is a more indepth look at the exogenous and endogenous contrast techniques already
touched upon plus some additional techniques that have been developed in the last two years.
30
,
141
,
,
-
-
-
-
-
-
--
--
-
--
Exogenous Techniques
5.1.1 Bolus Tracking/First Pass
Over 500 studies have been conducted on patients utilizing MR first pass techniques. The basic
technique involves injecting a contrast agent as a bolus into the patient and then observing the
time kinetics of the chemical in the tissue. Regional myocardium with perfusion defects will have
different enhancement patterns over time as compared to normal myocardium. An example can
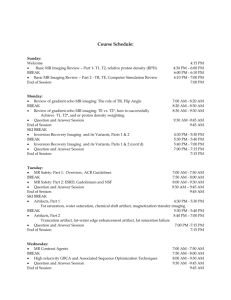
be seen in Figure 5.1 where the abnormal region shows early hypoenhancement after the patient
is injected with Gd-DTPA.
Figure 5.1- First-pass pictures of myocardium showing early hypoenhancement (ischemic region).
Theory
The theory behind MR first pass imaging is based on the earlier indicator-dilution methods
employed in nuclear medicine for studying perfusion. When a nondiffusible contrast agent is
injected into the bloodstream in the form of a bolus, the movement of blood through an organ can
be studied by observing the signal intensity changes over time induced by the blood flow.
Changes are due in part to two reasons- relaxivity effects and susceptibilty effects. The presence
of a contrast agent decreases the TI and T2 of blood and tissue. The high susceptibility of the
contrast agent also produces steep, localized magnetic fields that are reflected in a decrease of
31
-==LA-
-
-
T2*. Whether relaxivity or susceptibility effects dominate in an image depends on the imaging
sequence used. [Pettigrew, 1999 #31]
Assuming one adheres to certain experimental criteria to obtain concentration-time curves, the
next step is to extract the relevant perfusion information from the data. This can be done using the
central volume principle which states that absolute blood flow (BF) is:
BF = Vd/MTT
Equation 5.2
where V, is the volume fraction of the contrast agent in a tissue and MTT is the mean transit time.
V, for a freely diffusible agent is equal to 1 since the chemical diffuses throughout the entire
tissue. In the case of an intravascular agent, V is equal to the blood volume Vb (blood volume is
defined as the fraction of tissue occupied by blood). MTT, the mean transit time, refers to the
average time required for a particle of tracer to pass through the tissue.
V, can be calculated directly from the concentration-time curves as
Vd =
,,_._t
. Caiea(t)dt
MTT can be derived from the concentration time curves by calculating the first moment of the
measured concentration-time curve for tissue (this is an estimation of the indicator-dilution
methods rather than a precise measure). In the above manner it is possible to apply the central
volume principle to the concentration-time curves to get a a rough quantitative measure of
perfusion [Pottumarthi, 1995 #28].
32
Experimental Procedures
Given the theory, it is possible to use a number of different contrast agents and a number of
different arterial input functions to measure perfusion. In order to simplify computations and
avoid complex deconvolutions, studies often aim to inject a bolus of contrast agent into the
patient, thus allowing the arterial input function to be approximated as an impulse. Bolus
injections are not a necessity; a number of studies have shown it is possible to use other arterial
input functions, however it does make computations simpler. Another experimental concern is
monitoring the time kinetics of the contrast agent as it passes through the organ. Since mean
transit times can be fast, first-pass necessitates rapid imaging procedures such as EPI and
turboFLASH. For instance in the case of a patient with a heart rate of 50-90 beats/minutes,
acquisition should occur every 1 or 2 seconds [Pettigrew, 1999 #31].
Choosing a contrast agent can also impact experimental procedures since it effects the MTTs and
volume fraction distribution Vd. In the case that an intravascular agent is used, the volume
fraction of the contrast agent Vd reflects the blood volume, a bonus piece of information.
However intravascular agents have a short mean transit time meaning myocardial signal intensity
should be sampled quickly in order to get accurate concentration curves. It is possible to conduct
first pass studies with non-intravascular agents as well and get slower MTTs. For instance one
study attempted to use P760, a gadolinium chelate with slow interstitial diffusion and high
relaxivity and found it to work reliably well in pigs [Kroft, 1999 #56]. Some studies have also
used non-proton contrast agents such as F' 9 . Since this species does not appear in the body in
significant quantities, there is little confusion in tracking the diffusion pattern of this contrast
agent [Pottumarthi, 1995 #28].
One other issue that needs to be kept in mind is that MRI does not directly measure the contrast
agent concentration; the latter is determined by a measure of TI or T2. However calculating
33
contrast agent concentration from TI and T2 and requires a knowledge of the exhange rate of
water betweeen the various tissue compartments [Donahue, 1994 #60]. This is an area under
active investigation.
Qualitative & Quantitative Data
Qualitative studies have shown that the enhancement patterns of tissue over time are capable of
revealing regions of perfusion defects and furthermore describing the type of defect. For instance
patient studies with Gd-DTPA show that in TI weighted first pass images, areas of delayed
hyperenhancement compared well with areas of irreversible myocardial damage, known as "fixed
defects" [#5, #38]. In general under steady-state conditions, it has been shown that with GdDTPA, infarcted areas have a greater signal intensity than normal myocardium.
A number of quantitative studies using first-pass methods have been conducted on humans, pigs,
and other large mammals. Results of the technique have corresponded closely with histological
measurements peformed with microspheres, and first pass has become established as a reliable
method of ascertaining estimates of myocardial perfusion [Kroft, 1999 #56].
5.1.2 Blood Volume
Blood volume, V,, is defined as the fraction of a tissue volume occupied by blood. While in
theory V, for a tissue sample need not correspond to perfusion, experiments have shown a strong
correlation between the two parameters; thus ischemic or infarcted areas can often be spotted
through blood volume studies [Pottumarthi, 1995 #28]. Like in first pass studies, most blood
volume studies involve the use of a contrast agent. The agent is injected into the patient and TI or
T2 images are captured after the myocardiumn reaches a steady-state. One notable advantage of
blood volume studies over first pass techniques is that the state of the tissue does not need to be
34
studied over a time course, therefore eliminating the need for fast imaging sequences. Figure 5.2
below displays an example of a blood volume study in which Gd-DTPA was used in an ex vivo
and a T1 image captured. The bright areas in the myocardium reflects the infarcted tissue and can
be seen to correlate with TTC staining.
Figure 5.2- Blood volume pictures with Gd-DTPA showing infarcted area as hyperenhanced. MR images on
right and corresponding TTC stains on left.
Theory & Experimental Procedures
This section briefly covers the theory behind computing reginonal blood volume (RBV); for a
more detailed understanding refer to the section on "Tissue Models for RBV". As explained in
the section on first pass imaging, one can calculate the blood volume of a tissue by using an
intravascular agent and acquiring concentration-time curves. Applying the equation below we can
extract from the cocentration curves, the volume distribution fraction of the agent
this case is equal to the blood volume:
35
Vd
which in
Vd =
tssuetdt
.f Caena(t)dt
If we allow t to go to infinity, i.e. allow the system to reach steady-state, we can approximate V,
as the concentration of agent in the tissue divided by the concentration of agent in arterial blood.
The process of calculating concentration curves from image maps can be cumbersome and so
most studies use an related method to measure the blood volume in myocardium. By measuring
the Ti of a tissue sample before an intravascular agent is administered and then measuring it
again after administration, one can apply the equation below to get an approximation of the
regional blood volume:
Vb=
I /IP-1I/TI
1/T ipre_
MIA
1/T1,osI
Typically studies inject multiple doses of a contrast agent to get multiple T I maps and thus gather
more reliable data on the blood volume levels in myocardium. The use of multiple T I maps also
has another advantage. Equation 2 is a simplification of a more complicated equation which
includes the effects of perfusion to get a more accurate estimate of V. In order to use the more
precise equation, multiple TI maps are required [Kahler, 1998 #27]. For the purposes of keeping
this discussion simple, this equation nor method will be fully explored in this section (please refer
to the section on Tissue Models for more details).
Quantitative & Qualitative Data
While quantifying regional blood volume is useful in detecting perfusion defects, it is possible to
also rely on qualitative data. Steady-state images after administration of a contrast agent such as
36
Gd-DTPA have clearly shown that ischemic areas appear darker/brighter than normal
myocardium in TI-weighted images. An example of this behavior can be seen in Figure 5.2. This
result is based on the fact that the contrast agent, which shortens TIs, travels via the blood and is
able to effect ischemic areas less than normal myocardium due to depressed blood volumes.
Studies have been conducted to determine the relationship between qualitative detection of
ischemic/infarct detection using blood volume and first-pass methods. This relationship obviously
depends in part on the contrast agent used. One study compared the effectiveness of contrast
enhanced Gd-DTPA TI-weighted blood volume and MR first-pass imaging for accurately
estimating the size of infarcted regions in pigs. Steady state Gd-DTPA TI-weighted images
showed that the areas of abnormal signal intensity were larger than the defective areas spotted by
first-pass. By comparing the MR results against histology, the conclusion made by the study is
that first-pass is effective in detecting infarcted areas while the other technique seems to include
the peri-infarct. The peri-infarct area or boreder zone is defined as the area of reversibly injured
myocardium adjacent to the core of an infarct [#3, #34].
Contrast Agents
Both extracellular and intravascular agents can be used to study blood volume, however
intravascular agents (blood pool agents) provide better estimates of blood volume. These agents
cannot pass the capillary pores because of their molecular weight (usually on the order of 12-150
kDa) and thus stays in the blood for long periods of time unlike extracellular agents which
dissipate into the interstitial area. A number of studies have been conducted in the past to verify
the effectiveness of different contrast agents in blood volume studies. Among the newest agents
to be used are gadolinium chelates such as Gd-BSA and Gd-polysine. While most contrast agents
seem best imaged with TI-weighted sequences, there are agents that benefit from T2-weighted
images. For instance one study used a ultrasmall superparamagnetic ironoxide (USPIO)
preparation known as NC 100150 and found that imaging with a T2-weighted turbo spin echo
37
sequence gave the reliable indications of differences in myocardial blood volume [Bjerner, 2000
#43].
5.1.3 Other Methods Which Employ an Agent
Researchers have also investigated the use of nectrotic-avid agents such as gadophrin-2 to detect
a class of perfusion defects, infarcted/nectrotic tissue, and have met with promising results.
Studies suggest that necrosis-avid tracers might even be more precise in defining necrotic areas
than agents such as Gd-DTPA, which are said to overestimate infarcted areas by about 10%. The
downside of this agent is that it takes 1-3 hours after administration before imaging can take
place. Note that this contrast agent does not fall within the scope of blood volume studies since
agent concentrations in myocardium depend on the amount of necrotic tissue rather than blood in
a tissue [Pislaru, 1999 #45].
Similar to necrotic-avid tracer methods are ion contrast media methods such as "Na, twentrythree sodium, MRI. This method is based on the fact that irreversible myocardial injury and
myocyte death are characterized by loss of cellular membrane integrity and of normal
electrochemical ion gradients resulting in accumulation of intracelullar sodium and water in
necrotic cells. Although it is possible to detect these increases in intracellular sodium by
administering "Na, these agents cannot be used in vivo because of their high toxicity. More
recent studies suggest that total sodium may be used as an indictation of ischemia [Gerber BL,
Top Magn Reson Imaging #8]. MnDPDP (manganese dipyridoxyl diphosphate), also known as
Teslascan, works in a similar way. When administered in a patient, manganese cations are
released into the blood stream and quickly absorbed by viable myocardial cells via voltagedependent calcium channels and retained. The result is that the uptake of myocardium is high in
normal myocardium as compared with infarcted tissue and differing levels of uptake can then be
38
spotted with Ti-imaging [Bremerich J, 2000 #5]. As with necrotic-avid tracers, ion contrast
media are helpful in detecting infarcted regions and not other perfusion-limited areas such as
ischemic regions [Wendland, 1999 #47].
Figure 5.3 - Example of Sodium-23 image where bright area with arrows shows infarcted region.
