Pooling and Segmentation to Improve Primary Care
Prescription Management
by
Thomas Daniel Sanderson
B.S.E. in Mechanical & Aerospace Engineering, Princeton University, Princeton, 2000
M.S.E. in Aeronautical Engineering, Stanford University, Palo Alto, 2008
Submitted to the MIT Sloan School of Management and the Engineering Systems Division
in partial fulfillment of the requirements for the degrees of
Master of Business Administration
________
MASSACHUSETT9 "lW'
and
Master of Science in Engineering Systems Division
OF TECHNOOGY
in conjunction with the Leaders for Global Operations Program at the
JUN 18 201
MASSACHUSETTS INSTITUTE OF TECHNOLOGY
L
June 2014
LIBRARIES
@ 2014 Thomas Daniel Sanderson. All rights reserved.
paper
publicly
distribute
to
and
reproduce
to
The author hereby grants to MIT permission
and electronic copies of this thesis document in whole or in part in any medium now known
or hereafter created.
Signature redacted
..........------------------A uth or .................
Division
MIT Sloan School of Management and the Engineering
May 9, 2014
Signature redacted.......-- .-.-....
RetsefLeji, Jhesis Supervisor
J. Spencer Standish (1945) Professor of Management, MIT Sloan School of Management
Certified by.........................--..
Signature redacted
. .. .........................---- -.-.-.....
David Simchi-Levi, Thesis Supervisor
Professor of Engineering Systems, Engineering Systems Division and the Department of
Civil and Environmental Engineering
C ertified by .....
Signature redacted
A pproved by ......
--..
.----- .--- ..............- ......Richard C. Larson
Systems
Engineering
of
Mitsui Professor
Chair,, 17i;ineering Systems Division Education Committee
Signature redacted
Approved by ..
-...---...
-...... -............--...
-...
Maura Herson
Management
of
School
Director, MIT Sloan
. . . ..
Pooling and Segmentation to Improve Primary Care Prescription
Management
by
Thomas Daniel Sanderson
Submitted to the MIT Sloan School of Management and the Engineering Systems Division
on May 9, 2014, in partial fulfillment of the
requirements for the degrees of
Master of Business Administration
and
Master of Science in Engineering Systems Division
Abstract
Analyses of schedule history and medical records for large primary care medical practice are
combined with time studies to develop a quantitative network flow model of the prescription
management process, including metrics for the yield of prescription requests, excess requests
for chronic & stable medications, and prescriptions that overflow from scheduled appointments. The model is used to estimate the impact of segmenting and pooling the prescription
workflows into a central prescription management group, resulting in recommendations for a
new prescription management system. Interventions on pharmacy/practice coordination for
faxes, modification of the voicemail system, and improved workflow are piloted to validate
model estimates. The recommended changes are expected to improve prescription response
time and accuracy, reduce resource utilization, improve patient medicine compliance and,
ultimately, patient health outcomes.
Thesis Supervisor: Retsef Levi
Title: J. Spencer Standish (1945) Professor of Management, MIT Sloan School of Management
Thesis Supervisor: David Simchi-Levi
Title: Professor of Engineering Systems, Engineering Systems Division and the Department
of Civil and Environmental Engineering
3
4
Acknowledgments
This work would not have been possible without the support of many contributors.
First and foremost, my eternal thanks to my wife, Carson, and my children: Daniel, Riley,
Audrey, and Cara. Without their support and understanding, I could not have participated
in the Leaders For Global Operations (LGO) program or performed this work at MGH.
Prof. Retsef Levi's dedication to better healthcare operations and always keeping the
patient at the forefront was personally inspiring and professionally motivating. His tireless
work, including supporting this project on a near-daily basis late into the night by teleconference from Israel, made the MIT/MGH collaboration, our work with Internal Medicine
Associates, and this project, possible.
Prof. David Simchi-Levi provided valuable support from the beginning to keep the goal of
this completed thesis in sight, to keep the right balance of business and technical rigour, and
to work seamlessly with Prof. Levi to navigate the complex waters of the LGO dual-degree
requirements.
Dr. Peter Dunn & Bethany Daily of MGH Perioperative Services placed their faith in
MIT and the LGO program to become partners, expanded beyond their own group for
the selfless benefit of MGH and all patients, expressed their confidence in an eager but
unfamiliar aerospace engineer, and provided a welcome voice of experience and hospitality
to help navigate the culture shock of the healthcare landscape.
Brianna Germain (Perioperative Services), Carine Yelibi (Primary Care Operational Improvement), and Mary Morgan (Lab of Computer Science) provided seamless access and
responded to unending questions regarding that holy grail of any operations project: administration and data!
Virginia Manzella, Dr. Sherry Haydock, Dr. Blair Fosburgh, and Dr. Daniel Horn of
Internal Medicine Associates opened their arms and offices to our team, willing to ask hard
questions and receive hard answers, and always put the good of their patients at the forefront
to allow outsiders to come in to help make better what they have dedicated so much of their
lives to.
Kaitlyn Kelley, Yolanda Fernandez, and Morgan Lichtenstein of Internal Medicine As-
5
sociates eagerly showed us the ropes and provided invaluable honest feedback from the
front-lines, at the expense of their own free time, when theory and reality collided.
Prof. Kate Kellogg of the Sloan School of Management provided valuable insight into the
"OP rich environment" of IMA.
Last, but by no means least, Cecilia Zenteno of the Sloan School of Management provided expertise, guidance, boundaries, support, friendship, discipline, a welcome perspective,
mastery of R and data processing, and a nearly unlimited supply of good coffee.
6
Contents
1
Introduction
1.1
1.2
2
. . . ... ...
.....
. . ..
..
. . . . . . . ..
..
. . . . . ..
15
1.1.1
Massachusetts General Hospital . . . . . . . . . . . . . . . . . . . . .
15
1.1.2
Primary Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
16
1.1.3
Internal Medicine Associates . . . . . . . . . . . . . . . . . . . . . . .
17
Project Overview
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
17
Literature Review
23
2.1
The Role Of Primary Care . . . . . . . . . . . . . . . . . . . . . . . . . . . .
23
2.2
Primary Care Prescription Management
. . . . . . . . . . . . . . . . . . . .
24
2.2.1
Drug Adherence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
24
2.2.2
Renewal Errors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
27
Improvement Due To Process Redesign . . . . . . . . . . . . . . . . . . . . .
27
2.3.1
Use Of Simulation
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
28
2.3.2
Interruption . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
28
2.3.3
Centralization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
29
2.3.4
Specialization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30
2.3
2.4
3
Background
15
Proactive Medication Management
. . . . . . . . . . . . . . . . . . . . . . .