Endogenous Techniques
5.2.1 T2 Weighted Studies
Studies have reported that TI-weighted imaging without exogenous contrast agents provides little
or no information on perfusion defects in myocardium. However the same cannot be said for T2weighted imaging; infarcted areas have been shown to be detectable with T2-weighted MRI and
show up as hyperintense regions [Lim, 1999 #34]. A study by Lim and Choi showed that the
diagnostic concordance rate between T2-weighted MRI and rest thallium SPECT was 95% when
analyzing infarcted areas. The downside of this technique, however, is it does not identify chronic
infarcts (i.e. reversible vs irreversible damage) and may overestimate infarct size by including
areas at risk. T2-weighted images also often have a low signal-to-noise ratio compared with
contrast-enhanced perfusion imaging which provides better-quality images [Gerber BL, Top
Magn Reson Imaging #8].
39
.....
....
..
Figure 5.4 - Example of T2 weighted image for detection of ischemic region. Hyperintense area denotes
ischemic region.
5.2.2 Magnetization Transfer Contrast (MTC)
One technique which makes use of the inherent longitudinal magnetization properties of
myocardial tissue in order to obviate the need for exogenous contrast agents is Magnetization
Transfer Contrast (MTC) imaging. MTC is based on the saturation transfer method being applied
to biological tissue. This method relies on magnetization transfer between tissue water with
1
restricted motion, referred to as 'H, and "free" bulk water with unrestricted motion, Hf.
Examples of 'H, include water in cellular membranes and macromolecular matrices. By
selectively saturating the 'H, spins, magnetization transfer occurs between 'H, spins and 'Hf spins,
and this can be seen in an image as a signal intensity drop in 'Hf. It has been shown that surface
hydroxyl and/or amine groups on macromolecular surfaces appear to be necessary for
magnetization transfer. These groups presumably orient water protons in close proximity to
macromolecular protons for a time sufficient to allow magnetization transfer to occur. Several
tissues have been shown to have the necessary physiochemical properties for significant
magnetization transfer including myocardium, skeletal muscle, skin, and articular cartilage.
Figure 5.5 diagrams the interaction between water spins in an MTC experiment [Scholz, 1993
#50].
40
'Oaundaw9
Mae. cmleeulir M-MA
Ze'4
H
Hee'~
'QO.A
H
Water
H
H
0
N
H
H
VA"
H
H~H
H
Figure 5.5 Description of molecular interactions and MT.
Studies have shown that both MT-weighted signal intensity and T18 increase with an increase in
flow rate, thus imaging sequences that weight based on both these parameters can detect relative
differences in perfusion levels. Note Tl13 is defined as the spin-lattice relaxation time of 'Hf in the
presence of 'H saturation. An example of some images acquired by this method on an isolated
heart are shown in Figure 5.6. One can note the efficiency of this method as related to TI imaging
with Gd-DTPA. In this particular study imaging was done with MT preparation pulses followed
by an inversion recovery turboFLASH sequence. The TI for the inversion recovery pulse was
chosen to almost null normal myocardium (not completely), i.e. close to the zero crossing of the
tissue. Since MR images are usually displayed as absolute magnitude values, the Ti-weighted
image intensity taken at a zero-crossing will increase with any change in longitudinal equilibrium
magnetization. Similarly with TI, the absolute magnitude of the TI-weighted signal intensity will
increase for changes in TI values [Prasad, 1993 #5 7].
41
-M
I
M
M
M
Figure 5.6 -Example of MT images compared with Gd image.
5.2.3 BOLD
BOLD which stands for blood oxygen level dependent contrast, relies on the paramagnetic and
diamagnetic properties of blood. Deoxyhemoglobin is a paramagnetic molecule whereas
oxyhemoglobin is diamagnetic. The presence of deoxyhemoglobin in a blood vessel causes a
susceptibility difference between the vessel and its surrounding tissue, in other words between
venous blood and tissue. Such susceptibility differences cause dephasing of the MR proton signal,
leading to a reduction in the value of T2*. In a T2* weighted imaging experiment, the presence of
deoxyhemoglobin in the blood vessels causes a darkening of the image in those voxels containing
vessels. Since oxyhemoglobin is diamagnetic and does not produce the same dephasing, changes
in oxygenation of the blood can be observed as the signal changes in T2* weighted images
[Miller, 2000 #48]. BOLD has been a technique primarily used in fMRI but some perfusion
studies in cardiac imaging have used it as well. Currently no published literature shows that
studies have been conducted directly on ischemic tissue detection using BOLD. Instead most of
the work has been to prove that a relative change in the perfusion level of overall human
myocardium can be detected with this method [Eng, 1991 #49].
42
5.2.4 Arterial Spin-Labelling (ASL) / Flow-sensitive Alternating Inversion Recovery (FAIR)
Theory
Arterial spin-labelling is in essence a technique that uses water as an endogenous contrast agent.
By manipulating the spins at the inflow point of a targeted organ, for instance by inverting them,
the spins act almost as a tracer. The labelled spins specifically affect the nuclear magnetization in
the organ by reducing the magnetization in areas where flow is high (noted in Eq 5.3). The
specific relationship between the magnetization and blood flow can be seen by a modification of
the Bloch equations as listed in Eq 5.1 below:
dMb(t) = M 0" - MbL) + fM.(t) - fM~t)
dt
T,
(Eq 5.1)
f= perfusion (ml/g/s)
Ma = magnetization of arterial blood per ml
Mb
T,
=magnetization of organ (in this example we refer to the brain) per gm
the TI of tissue in the absence of flow
X the blood-brain coefficient =(amt water/g brain)/(amt vater/ml blood)
With some assumptions, we can massage Equation 5.1 such that the magnetization in the tissue is
expressed as an exponential decay in Mb with a time constant Tapp given by the following
expression:
1
1 + f
T 1v
T1
(Eq 5.2)
X
Steady state is expressed as
Mbss =
Mb (1-fTiLX)
(Eq 5.3)
(1+fT 1/ X)
43
Both of the above quantities can be investigated with proper MR imaging techniques and then the
results used to calculate perfusion f From equations 5.2 & 5.3, we show that
f=
k*
Tapp
Mb"-Mb"'
(Eq 5.4)
2 Mb'
In the case of continuous ASL, the spins are continuously inverted whereas in pulsed ASL, the
spins of the arterial blood are labelled at a single point in time, and an image acquired after the
spin-labelled blood has been allowed to wash into the organ. Often times continuous ASL is
useful when attempting to measure steady state conditions for the purposes of quantifying
perfusion (look at Eq 5.4).
With both continuous and pulsed methods, the signal intensity of an image acquired following
arterial spin inversion is reduced by an amount that is directly related to perfusion. If a second
image is obtained without the preceding arterial spin inversion, subtraction of the first image from
the second results in a perfusion-weighted image. From this process, perfusion maps can be
generated [Williams, 1992 #51]. Subtraction of a flow-sensitive image from a flow-insensitive
one is also known as FAIR, Flow-sensitive Alternating Inversion Recovery [Andersen, 2000
#55]. While the methods described so far use inverted spins to affect the imaging slice, other
variations of this technique choose to invert the spins in the imaging slice and allow arterial blood
to flow in as fully relaxed spins [Waller, 2000 #52]. Like BOLD techniques, ASL has been
mainly used in brain studies however the few cardiac perfusion studies published on ASL have
shown promising results [Williams, 1992 #51].
44
5.2.5 Intravoxel Incoherent Method (IVIM)
To the best knowledge of this write-up, no studies have been published using IVIM as a method
for myocardial perfusion studies in any mammal. Most IVIM studies in perfusion have been
targeted at other organs such as the kidney and brain. The method itself is based on measuring the
amount of diffusion in a given sample. When one considers a voxel under a gradient, spins in the
voxel may move in different directions with differing velocities and thus experience random
phase shifts which in turn attenuate the overall magnetization. Perfusion can be considered such a
kind of incoherent motion (i.e. similar to molecular diffusion). In order to avoid excess detail and
complicated concepts, the theory is ommitted for this method and further information can be
found in the Bibliography [Pettigrew, 1999 #31].
5.3 Perfusion-Analysis Techniques for Small Mammals
General MR techniques have been developed to study perfusion-defects as elucidated in the
previous section, however these methods work mainly for large mammals such as humans and
pigs. When working with rats and mice at similar field strengths, several of these methods have to
be adapted to compensate for faster heart rates and smaller fields of view. At present, no literature
has been published on studies of perfusion defects in mice. The most relevant studies to the topic
of perfusion defects in small mammals are those done on rats. Table 5.1 below presents a
summary of the imaging techniques that have been applied to rat hearts as well as the lowest field
strengths for which these techniques have been applied.
In choosing one technique that would work to image mice, we need a technique that would give
us good SNR for a 1-1.5 mm slice thickness and an inplane resolution around or less than 350
microns. Given the previous rat studies listed below, the most promising techniques seem to be
first pass and blood volume techniques. Nectrotic-avid tracers may also have potential though
they detect only one class of perfusion defects, infarcted tissue.
45
Table 5.1. MR Perfusion Techniques applied to Rat Hearts
Method Employed
Lowest Field Used
Associated Parameters at Specified Field
Strength
First Pass
4.7T
Resolution 156 micron; slice thickness 2mm.
(excised heart though)
Blood Volume
2.0 T
Gd-BSA used. Resolution 625 micron; slice
thickness 3mm.
Necrotic/Ion Avid Tracers
2.0 T
manganese dipyridoxyl diphosphate (Mn-DPDP).
Resolution 780 micron; 2mm slice thickness.
T2 Weighted Images
none
None
Magnetization Transfer Contrast (MTC)
4.7 T
resolution 468 micron, 3mm slice thickness
BOLD
none
None
7T
Arterial Spin-Labelling
IVIM
none
46
234 micron, 3mm slice thickness
None
6. Previous Cardiac MRI Studies on Mice
Skeleton:
6.0 Intro paragraph + First study done on mice.
6.1 1 st Group of studies- studies on hypertrophied hearts,
6.2 2nd Group of studies - studies on functional parameters
6.3 3rd Group of studies - even higher resolutions.
6.4 Conclusion
6.0 Introduction
Due to the fast heart rate and small size of the murie heart, cardiac MR imaging in mice has
posed some challenges to scientists. It has not been until this last decade that several articles on
this topic have surfaced. To the best of my knowledge, there are about twelve main papers
dealing with the topic of cardiac MR imaging in mice. One of the earliest of these published
studies was presented by Stephen Rose et al. in 1994 [Rose, 1994 #19]. The aim of the study was
to show that cardiac imaging in mice and rats was possible with high resolution and flow
suppression. Using magnets with field strengths of 7 T and 9.4 T, they were able to capture
multiple axial slices of the heart with a slice thickness of 1- 1.5mm and a voxel resolution of 97
pm 2. Flow suppression was achieved by using a spin echo sequence combined with gradient
refocusing (Fig 6.1). In this sequence, a 90 degree pulse flips the magnetization into the tranverse
plane. A gradient then dephases the flows such that when the 180 degree pulse is sent, we get a
spin echo but with minimal flow contribution.
47
90 (x)
180 (y)
90 (-x)
Pulses
Flow Dephasing Gradients
Fig 6.1 . Sequence used for Flow Suppression Imaging
6.1 Hypertrophy Studies in Murine Hearts
Subsequent studies also attempted to get high quality images of murine hearts but with a focus on
those mice that displayed physical deviations in the cardiac anatomy. For instance Siri et al.
attempted to quantitatively measure left ventricular mass in mice with two goals: 1) to show they
could detect hypertrophied hearts with MRI and 2) to prove that MRI was a more accurate tool
than echocardiography for this purpose. They captured proton images with a 9.4 T magnet and
achieved resolutions on the order of 156 E m2 with a slice thickness of Imm. The results in
comparison to echocardiography showed MR imaging to be more accurate [Siri, 1997 #22]. Other
papers published around this time also began to toute MRI as a superior tool in imaging muring
hearts for physical abnormalities [Christensen, 1997 #32].
Studies targeted at imaging hypertrophy were also conducted by Franco et al. [Franco, 1998 #16]
and Slawson et al. [Slawson, 1998 #23]. Slawson induced an increase in heart weight using
isoproterenol and then used a spin warp sequence on a 7T magnet (resolution= 195 Em 2) to image
the mice. His studies accurately detected the 25-30% increase in ventricular wall thickness caused
by the isoproterenol. Additionally he was able to get such information as the ejection fraction of
the heart. Franco et al. also measured hypertrophy for the purposes of assessing the cardiac
physiology of mice with a dysfunctional guanylyl cyclase A gene (GCA -/-). Her work was
48
pertinent in that she successfully imaged murine hearts at a 1. 5T field strength, a much weaker
field strength than had been previously used. Implementing a turboFLASH sequence she was able
to get a voxel resolution of 190 F m2 and a slice thickness of 1.6mm.
Another study that utilized MRI to detect hypertrophy was led by Jelicks et al [Jelicks, 1999 #18].
The aim of their study was to gather morphological information about mice infected with Chagas
disease. They imaged at a high field strength (9.4T) and found evidence of changes in ventricular
wall thickness in infected mice. While they decided to use a spin-echo sequence in their imaging
protocol, they also reported having tried EPI and gradient recalled echo imaging (this seems to be
the first published article that discusses these two sequences as they relate to mice). These
sequences were rejected in favor of a spin-echo sequence because the signal to noise ratio was
low.
6.2 Functional Assessment of Murine Hearts
By imaging the ventricular volume of the heart at different points in the cardiac cycle (i.e. systole
and diastole), it is possible to infer functional parameters such as ejection fraction and stroke
volume. Studies done by both Bryant et al. and Ruff et al. targeted the quantification of these
parameters through cardiac MR imaging [#14, #2 1]. In the case of the study by Bryant,
investigations attempted to understand the effects of TNF production on cardiac myocytes (TNF
= tumor necrosis factor, which is a multifunctional cytokine). Using gated gradient echo
sequences (GEFI) on a 1.5 T magnet, they were able to show that TNF production led to
biventricular dilation and depressed ejection fractions.
49
Similarly Ruff et al implemented a turboFLASH sequence on a 7T magnet to measure stroke
volume, ejection fraction, and myocardial mass in normal mice. The images he gathered were at a
117 pm2 resolution and show remarkable detail.
One paper that deviated from measuring typical functional parameters was presented by Henson
et al [Henson, 2000 #17]. Their investigations attempt to quantify the degree of left ventricular
torsion in murine hearts with the goal of better understanding the underlying shearing motion of
the myofibrils responsible for cardiac contraction. The study conducted at 4.7T, implemented a
well-known technique in MRI termed myocardial tagging, in which fiducial markers are placed
on the myocardium and tracked. Results showed that the torsion angles when normalized to
ventricular lengths were almost equal in mice and humans.
Another study that provided new functional information on the murine heart was published by
Chacko et al [Chacko, 2000 #15]. One of the aims in their work is to implement P3 ' MRI techniques in mice in order to non-invasively study cardiac metabolism and function. Adapted from
previous techinques used to assess PCr-to-ATP ratios in humans, the technique they developed
revealed that mice and humans have similar PCr/ATP ratios.
6.3 Imaging Murine Hearts at Higher Resolutions
Recent articles published within the last year on the topic of murine cardiac imaging have
seemingly been focused on obtaining higher resolution. In particular a study conducted by Ruff et
al investigated the feasibility of using MRI to explore cardiac mircostructures and coronary
vessels in mice [Ruff, 2000 #21]. By experimenting with a number of sequences - segmented 2D
FLASH, conventional 3D gradient echo, and segmented 3D FLASH- they were able to decide the
optimal sequence was a 3D multiple thin slab sequence. Running this sequence on a 7T magnet,
50
they imaged at spatial resolutions of 100 x 100 x 200 ptml which allowed for remarkable
visualization of the left coronary artery and other microstructures. Of all the articles that have
been published till now on murine cardiac images, this one provides the greatest detail in terms of
cardiac structures.
Another study by the same group that also targeted higher resolutions was conducted by
Wiesmann et al. [Wiesmann, 2000 #24]. The goal of their study was to determine whether MRI
could be used to characterize cardiac function in newborn, juvenile, and adult mice. By using a
turboFLASH sequence on a 7.05 T magnet, they were able to increase temporal and spatial
resolutions to 8.6ms and 78-117 ptm 2 respectively. This study is supposedly the first published
document on imaging neonate and infant mouse hearts.
6.4 Conclusion
The majority of the articles that pertain to cardiac MRIs of the murine heart deal mainly with
gathering morphological information about the heart. The remainder investigate the potential of
MRI to gather functional information about the heart, but to the best of my knowledge, no article
has been published up to now on the topic of detecting perfusion defects in murine inyocardiun.
Such a contribution would help uncover other potential uses for MRI in the field of murine
cardiac imaging.
51
7. Tissue Models
Skeleton:
7.0 Two-compartment model
7.1 Fast-exchange model
7.2 Exchange-diffusion Model
7.3 Bauer's Secondary Model Which Includes Perfusion Effects
7.0 Two-compartment model
One of the most popular models for perfusion and blood volume studies is the
two-compartment model. In this model the myocardium is represented as a composition of
arterial blood and tissue, where tissue can be further broken down into two compartments itself,
capillary blood and the extravascular space. Even though the extravascular space is
inhomogeneous, it is possible to treat the space as one homogeneous compartment because in
tissues with high capillary density (e.g. myocardium), the mean transit time of spins from
extravascular space to capillary wall is relatively small. One important aspect to note is that the
TI of arterial blood is not the same as the TI of capillary blood. Because oxygenation and
hematocrit levels influence TI and the level of these elements are different in the two
compartments, the relaxivity times between arterial and capillary blood are different
[Schwarzbauer, 1993 #41].
Having defined the different compartments, two main processes are involved in the
exchange of blood amongst them. The first, perfusion, describes blood exchange between the
arterial blood supply and the capillary supply. The secondary process involved in blood exchange
is diffusion; diffusion describes blood exchange between the capillary and the extravascular
space.
52
In the case of perfusion defect detection studies, the assumption is that the ischemic area
suffers poor perfusion and therefore very little arterial blood reaches the tissue space. This case is
described by capillary I in Figure 7.1 below. Previous studies have shown that without a contrast
agent it is very hard to distinguish the signal intensity between infarcted tissue and healthy tissue.
This problem is overcome by the use of an intravascular contrast agent (IVCA). When an IVCA
such as Gd-BSA is introduced, the TI of arterial blood is shortened and areas receiving arterial
blood (i.e. well-perfused areas or healthy tissue) likewise have a shorter TI. The relaxivity rate
for infarcted tissue remains minimally altered. On a normal T I -weighted image the infarct would
show as an area darker than healthy tissue [Bauer, 1992 #42].
C E C E C
C E C E C
AAA
Capilarv I - no perfusion
E E EE
A CAC
Capillary 2 - no diffusion
AC EACE
E A ACAEC
Capillary 3 - with diffusion & perfusion
Figure 7.1 : Two Compartment Model
7.1 Fast-exchange model
The above two-compartment model describes a method of qualitatively detecting
infarcted regions. Typically to get quantitative information, a complex system
encompassing relaxivity rates, spin densities, volume fractions, geometry of vessels and
more would have to be designed. In early blood volume studies such as that done by
Schwarzbauer et al. (27), many of these details were skipped and a simpler model known
as the fast-exchange model was created. The model assumes that diffusion between the
capillaries and the extravascular space of tissue is fast enough that the tissue space can be
treated as one element having one spin-lattice relaxation rate. In other words the average
53
time that spins stay in a compartment is much less than the TI associated with those
spins. The TI associated with tissue can then be expressed as a spatial average of the TI
of capillary blood and the TI of the extravascular space:
I
Ni
_=
Ni + Ne Ti
TI
where
+
(Eq 7.1)
I
Ne
Ni + Ne Te
Ni the number of spins in the capillary space of a given volume
Ne the number of spins in the extravascular space in a given volume
TI is the global TI associated with the tissue
Te is the TI of the extravascular space
Ti is the TI of the intravascular space
Given that the hydrogen spin density for blood and the extravascular are approximately the same,
for a given volume of tissue we can say that
Ni
Ni+Ne
=_V1_
Vi+Ve
regional blood volume (RBV)
equation 7.1 can be rewritten as
1
=RBV
TI
Ti
+
(Eq. 7.2)
(I- RBV)
Te
When an intravascular contrast agent (IVCA) is introduced, the global TI of the tissue and the TI
will definitely change due to short range dipole-dipole interactions. Assuming that Te remains
unchanged, and subtracting equation 7.2 for the pre-contrast case and post-contrast case, one gets
the following equation for estimating RBV:
RBV
=
/TIPr - I/T Vlat
1/TI pre -
/TIPosti
In Schwarzbauer's and Schmiedl's studies, an IVCA such as Gd-BSA was administered and then
several TI maps were captured. By entering the appropriate values in Eq 7.3, both studies
produced results for RBV that matched literature values (RBV ~ 7%) though a fraction lower. We
54
can hypothesize that in the case of an infarcted region, perfusion would be poor thus (l/TIpre I/T Ipost) would be smaller for infarcted tissue than for healthy tissue, leading to smaller RBV
values for infarcted regions.
It is important to note that in using the fast-exchange model for blood volume studies, two
important assumptions were made
1)
that Te would not change with the introduction of an IVCA. It turns out that a
brief analysis of the numbers proves this assumption wrong and therefore the
model slightly imprecise.
2)
mathematically the model only accounts for diffusion effects and ignores the
effects of perfusion on the TI of tissue.
More sophisticated models that overcome both these errors will be presented shortly.
7.2 Exchange-diffusion Model
The main premise of the fast-exchange model used by Schwarzbauer and Schmiedl was
that the IVCA does not affect the TI of the extravascular space. A look at the numbers proves
though that in fact the contrast agent does affect the extravascular space. A study by Schmiedl's
in 1987 showed the TI of myocardial tissue to be around 500ms and the TI of blood was
measured at 88ms [Bauer, 1992 #42]. Using Equation 7.2 along with the estimation that blood
volume is around 7%, the formula yields a TI greater than 470ms, a number much larger than the
experimentally measured TI of 300ms for his study. The only way the IVCA could lower the TI
of tissue by this factor would be if it affected the extravascular space.
The exchange-diffusion mechanism is a highly detailed model presented by Bauer et al,
the mathematics of which shall not be covered in this paper. The model basically holds that the
55
IVCA relaxes intravascular spins which diffuse across the capillary wall and mix with
extravascular spins causing TI relaxation in the extravascular space. The degree of TI relaxation
in the extravascular space depends on
1)
the exchange time across the vessel wall (dependent on radius and diffusion
coefficient of capillary, and estimated to be 1-500ms)
2)
the density of vessels in the tissue (shown to be high in the myocardium relative to
other tissues)
The exchange-diffusion model while being very thorough and taking into account aspects such as
the geometry of capillaries is still limited. It only explains how an IVCA affects the TI of a tissue
via diffusion. It does not attempt to include the role of perfusion in its model. Bauer having
developed the first model, developed a secondary model in 1996 that accounted for perfusion
effects on the TI of post-contrast tissue. Kahler later used this model in his rat studies and proved
that the theory yielded perfusion and RBV values closer to real data than previous RBV studies
had.
7.3 Bauer's Secondary Model Which Include Perfusion Effects
As mentioned earlier, the relaxivity rates of arterial blood and capillary blood are not the same.
Due to metabolic processes, the relaxivity properties of capillary blood are different. If no
contrast agent has been introduced to the body, the arterial blood typically has a longer TI than
capillary blood, and therefore perfusion will increase the TI of tissue. In the case a contrast agent
is present, the TI of tissue is typically shortened due to perfusion. Perfusion effects are significant
when calculating regional blood volume. Take for instance the case of myocardial tissue in rats.
The regional blood volume for such tissue is about 0.074 ml/g and the coronary flow rate about
56
0.075 - 0.33 ml/s.g. The fraction of intracapillary blood that is refreshed by arterial blood is then
on the order of 90-500 % for rats [Bauer, 1996 #42].