30
Characterization of Resource Use In IMA
33
3.1
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
33
3.2
T im e Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
34
3.3
M ethods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
37
7
3.4
Data Collection & Analysis
. . . . . . . .
39
3.5
Time Study Results . . . . . . . . . . . . .
40
. . . . . . .
40
3.6
4
Schedule Performance
3.5.2
Distribution Of Time Across Tasks
42
43
Discussion . . . . . . . . . . . . . . . . . .
49
Designing An Improved Prescription Management Model
4.1
Current Process & Resource Use . . . . . . . . . . . . . . . . . . . . . . . . .
49
4.2
Operational Challenges . . . . . . .
. . . . . . . . .
51
4.3
M etrics . . . . . . . . . . . . . . . .
. . . . . . . . .
51
. . . .
. . . . . . . . .
53
4.3.1
Prescription Volume
4.3.2
Non-Actionable Prescription Requests (Yiield)
. . . . . . . . .
56
4.3.3
Spillover . . . . . . . . . . .
. . . . . . . . .
57
4.3.4
Excess Chronic & Stable
. . . . . . . . .
58
4.4
Rationale For Proposed Solution.
. . . . . . . . .
62
4.5
M odeling . . . . . . . . . . . . . . .
. . . . . . . . .
62
4.5.1
Model Formulation . . . . .
. . . . . . . . .
65
4.5.2
Modeling Results . . . . . .
. . . . . . . . .
66
Implemented Interventions . . . . .
. . . . . . . . .
69
4.6
5
3.5.1
4.6.1
Prescription Linking At The Pharmacy
. . . . . . . . .
69
4.6.2
Voicemail Renewal Line Ret rement . . .
. . . . . . . . .
71
4.6.3
Prescription Renewal Workflow
. . . .
73
77
Recommendations & Conclusions
5.1
R esults . . . . . . . . . . . . . . . . . . . . . .
77
5.2
Performance Metrics
. . . . . . . . . . . . . .
78
5.3
Pooling & Segmentation
. . . . . . . . . . . .
79
5.4
Proactive Medicine Management . . . . . . . .
80
5.5
Future Work . . . . . . . . . . . . . . . . . . .
80
5.5.1
Scheduling . . . . . . . . . . . . . . . .
80
5.5.2
Capacity Planning
. . . . . . . . . . .
81
8
A Role Observation Form
83
B Patient Observation Form
87
C Revised Renewal Line Voicemail Script
91
D Additional Time Study Observations
93
E
97
Network Flow Model Screenshots
9
THIS PAGE INTENTIONALLY LEFT BLANK
10
List of Figures
1-1
IMA Organizational Structure - each pod consists of a small independent
group of attending doctors and their related support staff . . . . . . . . . . .
1-2
MGH information system data sources & data processing relationships. Source
- M IT direct observation.
1-3
18
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
19
Prescription system drug adherence feedback loops. Note that all "No" arcs
are generally invisible to the practice or doctor such that non-adherence is
only identifiable when the patient fails to renew on time. . . . . . . . . . . .
3-1
Fraction of observed time spent managing prescriptions. Source - MIT direct
observations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3-2
21
36
IMA schedule performance. Delay - difference between scheduled arid actual
start time. Overrun - difference between scheduled and actual duration. Each
marker corresponds to a single appointment, with like symbols corresponding
to the sam e provider. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
41
3-3
Time distribution by task - Patient Service Coordinator (PSC) . . . . . . . .
44
3-4
Time distribution by task - Medical Assistant (MA) . . . . . . . . . . . . . .
44
3-5
Time distribution by task - Nurse (RN)
45
3-6
Time distribution by task - Nurse Practitioner (NP)
3-7
Time distribution by task -- Resident
. . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . .
45
. . . . . . . . . . . . . . . . . . . . . .
46
3-8
Time distribution by task - Attending (MD) . . . . . . . . . . . . . . . . . .
46
3-9
Time distribution by task - Preceptor . . . . . . . . . . . . . . . . . . . . . .
47
4-1
IMA current state prescription workflow - single pod
. . . . . . . . . . . . .
50
4-2
IMA current state prescription workflow - all pods . . . . . . . . . . . . . . .
50
11
52
4-3
Current state non-appointment prescription workflow - all pods
4-4
2012 Total prescription volume, by processing path
4-5
2012 Total prescription volume, by pod, by role. 2010 and 2011 are qualita-
. .
. . . . . . . . . . . . . .
53
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
54
4-6
2012 Total prescription volume, by delivery channel . . . . . . . . . . . . . .
55
4-7
Metric schematic - spillover prescriptions . . . . . . . . . . . . . . . . . . . .
58
4-8
2012 Total spillover prescriptions
. . . . . . . . . . . . . . . . . . . . . . . .
59
4-9
Metric schematic - excess chronic & stable prescriptions
. . . . . . . . . .
61
. . . . . . . . . . . . . . . .
61
4-11 Network flow model schematic . . . . . . . . . . . . . . . . . . . . . . . . . .
63
tively sim ilar.
4-10 2012 Total excess chronic & stable prescriptions
4-12 2012 daily prescription volume distribution and coefficient of variation, by pod 68
4-13 IMA future state workflow . . . . . . . . . . . . . . . . . . . . . . . . . . . .
69
. . . . . . . . . . . . . . . . . . . . . . . . . .
84
A-2 Role observation form, page 2 . . . . . . . . . . . . . . . . . . . . . . . . . .
85
B-i Patient observation form, page 1 . . . . . . . . . . . . . . . . . . . . . . . . .
88
Patient observation form, page 2 . . . . . . . . . . . . . . . . . . . . . . . . .
89
A-1 Role observation form, page 1
B-2
C-1 Revised Renewal Line Voicemail Script . . . . . . . . . . . . . . . . . . . . .
92
Screenshot - Model inputs, page 1 . . . . . . . . . . . . . . . . . . . . . . . .
98
E-2 Screenshot - Model inputs, page 2 . . . . . . . . . . . . . . . . . . . . . . . .
99
E-1
. . . . . . . . . . . . . . . . . . . . . .
E-3 Screenshot - contraint preprocessing
10 0
E-4 Screenshot - network adjacency matrix . . . . . . . . . . . . . . . . . . . . . 10 1
E-5 Screenshot - decision variables (current state) . . . . . . . . . . . . . . . . . 102
. . . . . . . . . . . . . . . . . . . . . . . .
10 3
. . . . . . . . . . . . . . . . . . . . . . . . . .