In order to develop a mathematical model that accounts for perfusion, Bauer et al began with the
following set of equations to describe the tissue system. He used the two-compartment model (i.e.
compartments are arterial system, capillary system, and extravascular compartment). Assume a
non-equilibrium state over a time period dt, ,e.g. after a 180 pulse:
dnc=
F = flow in capillary
dnc = nuclear magnetic dipole moment inside capillary
dflreaxati denotes the loss due to T I relaxation
dnreiaxation + dlcap-evt + dflart-cap + dflcap-ven
di(t)reaxation
dt
dn (cap-ev
dnee = dipole exchange due to diffusion
-_I * n (t)
TC
=
arterial inflow into capillary
dnflap-en = capillary outflow to venous system
k = exchange rates spins between intracapillary to evt
dnrca,=
-k. *(Vc * mc(t)) + kevt * (V.vi *
(t))
dt
Fick's Law
m,=n/V and me,,=neNVest
dtLt)araap= F*mp("dt
volume in = volume out
dn(t)cap-ven=
-F*m,(t)
dt
The equations above account for perfusion as can be seen. By assuming diffusion is fastexchange between the capillaries and extravascular space, and stepping through some math
(which is skipped here), we get a perfusion-corrected equation for blood volume. As presented
earlier, initial fast-exchange models had claimed RBV could be calculated from the equation
below
RBVm =
/Tl - 1/Ti post
1/Tlpre i- 1/Tlost
In Bauer's perfusion-corrected model, he shows that the actual RBV can be calculated from the
measured regional blood volume, RBVm, by using:
57
RBV -RBV = P * (Ta*Tcb)
RBV
RBV*Tb
It was found using this method that the effect of tissue perfusion on the T I of the brain can be
neglected. However in the heart, the corrected RBV is 20% less than RBVm and much closer to
the values obtained with conventional methods. This error occurs in a heart at rest, in the case of
stress conditions, the error can be as much as 100% [Bauer, 1996 #39].
58
8.Anatomy of the Heart
Skeleton:
8..0 Anatomy of Normal Murine Heart
8.1 How Anatomy Differs When an Infarcted Region Exists
8.0 Anatomy of the Normal Murine Heart
1. Superior vena cava
2. Right atrium
3. Right ventricle
4. Left ventricle
5. Inferior vena cava
1
29
6. Aorta
39.
8 7. Pulmonary vein
8. Left atrium
Pulmonary artery
Aortic arch
7 10.
11. Left superior vena cava
Figure 8.1 : Gross anatomy of the mouse heart and its principal arteries and veins.
Within the body, the murine heart is tilted roughly at an angle of 30-40 degrees off the long axis
of the body. It measures on average 5-8mm with diameters spanning less than 3mm. At 2.OT it is
hard to see the micro or macrovasculature of the heart as depicted in Figure 8.1; what is
noticeable are the atria, ventricles and occasionally the papillary muscle of the ventricle. Typical
RR intervals for murine hearts are 100-200ms (300-700 bpm).
8.1 Anatomy of a Murine Heart with Infarct
One study conducted by Gao investigated the anatomy of hearts in which myocardial infarctions
had been induced by occluding the left coronary artery (same method used in our study). Postinfarct mortality was 46%, of which, 70% died of acute heart failure or LV rupture within the first
week. Left ventricular end diastolic and end systolic dimensions and fractional shortening (FS)
were measured in these mice and after week 1, there was modest LV dilatation [Gao, 2000 #11].
59
Another study showed that ligation resulted in antero-apical infarction of the left ventricular wall,
involving approximately 40% of left ventricular circumference. Infarction also resulted in
thinning of the infarcted area [Lutgens, 1999 #19].
60
9. Electro Physiology
Skeleton:
9.0 Introduction - Why Understand the Cardiac Cycle ?
9.1 The EKG and Phases of the Cardiac Cycle
9.2 Basset equation and Personal studies on Murine Cardiac Cycle
9.3 Conclusion- Best Time to Image
9.0 Introduction
The main challenge of cardiac imaging in comparison to imaging of the brain or other organs is
that the heart is a moving target. Often times motion appears in the image as smearing in the
phase encode direction. In order to avoid such motion artifact, each k-space line must be acquired
when the heart is at the same position. This can be achieved in two ways: either all the
acquisitions can occur in one heart beat during a time in the cardiac cycle when the heart is
relatively still, or each acquisition can occur at the same point of the cardiac cycle across several
heart beats. For instance in human hearts, the stable time period in one heart beat is long enough
that a full image can be acquired. However murine heart rates can be on the order of 600
beats/minute, yielding R-R intervals as short as 150 ms; the stable periods for such intervals are
even smaller thus one might only acquire one k-space line per heart beat. A hybrid of both
methods is possible with a segmented pulse sequence.
Since one goal of this study is to find a fast sequence with which to image perfusion defects, it
would be ideal to acquire more than one k-space line per heart beat; thus we need to understand
when and how long are the nonstationary and stationary periods of the cardiac cycle.
Understanding the cardiac cycle is not only important in reducing artifacts but also for
manipulating flow effects and capturing the heart at desired phases of its cycle.
61
9.1 The EKG and Phases of the Cardiac Cycle
R
TP
P
4
Atrial
systole
4
Ventricul
ar systole
Diastole
Figure 9.1. EKG with phases shown
Figure 9.1 above describes the cardiac cycle as it relates to an EKG reading. In cardiac imaging,
acquisition occurs relative to the R wave of the EKG. By varying the time between the R wave
and trigger (start) of the sequence, one can determine at what phase in the cardiac cycle
acquisition occurs. The R wave itself indicates the onset of ventricular systole, which ends with
the T wave. Following the T wave, the heart then enters diastole. Both systole and diastole have
two important subphases known as isovolumetric contraction (IC) and isovolumetric relaxation
(IR). Isovolumetric contraction describes the time when the heart volume is constant and equal to
the end-diastolic volume; it starts immediately after the R wave. During this time ventricular
pressure increases until the mitral valve opens and blood is ejected. In contrast isovolumetric
relaxation follows the T wave and is the time when ventricular pressure decreases while volume
remains constant (volume is equal to end-systolic volume).
62
9.2 Determining the Timings of the Cardiac Cycle in Our Study
In order to estimate the timing of the cardiac cycle in C57 BL/6 mice, we took a series of images
over the cardiac cycle of two mice. For one mouse with an R-R of approximately 550ms, half of
its cardiac cycle was acquired with coronal images that were each 25ms apart. A change in the
first image of the series from the second shows that isovolumetric contraction lasts less than
50ms. The results also show that peak systole occurs approximately at 175ms (Fig 9.2). With the
second mouse, a similar procedure was repeated but for a R-R of 350ms, a time resolution of
lOms, and with axial slices of the heart. The first three images of the series seem to be identical
which may possibly suggest that the isovolumetric period for this heart lasted about 30ms or less.
Maximum ventricular contraction also seems to suggest that peak systole occurred in the mouse
at about 130ms (Fig 9.3).
63
Figure 9.2 - Images of heart taken coronally over the entire cardiac cycle for Mouse #1. Temporal
resolution is 25 ms.
64
Figure 9.3 - Images of heart taken axially over the entire cardiac cycle for Mouse #2. Temporal
resolution is 10 ms (above figure shows every other image)
The results for the two mice correspond with published literature. Studies of the murine cardiac
cycle show that peak systole is linearly related to the square root of the RR interval; this
65
relationship is expressed by the Besset equation for a particular mouse strain [Berul, 1996 #59].
For C57 BL/6 mice, the Besset equation is as follows
QT = (25 Ims) * (RR in seconds)"2
(Eq 9.1)
For our first mouse with an RR of 550ms, peak systole should have occurred in theory around
180ms, which it did. In the second mouse, peak systole should have occurred at about 150ms
which is relatively close to the estimated 130ms. Similar findings are reported in other murine
studies such as those done by Weiss in which he imaged a murine cardiac cycle with a lOims time
resolution [Weiss, 2000 #25].
9.3 Conclusion & Discussion- Best Time to Image
Some studies have reported the isovolumetric states as being the best to image in since heart
motion is minimal [Pettigrew, 1999 #31]. With the periods lasting about 5Oms in humans, there is
sufficient time to acquire data in these subphases, however it is uncertain whether the same can
be said for murine hearts. Other studies have suggested that the heart is relatively stable during
diastole and is best imaged then. The problem with imaging in diastole is that this phase suffers
from beat to beat variations, however errors can be overcome by avoiding acquisitions close to
the end of diastole (i.e long before the next R wave).
In previously published articles on murine cardiac imaging, acquisition occurred either
immediately following the R wave (in IC) or alternatively were taken during diastole. Given our
results, we surmise that for acquisitions lasting less than 30ms, imaging within the isolvolumetric
contraction subphase or diastole is possible; for acquistions times longer than 30ms (e.g. large
RARE factor), imaging within diastole is best. Note however that if the RR is short (~ 100ms),
diastole lasts only 30ms as well. As was mentioned earlier, decisions on when it is best to image
are not only governed by avoidance of motion artifact, but by flow effects or decisions to image a
66
particular phase of the cardiac cycle (for instance we can image in ventricular systole to view the
ventricular wall at its thickest).
67
10. Experimental Procedures
Skeleton
10.0 Procedures for Creating Infarcts
10.1 Procedures for Imaging Mice
10.2 Procedures for TTC Staining
10.0 Procedures for Creating tnfarcts within Heart
Infarcts were created by ligating the left coronary artery. The mice were then allowed to rest for 1
day - 1 week before imaging; within a week's period about half the operated mice typically died.
10.1 Procedures for Imaging Mice
In this study only C57 BL/6 mice were used because of their popularity. Setup involved the
following protocol:
1) Mice were anesthetized with chloral hydrate before a dose of Gd-BSA was injected into their
jugular vein (attempts to inject into the tail vein were unsuccessful). Gd-BSA was 80mM with
DTPA to albumin ratio being 37:1 (agent was provided by Epix Medical). The injected dose was
0.1 mM/kg (0.3 ml of 8mM diluted BSA solution). A few minutes after the injection the mice
would awake.
2) The mice were then anesthetized with 1.5 % of isoflorane at a flow rate between 1-5.
3) Once asleep, they were transferred onto the surface coil and a nose cone placed on them.
Isoflorane = 1% were fed to the nose cone.
4) The two front paws of the mouse and the hind left paw were attached to the ECG plates with
tape and ultrasound gel. It was important that we made sure the heart (located roughly below the
armpits) was centered over the surface coil.
68
5) The ECG signal was then checked to verify it was clean and the threshold adjusted to have
proper triggering. Once this was done, the surface coil with mouse was placed in the magnet and
MR parameters were setup as needed. Note that imaging normally occurred within 5 hours of
injecting the Gd-BSA (not a problem since Gd-BSA is reported to stay intravascular for 24
hours).
6) The mice were imaged with a RARE IR sequence with RARE = 2, number of averages = 2, TR
= 1500ms, and TI = 300ms (to null infarcted tissue). FOV was set up as 3.84 x 1.92 mm with a
matrix size of 128 x 64 , thus giving us a spatial resolution of 300 microns. Note that the phase
encode direction is setup to match the smaller dimension of the matrix (64). The total acquisition
time of an image was approximately 1.5-2 minutes. Slice thickness was set to Imm. Trigger delay
was 1 ms and the RR interval typically ranged between 150-300 ms.
Figure 10.1 - Setup of Mouse on the Surface Coil (digital photo)
Variations That Failed:
Among some of the experimental methods tried that failed were injections into the tail-vein.
Though probably not impossible they proved to be difficult and additionally made it hard to
69
predict how much of the contrast agent got into the mouse. Injecting into the jugular vein posed
little trouble in contrast.
Attempts were also made to double-trigger the pulse sequence in order to acquire images at a
predictable points in the cardiac cycle. The first trigger would denote the time when the inversion
pulse starts and the second trigger would denote the point at which acquisition occurred. To
appropriately place the two triggers relative to the
Q waves
required some simple calculations
based on the duration of the RR interval. We found double-triggering not to work as well as
anticipated on mice with infarcts because often times their ECGs was unsteady and abnormal. A
double-triggered sequence may work well given a more robust ECG system.
10.2 Procedures for TTC-Staining
Each mouse heart was excised, sliced into Imm slices, and placed in a solution of 1 % TTC for
20-30 minutes. Photos were then taken with the use of a microscope and digital camera. Regions
which appeared white in color indicated areas of dead tissue cells, i.e. infarcted areas, while red
areas corresponded with living tissue.