10 4
. . .
105
E-6 Screenshot - network constraints
E-7 Screenshot - path constraints
E-8 Screenshot - output (current state), page
E-9
Screenshot - output (current state), page 2
12
...
. . . . . ...
. . . ..
106
List of Tables
3.1
Total role observations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
40
4.1
Requested vs. issued prescriptions - normalized to 2012 total request volume
56
5.1
Future state m etrics
. . . . . . . . . . . . . . . . . . . . . . . . . . . . ..79.
13
THIS PAGE INTENTIONALLY LEFT BLANK
14
Chapter 1
Introduction
Like many other healthcare delivery systems, Massachusetts General Hospital (MGH) anticipates that its primary care practices will play a major role in slowing the growth of health
care costs through optimal management of distinct patient populations. Internal Medicine
Associates (IMA) is the largest primary care practice at MGH. As the first MIT Leaders for
Global Operations (LGO) engagement with IMA, this project had three primary goals: (i)
quantify how IMA currently utilizes resources; (ii) identify high-leverage areas for system
redesign; and (iii) develop a concrete implementation plan for one area.
1.1
1.1.1
Background
Massachusetts General Hospital
Massachusetts General Hospital (MGH) is the largest and oldest hospital in New England,
and is consistently ranked as one of the best hospitals in the country [1].
MGH handles
approximately 48,000 inpatients and 1.5 million outpatients annually, including: 90,000 ER
visits, 37,000 surgeries, and 3,600 deliveries. MGH originally partnered with the LGO program to improve operations in the Perioperative Services group, which supports all surgical specialties. Based on several successful prior projects ([14][43][39][38][42]),
MGH/MIT collaboration extended to include MGH Primary Care.
15
in 2013 the
1.1.2
Primary Care
Primary care practices provide long-term longitudinal care for patients, coordinating multiple specialists and referrals as necessary, and provide an important training environment for
medical residents. Historically, primary care providers have been the "gateway" to specialists
with separate diagnoses/billing/treatment/follow-up procedures for each group.
However,
rising medical costs and increasingly complex treatment options have highlighted the need
for better coordination among various caregivers for a single patient. As a result, insurance
companies are turning to primary care providers to integrate all of the various specialists
and treatments in the hopes of providing more cost-effective care, and modifying their reimbursement policies to match.
Accountable Care Organizations (ACOs) are groups of
doctors, hospitals, and other healthcare providers who come together under a unified Medicare reimbursement framework where, rather than fee-for-service to each provider, the entire
organization is compensated based on overall health outcomes. An analogous non-Medicare
structure, capitation, reimburses providers on a risk-adjusted per capita basis regardless of
the number or type of treatments required for any given patient. Both ACOs and capitated
plans use primary care as the lynch-pin of coordination and integration between the vast
array of other health care providers that a patient may require. This shift will change the
operating framework of primary care away from individual patient encounters and towards
managing health outcomes. The transition of primary care to a Patient-Centered Medical
Home (PCMH) model to support outcome-based reimbursement plans places primary care
at the forefront of healthcare cost containment efforts.
MGH provides comprehensive primary care services for 200,000 patients at 15 locations
[2]. MGH is also the original and largest teaching hospital of Harvard Medical School [1]. Like
many other primary care practices [46], MGH has observed increasing dissatisfaction and
burnout among primary care physicians due to stressful and chaotic work environments, increasing administrative and regulatory demands, fragmentation of care delivery, and greater
than ever expectations placed on primary care providers.
MGH is redesigning their pri-
mary care system to increase capacity, improve utilization, and resolve the sustainability
of primary care. One MGH primary care practice, Internal Medicine Associates, requested
16
MIT's assistance with this redesign due to the scope and scale of the practice and their acute
resource utilization challenges.
1.1.3
Internal Medicine Associates
Internal Medicine Associates (IMA), the largest and oldest primary care practice at MGH,
cares for 31,000 patients with a staff of 46 attending physicians, 59 resident physicians, 6
nurse practitioners, and 86 related clinical and administrative support staff.
IMA was originally created to provide a training environment to complete the primary
care residency requirement for students at Harvard Medical School. Over time, the practice
has grown as both the training and patient care needs of the MGH population increased.
Throughout the years, groups of attending physicians have split off from IMA to form other
primary care practices within MGH.
IMA is characterized by a unique parallel operations structure with 14 semi-independent
"pods", shown schematically in Figure 1-1.
This parallel structure has made IMA highly
scalable but presents significant challenges in performance tracking and change management
due to the autonomous nature of each pod. IMA's scale suggests that typical operations
management techniques, such as segmentation and pooling, may be useful to improve performance and reduce waste.
As the largest, oldest, and most complex primary care practice at MGH, IMA is both the
flagship for primary care innovation but also the most difficult implementation environment.
MGH has expressed a desire to increase the capacity (patients per IMA headcount) and
productivity (revenue per provider) at IMA to accommodate the increasing workload in
the changing primary care environment discussed in section 1.1.2. Due to its scale, success
in operational improvement at IMA will make a significant difference in patient care, and
viability of primary care, at MGH.
1.2
Project Overview
The first phase of this project (Section 3.2) quantifies how IMA currently utilizes resources.
This phase required extensive data analysis, leveraging existing data sources through the
17
Internal Medicine Associates (IMA)
Management (3)
Labs(3)
Shared Administration (6)
VCase--,i Mgrs (9)-
MDs (105)
NPs (6)
"a
"o
0
0
M
V
0.
"0
CD
V
0.
-0
I.'.
C,
a'-I
U,
RNs (22)
CD
LMAS (20)
PSCs (35)
Team 2
eam 1
Team 3
Source: IMA organization tables
Figure 1-1: IMA Organizational Structure - each pod consists of a small independent group
of attending doctors and their related support staff
18
IDXn
Scheduling
System
TSI Billing
System
Electronic
Medical
Record
Appotment
Prescription
(o120,000)
(C190,000)
s
Primary Care
Patient
Comorbidities
Direct
Observations
Pgo
pi ver,
N n-Actionable
Operations
Improvement
Data Source /
Algorithms
Processina
Data
Patient Loyalty
Cohorts
Project
Analysis D
te
Figure 1-2: MGH information system data sources &data processing relationships. Source
-- MIT direct observation.
MGH Primary Care Office Insight (PCOI) system and OnCall electronic medical record.
These systems provide detailed logs of all patients, appointments, medications, and prescriptions from 2010-2012. Figure 1-2 shows the relationship between different data sources,
some of which were created as part of this work. In addition, 127 hours of detailed quantitative time studies were performed with all staff roles across IMA to determine what aspects
of the current primary care model are consuming disproportionate practice resources.