70
Figure 1u.2 - I'oto o EKi setup
71
11. Gadolinium BSA Dosages
Skeleton of Write up
11.0 Introduction
11.1 Background
11.2 TI Data on Gd-BSA Doses
11.3 Infarct Detection With Different Gd-BSA Doses
11.0 Introduction
This section discusses the effect of the dosage strength of Gd-BSA on the detection of ischemic
regions. While a quantitative analysis of blood volume is not the objective of this thesis study, a
better understanding of the numbers can help us 1) estimate a dose level that will enable us to
detect perfusion defects and 2) tell us at what MR parameters to image the myocardium in order
to get optimal qualitative results for detecting ischemic regions.
11.1 Background
A study done by Kuwatsuru et al on rats investigated the relationship between various
concentrations of Gd-BSA on estimates of plasma volume [Kuwatsuru, #40]. The relationship
between plasma volume and blood volume is linear. Plasma volume, PV, is expressed as PV =
BV(1-Hct) where BV is blood volume and Het is the fractional hematocrit for a particular animal.
Thus most of the relations drawn between plasma volume and the dosage levels of Gd-BSA can
be extended to understanding the relationship between blood volume and concentration of Gd-
BSA.
In his study, Kuwatsuru injected a rat with sequentially increased doses of Gd-BSA ranging from
0.005-0.05mmol/kg. Using a spin-echo sequence, the liver and IVC (inferior vena cavae) of all
the animals were studied for corresponding changes in the signal intensity.
72
Increased doses of Gd-BSA caused the signal intensity to increase from the non-enhanced case in
both the IVC and liver. TI weighted contrast agents shorten both the TI and T2 of the sample
being imaged; however contrast agents are termed TI weighted because the effect on TI as a
percentage is greater. A look at the Bloch equation for a spin echo sequence demonstrates, that
for a given TR, a shorter TI translates to a higher signal intensity.
SI= M * e -
*e
(Eq l1.1)
-
In Kuwatsuru's study the relationship between Gd-BSA dosage and SI was seemingly linear.
Theory has shown that the effects of a TI contrast agent can be partially expressed by the
relaxivity equation shown below.
[Gd-BSA] = l/R (1/Tlenh
- I/
Inon-enh)
(Eq 11.2)
where R is termed the relaxivity factor. Each contrast agent has a particular R associated with it at
a given field strength. If the concentration of Gd-BSA increases, then 1 /TI eh increases linearly as
well, and by the relaxivity equation (Eq 11.2), we can postulate that the SI should vary
exponentially with concentration of Gd-BSA; in short, signal intensities should not be linearly
proportional to the concentration of Gd-BSA. However experimentally, Kuwatsuru's study as
well as others have shown that at low doses, less than 0. 1mmol/kg in a 2.OT field, signal intensity
vs Gd concentration is near-linear [Kuwatsuru, 1993 #40]. These studies have also shown that
with Gd-BSA, the signal intensity change begins to saturate at doses higher than 0.05 mmol Gd-
BSA/kg.
73
Saturation of the signal in a tissue is detrimental to quantitative blood volume analysis since
blood volume is calculated according to TI. Kuwatsuru's study showed that doses of Gd-BSA
higher than 0.05 mmol Gd/kg, led to higher values of plasma/blood volume which deviated from
the actual blood volume as confinned by radionuclide techniques. Since in our study the goal is to
qualitatively spot ischemic regions, saturating the signal is not as big an issue. Even if the signal
in the non-ischemic region saturates somewhat, these areas should be distinguishable from
ischemic areas. The only down side to saturating the signal is that areas that suffer only mild
perfusion abnormalities may be hard to detect. We thus postulate that doses higher than 0.05
mmol Gd/kg should still allow us to qualitatively detect areas of gross perfusion defects (such as
infarcted regions).
11.2 Experimental Results of Varying Gd-BSA Dose
Kuwatsuru's study showed that signal did not saturate in tissue at doses between 0.005 - 0.05
mmol/kg. We used this range of concentrations as our starting point and aimed to find out the TI
effect on tissue of this range and furthermore if it would be possible to detect infarcts at these
concentrations.
11.3 T1 Effect of BSA Concentration:
The amount X to be injected into a C57 BL/6 mouse was calculated following Equation 11.3
below. Note that the weight of the mice was set at 25g and the concentration of the Gd-BSA was
80mM with a molecular weight of 115 kDa and 37 Gadolinium molecules bound to each albumin
molecule.
(X in ml)(80mM/1000ml) = 0.025 kg*(BSA dose between 0.01-0.04mM/kg)
74
(Eq
11.3)
For a concentration of 0.01mMIkg and 0.04mM/kg, the respective amounts of 80mM Gd-BSA to
be injected are 0.003 ml and 0.01 ml. To make procedures easier, we diluted the 80mM Gd-BSA
by a factor of 1:10 with saline, and injected 0.03ml and 0. Iml of the diluted chemical into the
mice.
TI measurements taken with a normal saturation recovery sequence at a 2.0 T magnet showed the
following results
Gd-BSA
Measured Ti of the
Concentration
myocardium (ms)
mM/kg
0
1100-1300
0.01
1000
0.04
625
0.1
500-550
0 19
400
.19
400
Table 11.1 - Gd-BSA Concentration and associated TI of the Myocardium
The above measures are estimates of the TI of myocardium taken with a saturation recovery
sequence immediately after the mice were sacrificed (motion artifact interfered with getting good
TI measurements in-vivo). Fig 11.1 shows the same results as Table 11.1 but on a graph
comparing Gd-BSA concentration against 1/Ti. According to Eq 11.2's relaxivity equation, the
relationship between concentration of Gd-BSA and 1/Ti should be linear in theory; whether this
is the case experimentally is hard to ascertain given the limited data.
75
Gd-BSA concentration vs ITI
..
0.003
0.0025
0.002-0.0015
0.001
0.0005
0
0
0.2
0.15
0.1
0.05
Gd-BSA concentration (mmollkg)
Figure 11.1 - Gd-BSA concentration vs 1/T1
11.4 Infarct Detection at High Gd-BSA Concentrations
From experimental trials and from knowing the TI of myocardium associatedwith various
concentrations of Gd-BSA, we were able to ascertain the MR parameters necessary to null the
perfusion-defective myocardium. Assuming infarcted regions receive little blood and thus little
contrast agent, their TI should remain approximately the same as unenhanced myocardium (Ti
=
1100-1300ms). The inversion time required to null infarcted tissue is approximately 300-350ms.
Table 11.2 shows inversion times that the null healthy myocardium for other doses of Gd-BSA.
Concentration BSA mM/kg
Ti Myocardium (ms)
Null point of myocardium: TI for TR=1500ms
0
1100-1300
300-350
0.04
625
200
0.1
500-550
180-200
0.19
300-400
----
Table 11.2 - Inversion Times for Nulling Healthy Myocardium at Different Concentration of Gd-BSA
76
Testing the three doses 0.04mM/kg, 0.01mM/kg and 0. l9mM/kg on an infarcted mouse heart, we
were able to see which of these three doses enabled us to detect gross perfusion defects best.
Below are the images of three infarcted hearts, each with a different dose of Gd-BSA, acquired
with an inversion recovery sequence. The two right hand images are the ones taken at doses 0.1
mM/kg and 0.19 mM/kg, and show SI inhomogenities better than the image taken at 0.04 mM/kg;
it was almost impossible to discern SI inhomogenities in the 0.04 mM/kg image.
Figure 11.3: Infarcted Hearts with
3 Different Doses of Gd-BSA. Top
Left: 0.04mM/kg; Top Right: 0.19
mM/kg (same slice as top-left
image); Bottom right: 0.1 mM/kg
(different heart as other two
images).
We thus concluded that out of the doses we tested, a dose of 0.1 mM/kg is the minimum dose
required for detecting gross perfusion defects in murine myocardium; we administered this dose
to all the experimental mice in our study.
77
12. IR TurboFLASH on Murine Heart & Phantom
Skeleton:
12.0 Introduction
12.1 Explanation
12.2 Studies on a
12.3 Studies on a
12.4 Conclusion-
and goals of turboFLASH study
of the sequence and pulse program. Including brief theory.
phantom and Results.
mouse at 2.OT.
sunuary.
12.0 Introduction
A perusal of previous literature reveals turboFLASH was often implemented in murine cardiac
imaging experiments. In view of the sequence's popularity and its rapid scan times, we decided to
evaluate its efficiency for perfusion imaging.
In using an IR turboFLASH sequence, three goals were at the forefront of the study:
1) to determine the optimal parameters for the sequence, where "optimal" refers to the
parameters which yield the best SNR within a unit time. Parameters under test were
segmentation, flip angle a, and number of averages.
2) to determine whether imaging at the optimal parameters found in part 1) would give us
sufficient SNR when imaging the murine heart in a reasonable imaging time.
3) to evaluate the optimized performances of IR turboFLASH and RARE in
differentiating infarcted regions (covered in another chapter of the write up).
12.1 Brief Theory
A brief summary of the important aspects of turboFLASH follows. For a detailed explanation of
turboFLASH, please refer to the section of the writeup on Cardiac Pulse-sequences.
Given that the T 1 of a sample and the TR in an experiment are specified, it is possible to estimate
the optimal flip angle for a turboFLASH sequence. Theory and previous studies have shown that
the optimal flip angle is governed by the following equation [Reeder, 2000 #44]:
a = cos (e
(Eq 12.1)
-TI)
78
Furthermore the relative signal can be estimated as
- TR I TI
SGE =
M= e -TET2
'Eq 12.2)
*
IT1
-+e-TR
An inversion recovery turboFLASH sequence is a small variation in the normal turboFLASH
sequence in that it is preceeded by a 180
0
inversion pulse. Figure 12.1 shows a diagram of the
pulse sequence used in our experiment. This particular example uses a nonselective inverting
pulse.
Figure 12.1 - Pulse sequence for a IR turboFLASH sequence.
79
12.2 Modeling the Sequence Parameters on a Phantom
Variable and Fixed Parameters
We decided to model the sequence on a phantom of Gd-DTPA in saline before going to a real
heart. The TI and T2 of this phantom were measured to be 300 ms and 100 ms respectively at a
2.OT field strength. The objective of the phantom study was to satisfy goal #1 listed above, i.e.
answer the following question: what parameters will give us the optimum SNR per scan time
(SGRE/scan time as defined in Eq 12.2).
The parameters that were varied were the number of averages and the numnber of segments per
TR. The parameters that remained constant in the study were the TI, TE, and TR of the inversion
recovery sequence. Note there is no need to specify the segment repetition time TR, (time
between each ax pulse), because it is always maximized according to the number of segments we
decide to have (an example is provided later). Likewise the optimal cc flip angle is maximized in
relation to the number of segments as described by Eq. 12.1.
Modeling the Physiologic Case
Since we are modeling a segmented IR turboFLASH sequence for subsequent use on a murine
heart, we need to appropriately alter our phantom study to mimic the real life case. In a cardiac
experiment the TI of the myocardium is about 10OOms at a 2.OT field. A TR of 1500 ms has been
found to work reasonably and the echo time, TE, is usually about 4-5ms. Assuming that imaging
will take place in diastole, we have about lOOms of stable time during which multiple signal
acquisitions can occur. Therefore if for example, we have a segmentation of 2, each segment time
length can be maximized to 50 ms. To mimic these constraints in the phantom, the parameters for
our phantom study were set as follows:
TR= T
phantom *
(TR
hcat,
/ TI
he)
300ms * (1500/1000)
90
= 450ms
"
TE does not matter since it is held constant in the study and won't
affect relative comparisons of SG..
"
TR, = (TR, of heart / Ti
=
a)
* TI
phntom
(100ms/# segments)/IOOOms * 300ms
*
a flip angle is maximized according to Eq. 12.1
*
TI= 0 (which is the same as making the IR turboFLASH sequence a regular
turboFLASH sequence).
Theoretical Results
A simulation of the parameters on Matlab yielded the following data (where SlrIs is the relative
SI, which is equal to the absolute SI normalized by the SI for an unsegmented turboFLASH
sequence):
# avgs
#
x (degrees)
SNRw
SNRr(scan time)
segments
16
16
10
100.2
100.2
8
8
14
102.1
102.1
4
4
19
100.2
100.2
2
2
26
100.1
100.1
1
1
90
100.0
100
1
16
10
25.0104
400
1
8
14
36.0
288
1
4
19
50.0
200
1
2
26
70.7
141.4
Table 12.1. SNR simulations on Matlab when parameters of II turboFLASH varied
81
In the first half of the table above the parameters were varied such that acquisition time
was the same. In the second half of the table the number of averages were kept the same.
Though average = 1 and segmentation = 16 seems to yield the best SNR per unit time, the
overall SNR is one fourth of the base case, perhaps too low to see a good image. If we
compare scans with the same scan times, then average = 8 and segmentation = 8 seems to
give us the best results. The numbers generated in our mathematical model were
compared against experimental data from our phantom study.
Scan #
# avgs
#
X (degres)
SNRm
SNRm/(time of
unsegmented case)
segments
1
16
16
10
38.9
38.9
2
8
8
14
62.9
62.9
3
4
4
19
73.4
73.4
4
2
2
26
88.2
88.2
5
1
1
90
100
100
11
1
16
10
13.5
216
12
1
8
14
22.1
176.8
13
1
4
19
40.4
161.6
14
1
2
26
67.3
134.6
Table 12.2 SNR measurements on phantom when parameters of IR turboFLASH varied
Scans 1-5 in Table 12.2 compare the SNR of experiments which have the same total scan time.
With averaging, the optimal SNR generated occurs when no segmentation is used (scan 5). Scans
11-14 compare the SNR of experiments which do not use averaging. If we look for which case
yields the best SNR for scan time, then a segmentation of 16 with works best. One can note that
the SNR for segmentation = 16 is on the order of nine to ten times less than the unsegmented case
82
(even lower than what was predicted our Matlab simulations). The big question about using a
segmentation of 16 without averaging is whether there will be enough SNR when imaging a heart
at 1mm slice thickness and resolution 200-300 micron.
12.3 Studies on a Mouse Heart at 2.OT field strength
Figure 12.2- Images of murine heart taken with IR turboFLASH.
The first row of the images in Fig 12.2 shows the results of imaging the heart with segmentation
-1, 2, 4, and 8, with 1 average. The case with segmentation= 16 was omitted since the SNR was
already low for segmentation =8 and would only have been lower with segmentation = 16. From
the images in the first row with 1 average, segmentation = 1 gave the only decent SNR results.
We then compared this with an image taken at segmentation =2 with average=2. The image
provided too low an SNR and further segmentation would only have worsened this. We thus
concluded that IR TurboFLASH with segmentation = 1 (i.e. an IR sequence with gradient echo) is
best for our imaging purposes.
83
12.4 Conclusion
By simulating the segmented IR turboFLASH sequence mathematically and furthermore testing it
on a phantom, we were able to conclude what the optimal segmentation was segmentation = 16
with I average. However when we tried the sequence on an ex-vivo heart, we concluded that we
did not get sufficient SNR on our 2.OT magnet when using segmentation. The best case therefore
is an unsegmented turboFLASH in murine hearts, i.e. an inversion recovery sequence with
gradient readout. Additionally comparing the base case of an unsegmented turboFLASH to a spin
echo showed that a spin-echo offered better SNR, thus we abandoned any further efforts to
evaluate turboFLASH.
84
13. Analysis of IR RARE sequence on Murine Heart &
Phantom:
Skeleton:
13.0 Introduction and goals of RARE study
13.1 Explanation of the sequence and pulse program. Including brief theory.
13.2 Studies on a phantom and Results. Satisfied goal #1.
13.3 Studies on a mouse at 2.OT. Satisfied goal #2
13.4 Conclusion- summary.
13.0 Introduction
In using a IR RARE sequence, three goals were at the forefront of the study:
1) to determine the optimal parameters for the sequence on a phantom, where "optimal"
refers to the parameters which yield the best SNR within a unit time. Parameters under
test were the number of echoes and number of averages.
2) to determine whether imaging at the optimal parameters found in part 1) would
provide decent images of the murine heart.
3) to evaluate the optimized versions of IR turboFLASH and RARE in differentiating
infarcted regions (covered in another chapter of the write up).
13.1 Brief Theory
A brief summary of the important aspects of RARE follows. For a detailed explanation of RARE,
please refer to the section of the writeup on Cardiac Pulse-sequences.
Compared with conventional spin echo imaging, the most important feature of RARE imaging is
that several phase-encoding lines are collected with each excitation pulse. The IR RARE pulse
sequence evaluated in our pulse sequence is shown below in Fig 13.1. As illustrated in the figure,
the RF pulse scheme includes a 180 degree RF pulse and then a 90 degree pulse, followed by
several refocusing RF pulses (the number of echoes is referred to as the RARE factor). Compared
to turboFLASH, RARE by virtue of being a spin echo is effected by T2 decay, whereas
turboFLASH uses a gradient echo and is thus susceptible to T2*.
85
Figure 13.1 - Pulse sequence of a RARE IR sequence.
13.2 Modeling the Sequence Parameters on a Phantom
Variable and Fixed Parameters
We decided to model the sequence on a phantom of Gd-DTPA in saline before going to a real
heart. The parameters that were varied were the number of averages and the number spin echoes.
The parameters that remained constant in the study were the TI and TR of the inversion recovery
sequence.
Modeling the Physiologic Case
Since we were modeling a IR RARE sequence for subsequent use on a murine heart, we needed
to appropriately alter our phantom study to mimic the real life case. In a cardiac experiment the
TI of the myocardium is about 1000 ms at a 2.OT field and the T2 of muscle is about 25-30ms.
86
When imaging a mouse heart with IR RARE, a TR of 1500ms has been found to work reasonably
and the echo time, TE, can be reduced to about 4.1 ins. For turboFLASH sequences all the
parameters were dependent on the TI of the sample under study; for RARE, the efficiency of the
parameters (i.e. RARE factor) depend on the T2 of the sample and therefore the echo time, TE,
matters.
*
TR= Ti
TE=
*
T
2
phantom *
(TR heart / TI
phantom *
4ms/28ms = 14ms
heart)
300ms
*
(1500/1000) = 450ms
TI = 0 (which is the same as making the IR RARE sequence a normal RARE sequence).
Experimental Results on Phantom
Figure 13.2 shows the images taken of the phantom with various RARE factors and averages.
The first row displays images with RARE = 1, 2, 4, and 8 taken with 1 average. One can note that
with RARE = 4 and RARE = 8, the signal is smeared in the vertical direction the phase encode
direction due to excess T2 decay. From a qualitative standpoint it already looks like RARE = 2 is
the maximum number of echoes we can tolerate. The second row of images shows RARE = 2, 4,
and 8 taken with 2 averages this time. Again RARE factors 4 and 8 show excessive smearing.
The best candidate therefore is either RARE = 1 with average = 1, RARE = 2 with average =2, or
RARE = 2 with average = 1. The fmial case is the more preferred because it has half the
acquisition time of the other two cases and still yields decent SNR.
87
Fig 13.2. IR RARE images of phantom. First row from Left to Right shows 1 average: segmentation
1, 2,4,8. Second Row from Left to Right shows 2 averages: segmentation = 2,4, and 8.
Table 13.1 lists the SNR,
=
measurements relative to the base case (RARE = 1, average = 1). We
ignore all rows with RARE factors equal to 4 or greater because of the error in smearing/banding
observed qualitatively. From the remaining cases the SNR can be ranked from best to worst as
rare=2 avg=2, rare = 1 avg=1, and then rare=2 avg=1. If ranked by SNR per unit time, then the
best to worst cases are ranked as rare=2 avg=1, rare-=2 avg=2, and rare=1 avg=l. Deciding which
case provides the best SNR per unit time was concluded by testing these parameters on the
murine heart.
SNRJ(time of unsegmented
cas")
# avgs
RARE factor
SNRno
1
1
100
1
2
91.1
182.2
1
4
111.3
445.2
1
8
71.8
574.4
2
2
154.1
154.1
2
4
143.4
286.8
2
8
81.0
324.0
100
Table 13.1 Values Recorded from RARE IR study on phantom
98
13.3 Studies on a Mouse Heart
Figure 13.3 shows the images taken of the murine heart with various RARE factors and averages.
The first row displays images of RARE = 2, 4, and 8 with 1 average and the second row displays
the same RARE factors with 2 averages, and the third row with 3 averages. Note that images
within one column have the same acquisition time.
Though hard to note in these figures, RARE factor 4 shows some smearing/banding as predicted
from our phantom model. Of the cases with RARE factor 1 and 2, the image taken with RARE
=
2 avg=1 seems to provide the most decent images for the given acquisition time. We therefore
conclude RARE = 2 with 1 average is the optimal parameter for the purposes of imaging murine
hearts.
89
Figure 13.3 Murine Heart studied with RARE IR sequence. Top row is 1 average with RARE factors = 1, 2, 4, 8
(left to right). Second row is 2 averages with RARE factor = 2,4,8. Third row is 4 averages with RARE factors =
4,8.
13.4 Conclusion
By simulating the IR RARE sequence on a phantom, we were able to conclude that the optimal
RARE factor would be RARE =2 with 1 average for the sequence. This finding was confirmed
when we tried the various parameters on a murine heart. In both the phantom and heart study,
RARE factors of 4 and greater suffered from excessive T2 decay. The next step is to see whether
the optimized IR RARE sequence or optimized IR turboFLASH sequence works better in
differentiating infarcted tissue from healthy myocardium.
90
14. MR Images of Infarcted Hearts
Skeleton
14.0 MR Methods Used for each Mouse
14.1 MRI Results vs. TTC Staining
14.2 Discussion
14.0 Methods
MI-M3:
We attempted to differentiate perfusion defects in a total of 7 mice, all of whose left coronary
arteries had been ligated to create an infarct. The first three mice (denoted as M1, M2, M3) were
imaged a week following ligation and had a concentration of 0.19 mM/kg Gd-BSA administered
before MR imaging. Attempts were made to null out the infarcted region using an inversion time
of 0.3 seconds, however due to a thinned ventricular wall in the insulted sections, it was hard to
determine at 300 micron whether we were successful. Nulling out healthy myocardium seemed to
show more promising results. Inhomogenities in signal intensity were distinguishable in the
myocardium and thus 5-6 axial slices of 1-1.25 mm were captured with healthy myocardium
nulled.
M4:
To overcome the problem posed by a thin wall and test whether the abnonnal region could be
nulled, we imaged in the coronal plane using an inversion time of 0.3 seconds. Distinct contrast
was shown in different regions of the myocardium. Also the original dose of 0.19 mM/kg was
dropped to 0.1 mM/kg to see if it was possible to image with lower doses and reduce the risk of
encountering saturation effects.
M5:
The mouse died during imaging.
91
M6-M7:
Mouse M6 and mouse M7 were imaged 4 days following ligation. We tried to null the infarcted
region as was done with M4, but an inversion time of 0.3 seconds did not show contrast.
Therefore the next best option was to null the healthy myocardium. For a dose of 0.1 mM/kg, the
inversion time used to null the myocardium was 0.18-0.2 seconds. We took 5-6 axial shots of 11.5mm thickness and 200 micron resolution. Additionally a test with a plain GEFI showed the
infarcted region to be brighter than the healthy myocardium meaning, that the TI of the infarcted
region was shorter than the TI of the myocardium.
A summary of the methods used to image mice MI-M7 are shown in Table 14.1. The pulse
sequence used is listed too; note that both gradient echo IR and RARE IR were used on all mice
but final images were captured with the optimal one.