The second phase of the project (Section 3.4) uses the results of the time studies&
data analysis to identify the highest leverage process changes for potential system redesign
efforts. Five high-leverage areas were proposed to the practice to select the first area for
implementation with an assessment of impact, feasibility, and interaction with other practice
19
operations.
This phase identifies prescription management as the first focus area due to:
significant resource utilization across all roles; widespread dissatisfaction with the current
state; lack of coupling with the compensation and scheduling processes; and relatively high
process control within IMA. The latter two points, in particular, simplify implementation.
The remaining focus areas (rescheduling load, scheduled appointment duration, patient panel
capacity analysis, and support staff capacity analysis) are discussed in more detail in Section
5.5.
The third phase (Chapter 4) uses the results from the prior phases, plus additional direct
observation of the current drug prescription management process, to develop a network flow
model of the current state in the clinic.
Model validation was determined by the match
between predicted and observed resource utilization for a given prescription load. Once calibrated, the model was used to quantify the improvement based on various centralization
options, developed in collaboration with the practice, for pooling and segmentation of the
various prescription management workflows. These quantified improvements were used to
select and develop the implementation plan for a new prescription management system. The
model was also used to study the opportunities for implementing proactive drug management to reduce prescription demand variance and volume, and to improve patient medical
adherence.
Due to the lack of system feedback for patient actions in the current prescription process
(Figure 1-3), we had to focus on operational/efficiency metrics derived from the interaction
of schedule, prescription, and drug data.
Historical logs of prescription output are com-
bined with three newly developed metrics: redundant/non-actionable prescription requests
(Yield), prescription requests done outside an appointment that could have been done at
an appointment (Spillover), and prematurely renewed prescriptions for chronic medications
(Excess chronic & stable). A network flow model estimates the resources required to process
non-appointment prescriptions under a variety of scenarios, measured in full-time-equivalent
(FTE) staff. One FTE is one person working forty hours per week, fifty weeks per year (two
weeks vacation per year are assumed).
Modeling shows that IMA currently expends 4.1 FTE to service non-appointment prescriptions.
This work is spread out part-time over an average of 28 nurses and medical
20
Yes
,,
,.
Pick up
drug?
Renew on
time?
NoY
Y sNo
Take drug
correctly?
No
No
Take
drug?
Yes
Figure 1-3: Prescription system drug adherence feedback loops. Note that all "No" arcs
are generally invisible to the practice or doctor such that non-adherence is only identifiable
when the patient fails to renew on time.
21
assistants, with work arriving at random intervals throughout the day and disrupting other
tasks. The 4.1 FTE estimate is a lower bound as it does not include the additional cost of
these disruptions. 15% of prescription requests are redundant/non-actionable, 4% of prescription requests could be done in an appointment but are not, and 8% of prescription
requests are due to chronic prescriptions being renewed early. A new prescription system is
developed to segment prescriptions away from other processes and centralize the prescription streams of multiple pods into one specialized group. Based on the expected reduction
in variance due to pooling, improved cycle times due to specialization, and the opportunity
to proactively identify and correct non-value-added prescription requests, we predict that
2-2.5 FTE will be capable of handling the entire non-appointment prescription load, a 37%
reduction in resource utilization that will free 28 nurses and medical assistants from frequent
interruption to allow them to focus on direct patient care.
A pilot intervention with a major New England retail pharmacy chain showed that proper
prescription linking could reduce redundant/non-actionable prescriptions requests by 35 to
50% (P-value < 0.05). The voicemail renewal lines will be modified to improve yield, then
eventually eliminated. Two dedicated staff will be added to the practice in 2014 to implement a centralized prescription management group, forming the foundation for proactive
monitoring and management of patient medicine compliance and drug-related health outcomes.
22
Chapter 2
Literature Review
2.1
The Role Of Primary Care
Primary care provides, directs, and arranges for all of a patient's healthcare needs [2]. Recent perspectives of primary care include the intention that preventative care coupled with
long-term management of chronic conditions will reduce the later use of high-cost high-risk
medical interventions. In particular, there is extensive literature that appropriate primary
care can improve outcomes and lower costs for many common chronic conditions: hypertension [10][29], diabetes [9], and cholesterol [29][12]. The quantitative savings of primary care
on many other comorbidities is an area of active research.
At the same time, primary care is facing a looming shortage of doctors. Relative to the
general population, primary care physicians are more likely to have symptoms of burnout
and be dissatisfied with worklife [44]. Most solutions proposed for the looming shortage of
primary care physicians entail strategies that fall into one of three categories: (i) train more;
(ii) lose fewer; or (iii) find someone else. A fourth strategy is now receiving more attention
based on inefficiency and waste in primary care today: improve productivity of the available
doctors to allow them to keep pace with the workload. If widely adopted, small efforts to
empower non-physicians, re-engineer workflows, exploit technology, and update policies to
eliminate wasted effort could yield the capacity for millions of additional patient visits per
year in the United States [45].
Practices that do show high performance and improved physician satisfaction show con-
23
sistent characteristics: proactive planned care, with previsit planning and previsit laboratory
tests; sharing clinical care among a team, with expanded rooming protocols, standing orders,
and panel management; sharing clerical tasks with collaborative documentation (scribing),
nonphysician order entry, and streamlined prescription management; and improving team
functioning through co-location, team meetings, arid work flow mapping [46].
In the context of this work, any improvement in primary care operations provides an
opportunity to reduce resource utilization, at least on a per patient basis. This may create
the opportunity to apply that freed capacity to improve care and/or mitigate the primary
care doctor shortage.
2.2
Primary Care Prescription Management
Within the primary care environment, the issue and maintenance of prescriptions consumes
a significant amount of resources and impacts the majority of patients (Chapter 4) but can
have major positive impacts on patient outcomes. For example, national survey data suggests
that statin therapy resulted in roughly 40,000 fewer deaths, 60,000 fewer hospitalizations
for heart attacks, and 22,000 fewer hospitalizations for strokes in 2008 [21].
As a result,
drug adherence (the degree to which patients comply with the intended drug therapy) and
prescriptions errors are of central concern to any primary care prescription management
system. Operational improvements discussed in this work can free resources to improve the
quality and responsiveness of the prescription system, improving health outcomes through
better adherence and decreasing costs by serving the existing demand more efficiently.