0.19
Myocardium
300
Slice
thickness
(mm)
1
Myocardium
300
1
7
0.04 &
0.19
0.19
Myocardium
300
1.2
5
0.1
Infarcted
300
1.5
Pulse
sequence
used
RARE IR
RARE = 1
RARE IR
RARE = 1
RARE IR
RARE = 1
GEFIIR
MI
Days
after
Ligation
7
M2
7
M3
M4
Mouse
M5
Region
nulled
Gd-BSA
(mM/kg)
-
____
Resolution
(micron)
RARE = 2
too little SNR
RARE = 2
too little SNR
RARE = 2
was possible
----
-
M6
4
0.1
Myocardium
200
1.0
GEFI IR
M7
4
0.1
Myocardium
200
1.2
GEFI IR
M8
M9
M10
Ml1
0
1
3
0.1
0.1
0.1
0.1
3
Comments
GEFI IR
1.2
200
Myocardium
GEFI IR
1.2
200
Myocardium
GEFI IR
1.2
200
Myocardium
GEFI IR
1.2
200
Myocardium
1.
M1-Mi
Testing
for
Conditions
of
Summary
14.1
Table
92
RAREIR
had low SNR
RAREIR
had low SNR
14.1 Results: MR Images vs TTC stained hearts
Ml-M3:
TTC stains for M1-M3, showed that all the hearts had abnormal tissue. In the MR images of Ml
and M3 this was hard to detect (shown in Fig 14.1), however M2 did show some SI
inhomogenities in one slice that related to TTC staining (Fig 14.2). Two possible explanations for
why MRI could not detect the insulted regions are 1) the ventricular walls had thinned due to
infarction such that it was difficult to see SI inhomogenities and 2) the dose of Gd-BSA may have
been large enough to cause saturation effects.
M2
M1
M3
Figure 14.1 MR images for MI, M2, and M3. All show almost no SI inhomogenties that could suggest perfusion
defects in the heart.
93
Suspecting that the dose may have been too high, two days after the first set of MR images for
M2, we re-dosed the mouse at 0.04 mM/kg Gd-BSA. Previous studies have shown no saturation
effects with this dose. A comparison of the same axial slice in M2 at 0.19 mM/kg and 0.04
mM/kg is shown below. At the higher dose we clearly see some evidence of a perfusion defect; at
the lower dose the differentiation is almost unnoticeable.
MR Image of M2 slice compared with TTC
No
M2- 0.04 nMikg
-0.19
mIg
TTC Stain
Figure 14.2 MR images for the same slice of M2 at two different BSA concentrations. Bottom image is TTC stain
of the corresponding slice.
M4:
The coronal slice of M4 shown in Fig 14.3 below indicates some correlation between the
infarcted region in the MR image (nulled region) and the white infarcted area denoted in the TTC
stain. The MR images show the defective region as being larger than the actual infarcted region.
94
It is possible that the MR image includes the areas at risk (the ischemic area) as well as the
infarcted area. It is also possible that due to the difficulty in getting histology on coronal slices,
the TTC stained slice does not correspond fully with the slice of the MR image. Atleast the MR
image seemed to indicate that a dose of 0.1 mM/kg could detect some degree of perfusion defect
in the myocardium.
An additional finding with M4 was that MR images taken at inversion times other than the null
point, did not show any severely darkened areas in gradient echo sequences. This piece of
information was useful in ruling out the possibility that susceptibility effects may have been
responsible for nulling the infarcted regions.
Mouse 4: Infaret Nulled
Figure 14.3 MR image and corresponding TTC stain for M4
M6-M11:
Using the same dose as was used for M4, M6 -Ml 1 were imaged with axial slice of 200 micron
resolution. The results from MR and TTC are shown in Figures 14.4-8. Because of the higher
95
resolution and because the images were taken soon after ligation, the inhomogenities in the
myocardium are clearer than what was shown for M l-M3. In M6 the second slice from the apex
is particularly noteworthy because the MR image matches histology closely. The MR images
seem to indicate the insulted area is larger than what is shown by TTC staining; again this could
be because the MR images include ischemic regions.
Mouse 6: Healthy Myocardium Nulled
Figure 14.4 MR image and corresponding TTC stain for M6
96
Mouse 7: IR gradient echo with healthy Myocardium Mulled
bFe
Figure 14.5 MR image and corresponding TTC stain for M7
97
Mouse 8 - Heart without Infarct
Figure 14.6 MR image and corresponding TTC stain for M8- normal heart (i.e. no infarcted tissue)
Mouse 9
98
Mouse 10
Figure 14.8 MR image and corresponding TTC stain for M10
Mouse 11
LFigure 14.9 MR image and corresponding TTC stain for M 1I (Evan's Blue stain used here to show areas of
reperfusion)
99
14.2 Discussion
MRI vs TTC:
MR imaging of the first three mice Ml -M3 proved to be unsuccessful due to either 1) excessive
wall thinning of the infarcted region or 2) the dose of contrast agent being too high. By halving
the dose and imaging sooner after ligation (4-5 days), MR results taken as a coronal slice from
M4 seemed to yield promising results when compared with TTC staining. M6 and M7 were
imaged at the same dose used for M4 but with axial slices of resolution 200 micron (higher
resolution than used previously). A look at Fig 14.4 -14.9 suggests an overlap in the areas
marked as injured tissue by TTC and MRI. In some instances, such as Fig 14.3 and the last slice
in Fig 14.4, the region shown by MRI is larger than that shown by TTC. This could be due to bad
mapping of TTC slices to MR slices or the fact that MR imaging and TTC staining measure two
different parameters. TTC staining differentiates between necrotic and healthy tissue. MR
imaging with Gd-BSA differentiates between perfused and non-perfused areas. Therefore
ischemic regions targeted by MRI may show both the infarcted region as well as the area at risk
while TTC only marks the infarcted region.
Pulse Sequence:
Though our studies between RARE IR and GEF IR showed that RARE IR with rare factor 2 was
the optimal sequence to use, we found GEFI IR to be best in detecting infarcted regions at 2.OT.
The main constraint in using RARE IR was the low SNR. Because it has a TE of 7-8ms, twice
that of GEFI IR, RARE IR suffers greater T2 decay which renders the image quality low. It is
possible that at higher magnetic fields or with shorter TE's, a RARE IR sequence could be used
successfully.
In developing the MR parameters we also decided that nulling viable myocardium was a better
option than nulling infarcted regions. Nulling viable myocardiurn could be done reliably with an
inversion time of 180-200ms at a dose of 0.1 mM/kg; the same reproducibility could not be
100
achieved with the infarcted region. Infarcted regions can suffer reduced perfusion due to
obstruction of the microvasculature but opposing this, capillary leak may occur in necrotic areas
and increase the amount of contrast agent in the extravascular space. It is hard to predict what the
concentration of Gd-BSA in the ischemic region will be, thus it is easier to null healthy
myocardium.
101
15. DISCUSSION
The goal of this study was to be able to detect perfusion defects in murine myocardium with MRI.
Additionally we focused on evaluating the effectiveness of various pulse sequences and
parameters in imaging infarcted tissue in an attempt to define a fast sequence that would detect
perfusion defects at a 2.OT field. The two principle sequences compared were inversion recovery
RARE and inversion recovery turboFLASH (or GEFI IR).
Developing a Method
By simulating the segmented IR turboFLASH sequence mathematically and furthermore testing it
on a phantom, we were able to conclude that the most efficient segmentation was segmentation =
16 with 1 average. However when we tried the sequence on a heart, we concluded that we did not
get sufficient SNR on our 2.OT magnet when using segmentation. The best case for turboFLASH
therefore was an unsegmented turboFLASH in murine hearts, i.e. an inversion recovery sequence
with gradient echo readout. Additionally comparing the base case of an unsegmented
turboFLASH to a spin echo showed that a spin-echo offered better SNR, thus we abandoned any
further efforts to evaluate turboFLASH.
When testing the IR RARE sequence on a phantom, we were able to conclude that the optimal
RARE factor would be RARE = 2 with 1 average for the sequence. This finding was confirmed
when we tried the various parameters on a murine heart. In both the phantom and heart study,
RARE factors of 4 and greater suffered from excessive T2 decay.
Though our studies between RARE IR and GEFI IR showed that RARE IR with rare factor 2 was
the optimal sequence to use, we found GEFI IR to be best in detecting infarcted regions at 2.OT.
The main constraint in using RARE IR was the low SNR. Because it has a TE of 7-8ms, twice
102
that of GEFI IR, this may be due to the fact that RARE IR suffers greater T2 decay which renders
the image quality low. Perhaps the reason we did not see this in our previous phantom studies was
that those particular hearts were not dosed with Gd-BSA which shortens T2 (and TI of course). It
is possible that at higher magnetic fields or with shorter TE's, a RARE IR sequence could be used
successfully.
In developing the MR parameters we also decided that nulling viable myocardium was a better
option than nulling infarcted regions. Nulling viable myocardium could be done reliably with an
inversion time of 180-200ms at a dose of 0.1 mM/kg; the same reproducibility could not be
achieved with the infarcted region. Infarcted regions can suffer reduced perfusion due to
obstruction of the microvasculature but opposing this, capillary leak may occur in necrotic areas
and increase the amount of contrast agent in the extravascular space. It is hard to predict what the
concentration of Gd-BSA in the ischemic region will be, thus it is easier to null healthy
myocardium.
We determined the best dose of Gd-BSA to administer by testing three doses: 0.04mM/kg,
0.0 lmM/kg and 0. 19mM/kg on an infarcted mouse heart. We found that doses 0.1 mM/kg and
0.19 mM/kg showed SI inhomogenities in the myocardium, whereas at a dose of 0.04 mM/kg; it
was almost impossible to discern SI inhomogenities in the 0.04 mM/kg image.
Testing Method on Murine Hearts
Of the 11 mice imaged, 4 were used to understand and refine the MR parameters which would
enable us to detect ischemic tissue (M1-M4). One mouse died (M5), and the other 5 mice (M6M 11) were imaged at the final specified MR parameters. These final parameters for a 2.OT field
were: axial slices with 1-1.25mm slice thickness, 200 pn2 in-plane resolution, trigger delay of
I ms. The sequence used was an inversion recovery sequence with gradient readout; inversion
103
time was set to null healthy myocardium (TI=180-200ms), TE = 3-4ms and the repetition time
(TR) was set to 1500ms. All mice that were imaged were then sacrificed and their hearts sliced
axially and stained with TTC. Please refer to Section 14 to view the MR images and
corresponding TTC stained slices.
Mice M6-M 11 showed areas of abnormal myocardial tissue in both MR images and TTC
staining, with the exception of M8 which was shown to have a completely healthy heart. TTC
suggests a correspondence between nonviable myocardium and brightened regions in the MR
images. The areas demarcated as abnormal by MRI occasionally appeared larger than those
shown by TTC. This could be due to bad mapping of TTC slices to MR slices or the fact that MR
imaging and TTC staining measure two different parameters. TTC staining differentiates between
necrotic and healthy tissue. MR imaging with Gd-BSA differentiates between perfused and nonperfused areas. Therefore abnormal regions targeted by MRI may show both the infarcted region
as well as the area at risk while TTC only marks the infarcted region.
Suggestions for Future Studies
*
Determine the cause for the BSA enhancement seen in the abnormal myocardium (as
observed in this study). Note that the causes may differ depending on the time after ligation
due to tissue recovery processes.
"
Imaging at higher field strengths will provide better resolution and image quality, and may
enable one to use faster imaging sequences (e.g. RARE IR with rare = 2).
"
Imaging at higher field strengths may also enable quantitative studies of blood volume, which
though not a direct measure of perfusion is nevertheless approximately related.
104
*
With more advanced ECG systems it may be possible to double gate the pulse sequence and
find whether certain phases in the cardiac cycle are more optimal for imaging perfusion
defects.
105
16. BIBLIOGRAPHY
1.
Arai A. "Magnetic resonance first-pass myocardial perfusion imaging.". Top Magn
Reson Imaging 2000 Dec;6:383-98.
2.
Sandstede JJ LC, Beer M, Harre K, Pabst T, Kenn W, Neubauer S, Hahn D. "Analysis of
first-pass and delayed contrast-enhancement patterns of dysfunctional myocardium on MR
imaging: use in the prediction of myocardial viability.". AJR Am J Roentgenol 2000 Jun;6:173740.
3.
Choi SI JC, Lim KH, Kim ST, Lim CH, Gong GY, Lim TH. "Application of breath-hold
T2-weighted, first-pass perfusion and gadolinium-enhanced T 1-weighted MR imaging for
assessment of myocardial viability in a pig model.". J Magn Reson Imaging 2000 May;5:476-80.