2.2.1
Drug Adherence
Adherence to the medical regimen continues to rank as a major clinical problem in the
management of patients treated with drugs arid life-style modification [33]. There is potential
for increased drug utilization to provide a net economic return when it is driven by improved
adherence with guidelines-based therapy [48]. Medication nonadherence is a growing concern
to clinicians, healthcare systems, and other stakeholders (e.g. payers) because of mounting
evidence that it is prevalent and associated with adverse outcomes and higher costs of care
24
[24]. Helping patients take their existing medication as prescribed is identified as one of the
most effective medical interventions to significantly improve the health of patients although
it does not require the latest technology or expensive medication [11].
One study showed that 66% of all Americans fail to take any of their prescription
medicines [22].
A pharmacy care program that coordinated primary care doctors, phar-
macists, and patients led to increases in medication adherence, medication persistence, and
clinically meaningful reductions in blood pressure, whereas discontinuation of the program
was associated with decreased medication adherence and persistence [29].
A similar study
found dyslipidaemia is a poorly-controlled condition in clinical practice largely because more
than 10% of patients are potentially non-adherent [56].
Chronic obstructive pulmonary
disease is frequently treated in a primary care setting; one study found 48% of patients
underadherent and 5% overadherent and found that age and number of drugs increase the
chance of underadherence [30]. Another study of antihypertensive prescriptions found 31.8%
non-adherence [57].
Among patients discharged with prescriptions for aspirin, statin, and
blockers after acute myocardial infarction, 34% of patients stopped at least 1 medication
and 12% stopped all 3 medications within 1 month of hospital discharge [24]. Another study
demonstrated that only 40% of patients were still taking statin medications 2 years after hospitalization for acute coronary syndrome and adherence was even lower for patients taking
statins for chronic coronary artery disease [24]. An antibiotic study found 20.7% of patients
failed to take the complete course of antibiotic treatment [40].
Simply providing patients with medication timetables and computer generated consumer
product information does not improve drug adherence in primary care [8].
In fact, even
filling prescriptions is a challenge. One study of a large database of electronic prescriptions
found only 78% of all prescriptions were filled. Of e-prescriptions for new medications, only
72% were filled. Efforts to increase adherence could dramatically improve the effectiveness
of medication therapy [20]. In 2004, an estimated 1.6 million Medicare beneficiaries (4.4%)
failed to fill or refill 1 or more prescriptions [28].
Metrics do exist to attempt to identify drug abuse, such as the Doctor Shopping Indicator (DSI) used to assess the relative abuse liability of benzodiazepines and to detect signals
of new patterns of abuse in settings where centralized records of prescription or deliveries
25
are available for the great majority of patients [37].
Other studies suggest that analysis
of prescription logs can assess medical compliance and correlates with patient drug effects
in general [50]; and that younger subjects, new patients, and those without comorbidities
should receive more meticulous monitoring of their medication-taking behavior [56].
Tra-
ditional methods of assessing non-adherence, mainly self-reporting, may be ineffective as
agreement between self-reported and refill adherences is poor to fair [34].
Currently, the
two most commonly used measures of medication adherence based on pharmacy data are
the medication possession ratio and the proportion of days covered methods, which essentially are defined by the number of doses dispensed in relation to a dispensing period [24].
These are similar to, but less specific, than the "excess chronic & stable" metric developed
in Section 4.3.4.
Improper and unnecessary use of medications cost over $200 billion in the US in 2012:
patients fail to receive the right medications at the right time or in the right way, or receive
them but fail to take them. Improvements are possible only through collaboration among
multiple healthcare stakeholders: providers, pharmacists, patients, payers, pharmaceutical
manufacturers and policymakers. In addition, healthcare informatics and analytical approaches to harness the value of data -
the use of technology
is a key driver of improvements
[5].
Some interventions have proven to be at least partially effective in addressing this issue. A
pharmacy care program led to increases in medication adherence, medication persistence, and
clinically meaningful reductions in blood pressure, whereas discontinuation of the program
was associated with decreased medication adherence and persistence [29].
However, one
study found that pharmacist contact with the patient by phone or fax was no better than
usual care [35], suggesting that the nature of pharmacist contact is important.
Plainly, improper prescribing and drug adherence imposes a significant burden on the
healthcare system in terms of poorer outcomes and higher costs. The operational improvements and new metrics discussed in this work provide a framework to improve the accuracy
and timeliness of prescriptions, and to detect potential non-adherence earlier and more effectively.
26
2.2.2
Renewal Errors
Some drug adherence issues are the result of incorrect or overly complex prescription management systems. Poorer-quality prescribing and primary care are associated with higher
medical spending in general and inpatient spending in particular [60]. Because many patients
have multiple chronic conditions, therapeutic regimens often involve multiple medications
and frequent daily dosing. Such regimen complexity may undermine effective chronic disease
management. Patients who are prescribed medications that must be taken multiple times per
day are less likely to adhere to their treatments than patients with simpler dosing schedules.
Interventions that simplify treatment regimens by reducing dosing frequency or by switching
patients to fixed-dose medication combinations result in substantial improvements in appropriate medication use [13]. Greater prescribing and filling complexity is associated with lower
levels of adherence. Patients with the least refill consolidation had adherence rates that were
8% lower over the subsequent year than patients with the greatest refill consolidation [13].
A large study of safety reports found medication incident reports represented 9.68% of all
patient safety incidents. There were relatively smaller numbers of medication incident reports from primary care, representing 8.5% of the total [15]. A UK study that evaluates the
efficacy of pharmacist-led, information technology-based intervention for medication errors
found it is an effective method in lessening the prescription errors [6].
2.3
Improvement Due To Process Redesign
There is considerable literature on the use of operations management principles (chiefly
modeling and process redesign) in the healthcare field, although application to the outpatient
primary care environment is significantly less common. One case of the application of lean
principles to an outpatient pharmacy also showed many recommendations similar to those
discussed in this work [26]:
e Answer more calls "live" whenever possible, rather than taking messages.
9 Relocate the pharmacy technician and the MA into the same office space
27
"
Utilize clerical staff to move necessary documents between the clinic and the renewal
office.
" Change the phone tree message for patients with clearer directions
This work, in part, explores the use and applicability of these techniques to the primary care practice prescription management environment and extends them via modeling
to provide quantitative predictions of expected performance after redesign.
2.3.1
Use Of Simulation
Discrete event simulation is a common technique to analyze the current state of healthcare
operations and suggest improvements. At MGH, a SICU and its six primary downstream
units were modeled in a highly detailed discrete event simulation. The validated simulation
is applied to evaluate the impact of several possible operational adjustments [14]. Another
study decreased the patient processing time and length of stay in the PACU through the
application of discrete event simulation [43]. Other simulation models are built to evaluate
the downstream effects of scheduling rules and discharge process changes in the perioperative
environment [39] [38].
Two known cases of simulation in an ambulatory care clinic, which is roughly comparable
to the primary care environment, also used discrete event simulation [49] [41].
2.3.2
Interruption
As discussed in detail in Chapter 3, primary care operations at IMA are characterized by
frequent interruption of tasks, especially for the support staff, by many different workflows
throughout the day. Interruptions have been described as extremely disruptive, as "constant,
constant, multitasking craziness", and as events that can cost a knowledge worker as much as
15 minutes in recovery time [31]. In one study, subjects' responses are substantially slower
and, usually, more error-prone immediately after a task switch [32].
In busy interrupt-
driven clinical environments, clinicians reduce the time they spend on clinical tasks if they
experience interruptions, and may delay or fail to return to a significant portion of interrupted
28
tasks. Task shortening may occur because interrupted tasks are truncated to "catch up" for
lost time, which may have significant implications for patient safety [55].
2.3.3
Centralization
The new prescription management system proposed in Chapter 4 relies, in part, on taking
advantage of centralization to enable pooling benefits.
In this context, pooling refers to
combining two or more independent but similar workstreams into one stream handled by
one entity. This provides two primary benefits:
(i) the variability, measured by standard
deviation or coefficient of variation, of the combined workload is lower than the sum of
the individual workloads; and (ii) the combined workload is larger, allowing the central
processing entity to devote a greater fraction of their capacity to the pooled workstream.
There is considerable research on the positive benefits of centralization in the healthcare
environment.
Uniform standards, vocabularies, and centralized knowledge structures and services could
reduce rework by vendors and care providers, improve dissemination of well-constructed interventions, and accelerate the movement of new medical knowledge from research to practice [54]. Centralization of coronary revascularization procedures in two Calgary hospitals
resulted in a higher rate of procedures with shorter hospital stays and more-favorable shortterm outcomes despite sicker patients [23].
Centralization of esophageal cancer surgery
improved outcomes even with more severe comorbidity [58].
Specialist cancer centers that
centralized surgical care reduced the number of adverse events in patients with pancreatic
cancer [59].
Centralization of pharmacy services results in decreased inventory costs [53].
A centralized prescription network with filled prescription feedback reduced inappropriate
prescription filling of opioids by 32.8% and benzodiazepines by 48.6% [19]. Centralized pharmaceutical services, pharmacist consultation and drug use review significantly reduced drug
use and medication costs [51]. Centralization of travel medicine service reduced pharmacy
costs by 17% due to better adherence to expert recommendations [7].
29
2.3.4
Specialization
In addition to pooling benefits, centralization allows employees to specialize in their tasks.
One primary-care redesign that included on-site physician pharmacy dispensing improved
patient medication adherence [52].
Application of operations management principles to
improve quality through specialized employees and processes increased accountability, drove
improvement, and produced savings [27]. Care guides, a specialized non-licensed care role,
can improve care for some patients with chronic disease at low cost [3][4].
Drug experts,
such as pharmacist or pharmacy technicians, can improve prescribing, reduce health-care
utilization and medication costs, and contribute to clinical improvements in many chronic
medical conditions, such as cardiovascular disease, diabetes, and psychiatric illness [18].
By centralizing prescription management in the primary care environment, this work
seeks to gain the benefits of less interruption and greater specialization that have been
observed in other areas of health care operations.
2.4
Proactive Medication Management
A future benefit of creating a centralized prescription management group is the capability
to switch from reactive to proactive medication management. The use of electronic medical
record data to generate information regarding control status and successful drug regimens
used by similar patients to develop collective experience decision support is both technically
possible and promising [16]. Thoughtful implementation and strategic workflow redesign can
mitigate the disproportionate electronic health record related work burden for clinicians, as
One study of a pharmacist intervention to
well as facilitate population-based care [25].
proactively improve patient health literacy improved adherence in patients with adequate
and inadequate health literacy [36].
In a large health maintenance organization, a case-
management system was considerably more effective than usual medical care for modification
of coronary risk factors after myocardial infarction [17].
Medication synchronization also becomes possible with a central prescription group. Synchronized, bundled prescription renewal is a systematic approach to prescription management
that can decrease patient inconvenience, support medication adherence, and save one to two
30
hours of physician and staff time daily [47].
31
THIS PAGE INTENTIONALLY LEFT BLANK
32
Chapter 3
Characterization of Resource Use In
IMA
3.1
Introduction
Internal Medicine Associates (IMA) is characterized by many semi-autonomous pods. Each
pod has its own team of doctors and staff who serve non-overlapping panels of patients.
Based on interviews with key IMA members, we suspect considerable variation between and
inside pods with respect to roles and responsibilities of different staff members and task
flows. The organizational structure of IMA was previously illustrated in Figure 1-1. Each
pod typically contains the following roles:
Attending (MD): A primary care doctor who has completed their residency and has a
panel of patients that they care for in the practice. MDs may be part-time or full-time
depending on the number of clinical sessions they have per week, and may have other
duties within the hospital or surrounding research environments. MDs diagnose and
treat patients, and provide guidance and medical orders to support staff.
Preceptor: An attending who oversees the medical actions of one or more residents.
Resident: A doctor who has completed medical school but is in some phase of their three
year residency. All medical residents perform at least some primary care work, although
33
many will eventually assume other specialties. All residents at IMA have a small patient
panel and perform essentially the same medical tasks as an attending but all of their
work must be reviewed and approved by a Preceptor.
Nurse Practitioner (NP): An advanced-degree nurse with some diagnostic and prescription authority who can provide autonomous healthcare decisions for less complex medical issues but may require consultation from an MD for more complex issues. Some
NPs may also have their own patient panel.
Nurse (RN): A licensed medical provider with a nursing degree, trained to perform many
medical procedures under the orders of an MD. RNs triage patients as needed, over
the phone or on arrival to the practice, and provide intra-visit followups and patient
education. RNs do not have prescription authority.
Medical Assistant (MA): A non-licensed medical support staff with some training in
basic diagnostic procedures, such as taking height/weight/blood pressure/pulse. MAs
help prep the patients for appointments, escort them to/from the exam rooms, assist
the doctors during the appointment as needed, and generally facilitate the physical
flow of patients through the practice. They also perform the administrative processing
of prescriptions, referrals, prior authorizations, and related patient paperwork.
Patient Service Coordinator (PSC): A non-licensed administrative support staff who
handles practice communications (faxes, phone calls, walk-ins); checks patients in and
out at the front desks; preps and processes charts and billing forms; and performs
all doctor and patient scheduling. They also work together with the MAs to process
administrative paperwork for patients.