4.
Pereira RS WG, Prato FS, Yvorchuk K. "Clinical assessment of myocardial viability
using MRI during a constant infusion of Gd-DTPA.". MAGMA 2000 Dec;3:104-13.
5.
Bremerich J SM, Arheden H, Higgins CB, Wendland MF. "Normal and infarcted
myocardium: differentiation with cellular uptake of manganese at MR imaging in a rat model.".
Radiology 2000 Aug;2:524-30.
6.
Bauer WR NW, Bock M, Schad LR, Wacker C, Hartlep A, Ertl G. "The relationship
between the BOLD-induced T(2) and T(2)(*): a theoretical approach for the vasculature of
myocardium.". Magn Reson Med 1999 Dec;6:1004-10.
7.
Wacker CM BM, Hartlep AW, Beck G, van Kaick G, Ertl G, Bauer WR, Schad. Changes
in myocardial oxygenation and perfusion under pharmacological stress with dipyridamole:
assessment using T*2 and TI measurements. Magn Reson Med 1999 Apr;4:686-95.
8.
Gerber BL LJ, Garot J, Bluemke DA. "Magnetic resonance imaging of myocardial
infarct.". Top Magn Reson Imaging Top Magn Reson Imaging;6:372-82.
9.
Callaghan P. Principles of Nuclear Magnetic Resonance Microscopy. New York, NY:
Oxford University Press; 1993.
10.
Primer A. Medical Magnetic Resonance Imaging and Spectroscopy. Berkeley, CA:
Society of Magnetic Resonance in Medicine; 1986.
11.
Gao XM, Dart AM, Dewar E, Jennings G, Du XJ. Serial echocardiographic assessment of
left ventricular dimensions and function after myocardial infarction in mice. Cardiovasc Res
2000;45:330-8.
12.
Suehiro K, Takuma S, Cardinale C, Hozumi T, Shimizu J, Yano H, et al. Assessment of
segmental wall motion abnormalities using contrast two- dimensional echocardiography in awake
mice. Am J Physiol Heart Circ Physiol 2001;280:H1729-35.
13.
Yang Z, French BA, Gilson WD, Ross AJ, Oshinski JN, Berr SS. Cine magnetic
resonance imaging of myocardial ischemia and reperfusion in mice. Circulation 2001;103:E84-4.
106
14.
Bryant D, Becker L, Richardson J, Shelton J, Franco F, Peshock R, et al. Cardiac failure
in transgenic mice with myocardial expression of tumor necrosis factor-alpha. Circulation
1998;97:1375-81.
15.
Chacko VP, Aresta F, Chacko SM, Weiss RG. MRI/MRS assessment of in vivo murine
cardiac metabolism, morphology, and function at physiological heart rates. Am J Physiol Heart
Circ Physiol 2000;279:H2218-24.
16.
Franco F, Dubois SK, Peshock RM, Shohet RV. Magnetic resonance imaging accurately
estimates LV mass in a transgenic mouse model of cardiac hypertrophy. Am J Physiol
1998;274:H679-83.
17.
, Henson RE, Song SK, Pastorek JS, Ackerman JJ, Lorenz CH. Left ventricular torsion is
equal in mice and humans. Am J Physiol Heart Circ Physiol 2000;278:H1 117-23.
18.
Jelicks LA, Shirani J, Wittner M, Chandra M, Weiss LM, Factor SM, et al. Application of
cardiac gated magnetic resonance imaging in murine Chagas' disease. Am J Trop Med Hyg
1999;61:207-14.
19.
Rose SE, Wilson SJ, Zelaya FO, Crozier S, Doddrell DM. High resolution high field
rodent cardiac imaging with flow enhancement suppression. Magn Reson Imaging 1994;12:1183-
90.
20.
Ruff J, Wiesmann F, Hiller KH, Voll S, von Kienlin M, Bauer WR, et al. Magnetic
resonance microimaging for noninvasive quantification of myocardial function and mass in the
mouse. Magn Reson Med 1998;40:43-8.
21.
Ruff J, Wiesmann F, Lanz T, Haase A. Magnetic resonance imaging of coronary arteries
and heart valves in a living mouse: techniques and preliminary results. J Magn Reson
2000; 146:290-6.
22.
Siri FM, Jelicks LA, Leinwand LA, Gardin JM. Gated magnetic resonance imaging of
normal and hypertrophied murine hearts. Am J Physiol 1997;272:H2394-402.
23.
Slawson SE, Roman BB, Williams DS, Koretsky AP. Cardiac MRI of the normal and
hypertrophied mouse heart. Magn Reson Med 1998;39:980-7.
24.
Wiesmann F, Ruff J, Hiller KH, Rommel E, Haase A, Neubauer S. Developmental
changes of cardiac function and mass assessed with MRI in neonatal, juvenile, and adult mice.
Am J Physiol Heart Circ Physiol 2000;278:H652-7.
25.
Weiss RG, Chacko SM, Aresta F, Chacko VP. Dynamic magnetic resonance images of
murine cardiac function at physiologic heart rates. Circulation 2000;101:E92.
26.
Schmiedl U, Sievers RE, Brasch RC, Wolfe CL, Chew WM, Ogan MD, et al. Acute
myocardial ischemia and reperfusion: MR imaging with albumin-Gd- DTPA. Radiology
1989;170:351-6.
27.
Kahler E, Waller C, Rommel E, Hiller KH, Voll S, Broich A, et al. Quantitative regional
blood volume studies in rat myocardium in vivo. Magn Reson Med 1998;40:517-25.
107
28.
Pottumarthi PRE. Magnetic Resonance Perfusion Imaging. International Journal of
Imaging Systems & Technology 1995;6.
29.
Stark DaB, W. Magnetic Resonance Imaging. vol. 3. St Louis, Mo: Mosby; 1999.
30.
Frahm J, Merboldt KD, Bruhn H, Gyngell ML, Hanicke W, Chien D. 0.3-second FLASH
MRI of the human heart. Magn Reson Med 1990;13:150-7.
31.
Pettigrew RI, Oshinski JN, Chatzimavroudis G, Dixon WT. MRI techniques for
cardiovascular imaging. J Magn Reson Imaging 1999;10:590-601.
32.
Christensen G, Wang Y, Chien KR. Physiological assessment of complex cardiac
phenotypes in genetically engineered mice. Am J Physiol 1997;272:H2513-24.
33.
James JF, Hewett TE, Robbins J. Cardiac physiology in transgenic mice. Circ Res
1998;82:407-15.
34.
Lim TH, Choi Si. MRI of myocardial infarction. J Magn Reson Imaging 1999;10:686-93.
35.
Rehwald WG, Reeder SB, McVeigh ER, Judd RM. Techniques for high-speed cardiac
magnetic resonance imaging in rats and rabbits. Magn Reson Med 1997;37:124-30.
36.
Burstein D, Taratuta E, Manning WJ. Factors in myocardial "perfusion" imaging with
ultrafast MRI and Gd- DTPA administration. Magn Reson Med 1991;20:299-305.
37.
Simonetti OP, Kim RJ, Fieno DS, Hillenbrand HB, Wu E, Bundy JM, et al. An improved
mr imaging technique for the visualization of myocardial infarction. Radiology 2001;218:215-23.
38.
Wilke NM, Jerosch-Herold M, Zenovich A, Stillman AE. Magnetic resonance first-pass
myocardial perfusion imaging: clinical validation and future applications. J Magn Reson hnaging
1999;10:676-85.
39.
Bauer WR, Hiller KH, Roder F, Rommel E, Ertl G, Haase A. Magnetization exchange in
capillaries by microcirculation affects diffusion-controlled spin-relaxation: a model which
describes the effect of perfusion on relaxation enhancement by intravascular contrast agents.
Magn Reson Med 1996;35:43-55.
40.
Kuwatsuru R, Shames DM, Muhler A, Mintorovitch J, Vexler V, Mann JS, et al.
Quantification of tissue plasma volume in the rat by contrast-enhanced magnetic resonance
imaging. Magn Reson Med 1993;30:76-81.
41.
Schwarzbauer C, Syha J, Haase A. Quantification of regional blood volumes by rapid TI
mapping. Magn Reson Med 1993;29:709-12.
42.
Bauer WR, Schulten K. Theory of contrast agents in magnetic resonance imaging:
coupling of spin relaxation and transport. Magn Reson Med 1992;26:16-39.
43.
Bjerner T, Ericsson A, Wikstrom G, Johansson L, Nilsson S, Ahlstrom H, et al.
Evaluation of nonperfused myocardial ischemia with MRI and an intravascular USPIO contrast
agent in an ex vivo pig model. J Magn Reson Imaging 2000;12:866-72.
]OR
44.
Reeder SB, Faranesh AZ. Ultrafast pulse sequence techniques for cardiac magnetic
resonance imaging. Top Magn Reson Imaging 2000; 11:312-30.
45.
Pislaru SV, Ni Y, Pislaru C, Bosmans H, Miao Y, Bogaert J, et al. Noninvasive
measurements of infarct size after thrombolysis with a necrosis-avid MRI contrast agent.
Circulation 1999;99:690-6.
46.
Judd RM, Lugo-Olivieri CH, Arai M, Kondo T, Croisille P, Lima JA, et al. Physiological
basis of myocardial contrast enhancement in fast magnetic resonance images of 2-day-old
reperfused canine infarcts. Circulation 1995;92:1902-10.
47.
Wendland MF, Saeed M, Lund G, Higgins CB. Contrast-enhanced MRI for
quantification of myocardial viability. J Magn Reson Imaging 1999;10:694-702.
Miller S, Schick F, Scheule AM, Vogel U, Hiller R, Strotmann C, et al. Conventional
48.
high resolution versus fast T(2)-weighted MR imaging of the heart: assessment of reperfusion
induced myocardial injury in an animal model. Magn Reson Imaging 2000;18:1069-77.
Eng J, Ceckler TL, Balaban RS. Quantitative 1H magnetization transfer imaging in vivo.
49.
Magn Reson Med 1991;17:304-14.
50.
Scholz TD, Ceckler TL, Balaban RS. Magnetization transfer characterization of
hypertensive cardiomyopathy: significance of tissue water content. Magn Reson Med
1993;29:352-7.
51.
Williams DS, Detre JA, Leigh JS, Koretsky AP. Magnetic resonance imaging of
perfusion using spin inversion of arterial water. Proc Natl Acad Sci U S A 1992;89:212-6.
52.
Waller C, Kahler E, Hiller KH, Hu K, Nahrendorf M, Voll S, et al. Myocardial perfusion
and intracapillary blood volume in rats at rest and with coronary dilatation: MR imaging in vivo
with use of a spin- labeling technique. Radiology 2000;215:189-97.
53.
Horowitz A. MRI Physics for Radiologists. vol. 3. New York, NY: Springer; 1994.
54.
Finn P. Magnetic Resonance Imaging - Clinics of North America. vol. 7. Philadelphia,
Pennsylvania: Saunders Company; 1999.
55.
Andersen IK, Sidaros K, Gesmara H, Rostrup E, Larsson HB. A model system for
perfusion quantification using FAIR. Magn Reson Imaging 2000;18:565-74.
56.
Kroft LJ, Doornbos J, van der Geest RJ, Benderbous S, de Roos A. Infarcted
myocardium in pigs: MR imaging enhanced with slow- interstitial-diffusion gadolinium
compound P760. Radiology 1999;212:467-73.
57.
Prasad PV, Burstein D, Edelman RR. MRI evaluation of myocardial perfusion without a
contrast agent using magnetization transfer. Magn Reson Med 1993;30:267-70.
58.
Mitchell GF, Jeron A, Koren G. Measurement of heart rate and Q-T interval in the
conscious mouse. Am J Physiol 1998;274:H747-5 1.
109
59.
Berul CI, Aronovitz MJ, Wang PJ, Mendelsohn ME. In vivo cardiac electrophysiology
studies in the mouse. Circulation 1996;94:2641-8.
60.
Donahue KM, Burstein D, Manning WJ, Gray ML. Studies of Gd-DTPA relaxivity and
proton exchange rates in tissue. Magn Reson Med 1994 Jul;32(1):66-76.
110