3.2
Time Study
Existing datasets from the PCOI group (Figure 1-2) provide excellent visibility of scheduled
patient load and actual patient arrivals, but do not capture work not associated with an
appointment, the breakdown of effort required by different roles during appointments, or the
difference between scheduled and actual appointment duration.
34
To fill in this missing information, we conducted a structured time study of 36 members
of the practice across seven roles (PSC, MA, RN, NP, resident, MD, and preceptor) across
all pods. This effort generated 127 hours of data including task, duration, physical location,
and interaction with other members of the practice. This provided a detailed view of the
practice current state: workflows, task allocations, staff interaction, and "pain points". This
effort also helped meet the goal of mapping out major challenges and opportunities, and
analysis of the resulting data quantitatively confirmed several hypotheses based on observed
workflow and interviews with IMA team members:
" Prescription management load falls primarily on the nurses and medical assistants
(Figure 3-1)
" Pre- and post-visit work falls primarily on the PSCs and attendings
" Non-visit care forms the majority of the nurse workload
However, the data also shows a significant fraction of time for non-nurse roles spent on
non-visit care.
This has significant implications for practice reimbursement under a fee-
for-service model, as most of this work is not billable, but under future Accountable Care
Organization/capitated reimbursement this type of non-visit care will be essential.
The data also shows a statistically significant tendency for appointments to start late,
to run over, and a positive correlation between delay and overrun (Figure 3-2). This quantitatively validates the providers' and patients' anecdotal experience of waiting room delays
and providers' motive to "give patients a more thorough appointment if they've been kept
waiting."
Other general findings include:
" Very low level of non-work activity (breaks, lunch, etc.): staff spend essentially all of
their time directly performing IMA work
" Low level of cross-pod interaction
" Each pod has its own "process personality", which presents challenges for clinic-wide
implementation
35
Prescription Management - Fraction Of Observed Time
50%
40%---
40%-
-
-~-
----
-
-
-
-
-
-
-
-
-
-
----
----
-
-
E
0 0%
p0%
20%-
-
*-
---
-
f
-
0%~~.~
-
----
-tl
--
---
--
-
---
-
,
[
...............
t
~Q~
k
1Q.11
....
Od
d
~<
Figure 3-1: Fraction of observed time spent managing prescriptions. Source - MIT direct
observations.
I
36
* Many small IT problems generate rework and confusion
" Implementation of quality improvement initiatives, such as team huddles, is very inconsistent across pods and providers
* A large portion of non-visit patient contact takes place through the phone
* Low consistency between pods of assignment of tasks to roles
In addition to supporting prescription management improvement, the time study data provided insight into several potential avenues of future work (see Section 5.5 for details).
3.3
Methods
Quantifying the current state is necessary to determine how and where IMA is expending
its resources, support development of alternative care delivery models, and provide baseline
data for decision support tools to quantify the benefits/risks of any proposed changes.
The basic work unit for patient care within IMA is an appointment. Providers support
appointments in half-day sessions while other staff support providers/patients/appointments
in pairs of sessions (two sessions equals one work day). The observation data collection plan
has two main targets: 1) follow patients at each step of their appointments, and 2) follow
staff members through a complete session. This approach aims to capture the process flow
from both a patient-centric and IMA operations standpoint.
Sessions were used as the
basic observation unit to match up with the scheduling system. Samples of the observation
forms developed to capture data are provided in Appendix A and Appendix B. The major
components of each observation are:
" Info Blocks: Identify the date/time/location/role/etc. of the observation
" Time: recorded to the nearest minute
" Location: physical location within the practice
" Staff present: What other practice members are interacting with the observed person
37
*
Activity: What task the observed person was working on
* Notes: A free-text description of the task and any relevant information
The "Activity" fields were developed in consultation with IMA to provide a meaningful way to categorize the disparate activities conducted in the practice. Activities are first
divided as "Visit" (V) or "Non-Visit" (NV). Visit activities correspond to work required
to support a scheduled appointment, are associated with a patient physically present or
planned to be present, and are associated with practice revenue under a fee-for-service payment system.
Non-visit activities are everything else, including Population Management
(PM), patient care not associated with an appointment (Intravisit care, or "Intra"), and
administration. Detailed guidelines for assignment activities are printed on the back of the
observation forms (included in Appendix A & B) and repeated here for convenience:
" Visit: Work associated with a specific billable/scheduled visit (past, present, or future)
- Pre: Work to prepare for the patients visit
- Treat: Working with a patient
- Post: Work to follow-up on patients visits that already occurred
- Oth: Anything else related to a particular visit (see the notes field for details)
" Non-visit: Work not associated with a specific billable/scheduled visit
- PM: Population management (as defined by IMA role documents)
- Intra: Care for patients not directly tied to a visit (letters, emails, calls, consultations, prescriptions, etc.)
- Adm: Administrative work not related to any patient or population need
- Oth: Anything else
Observers did not interact with patients and were not present in the exam room per current MGH Internal Review Board (IRB) guidelines. Individual staff members were followed
at each step through a session. When appropriate, the time that patients entered or left
38
the exam room or interacted with observed roles was recorded. Role/pod combinations were
chosen with guidance from IMA to provide a representative spread across the practice.
Completed forms were scanned and form data was transcribed for analysis. This dataset
includes all of the information captured on the observation forms as well as the following
derived data:
" Duration: The time, in minutes, for each line
" Rx-Related: A TRUE/FALSE flag for whether a line is related to prescription handling,
determined by the text "rx" or "presc" in the notes field
3.4
Data Collection & Analysis
We initially proposed tracking two patients per session in ten different pods (twenty patients,
ten sessions) with patients selected in concert with the MDs approximately 2-3 days ahead
of the session. Identified patients would have been informed by the PSC at check-in using
an IMA-approved script. After initial role observations it was clear that this approach was
unnecessary, as most patient interactions were observed in the process of the role observations. As a result, only eleven dedicated patient observations were completed by recording
the time that particular patients arrived in the practice and moved from one practice staff
member to another. This data is identical to that captured while observing roles, and the
11 dedicated patient observations were combined with the role observations to cover a total
of 77 appointments.
We initially proposed tracking one of each of the eight major patient-facing roles through
a session in at least two different pods (three observations per role, twenty-four observations
total, twenty-four sessions). As the observation effort progressed, the following changes were
made with IMA concurrence:
* Patient Service Coordinator (PSC): Increased from 3 to 9 due to request from the
Operations Manager and recognition that observing the PSC was the most effective
way to see overall pod workflow
9 Medical Assistant (MA): Increased from 3 to 4 due to scheduling
39
Table 3.1: Total role observations
Role
Preceptor
Attending
Resident
Nurse Practitioner
Nurse
Medical Assistant
Patient Service Coordinator
Total Observations
Observations
3
9
2
3
6*
4
9
36
Total Duration (hh:mm)
127:12
* - In one case, two observers shadowed the same nurse at the same time. Thus, in the
quantitative analysis N = 5 for nurse observations.
" Nurse: Increased from 3 to 6 to capture more data for Non-visit care activities
" Resident: Reduced from 3 to 2 due to similarity to attending observations and time
constraints
" Attending: Increased from 3 to 9 to increase practice confidence in the validity of the
attending data
The final distribution of role observations are provided in Table 3.1.
A total of three different observers were used to compile the observations. Initial observations were done in pairs to improve consistently between observers.
3.5
Time Study Results
This section discusses both the qualitative and quantitative findings from the time study.
Observations highlighted several system design challenges that could be addressed to improve
practice operations.
3.5.1
Schedule Performance
As part of the provider observations, many patients interacted with the providers. Comparison of the times the providers entered and left the exam room with the schedule allows
40
Schedule Performance by Provider
Excluding NPs
Gn Bn
[Getting Behind
11 Providers (2 Residents, 9 Attendings)
1
37 Follow-Up (2 post-discharge)
28 Annuals
7 AWV
5 Urgent
Time measured from when provider enters the room
with the Pt until provider leaves the room for the last
Average appointment Is delayed
27 minutes and takes 4 minutes
longer than scheduled
40
+
time.
-
C
20
8
I
A
0~nnn
IRunning
Ea
Earl
o
_0
-40~
0A
*
~~~~
I-A
-
0
80
100
*0
Crvdr
0
10
1
Provider 3
Running Late
X Provider 4
0+
O Provider 5
Provider 6
20
-Provider 7
-Provider 8
#Provider 9
*Provider 10
Provider 11
*Average
40
Catching Up
+
-
++
++
~X~ o-Provider
60
0 4'0
0A
-
+
++
I
Delay [Minutesl
Mean Delay, Ratio, and Overrun are statistically siginificant
(P<0.01) by t-test and Wilcox signed-rank test.
(IMA Schedule Performance.jmpprj)
Figure 3-2: IMA schedule performance. Delay - difference between scheduled and actual
start time. Overrun - difference between scheduled and actual duration. Each marker
corresponds to a single appointment, with like symbols corresponding to the same provider.
41
calculation of the appointment delay and overrun. The aggregate results are shown in Figure
3-2. Significant items include:
" A "perfect" scheduling system would cluster around the origin (0 delay, 0 overrun)
" The average appointment is both delayed and overrun, to high statistical significance
" There is clustering by provider: providers tend to be consistently on time or consistently
late
" There is a statistically significant (P-value <= 0.05) positive correlation between overrun and delay. Once a provider is delayed, they are more likely to overrun and become
further delayed for subsequent appointments.
Distribution Of Time Across Tasks
3.5.2
It is helpful to look at the observation data in terms of what fraction of each roles' time is
taken up by different tasks. See Section 3.3 for detailed task definitions. Figures (3-3) - (3-9)
show the fraction of observed time spend on each task with one figure per role in standard
boxplot format. Note that each fraction is the total of many very small (1-2 minute) tasks
and there is wide variability within roles and across roles, consistent with the observation of
significantly varying workloads and processes across pods and throughout the day.
Figure 3-3: Based on responsibilities we expect PSCs to have a high fraction of pre- and
post-visit work and non-visit administration, and this is the case. However, the nonvisit intra activity (patient care not associated with an appointment) is equally significant. This is driven primarily by PSC handling of clinical phone calls and faxes
(prescriptions, referrals, etc.).
Figure 3-4: As expected based on responsibility, the medical assistants spend a high fraction of their time supporting visit activities.
However, as with the PSCs, note the
significant fraction of non-visit care (NV-Intra) time.
Figure 3-5: As expected, the nurses spend the majority of their time on non-visit care
(primarily triage phone calls, follow-up phone calls, and prescription management).
42
However, note the extreme variability across the observed nurses, suggesting substantially different nurse workflows between pods.
Figure 3-6: Comparable to attendings and residents, nurse practitioners spend the majority
of their time on patient treatment. However, as expected for their flexible role, the
nurse practitioners spend a greater fraction of their time on intravisit care (NV-Intra).
Figure 3-7: As expected, residents spend the majority of their observed time actually treating patients. This pattern is very similar to attendings, as we would hope, but with
smaller spread (likely due to the small sample size).
Figure 3-8: Similar to residents, attendings spend the majority of their time on patient
treatment during a visit. However, note the higher pre- and post-visit load and larger
spread compared to resident data.
Figure 3-9: Consistent with the observed preceptor workflow, preceptors spend the majority of their time on visits and post-visit consultation with residents.
3.6
Discussion
Based on the combination of direct observation, data logs for appointments and prescriptions,
and derived metrics discussed in detail in Section 4.3, we identify prescription management
as the first area to make a concrete intervention in the practice.
Chapter 4 details the
analysis, modeling, and proposed operational changes to address prescription management
at IMA. In the course of performing the observations, the MIT team also noted several more
general operational items of interest, which are provided for reference in Appendix D.
43
Patient Service Coordinator (N=9)
90%
Non-FFS Work
80%
E
iZ 70%
2
60%
IA
50%
0
4-
o
----..........
40%
.....
30%
20%
10%4
0%
V-Pre
V-Treat
V-Post
V-Oth
V-Adm
NV-Intra
NV-PM
NV-Adm
NV-Oth
Task Category
Source: MIT Observation Data
Figure 3-3: Time distribution by task
-
Patient Service Coordinator (PSC)
Medical Assistant (N=4)
100%
Non-FFS Work
80%
E
P 70%
M
? 60%
0
.4-
o
2
LA.
40%
S 30%------.........
20%
0%
V-Pre
Source: MIT Observation Data
V-Treat
V-Post
V-Adm
V-Oth
NV-Intra
NV-PM NV-Adm
NV-Oth
Task Category
Figure 3-4: Time distribution by task - Medical Assistant (MA)
44
Nurse (N=5)
90%
Non-FF S Work
80%
E
R
70%
"a
2
----
60%
2 0% -@
-
-
10%
0%
V-Pre
Source: MIT
V-Treat
V-Post
V-Adm
V-Oth
NV-Intra
NV-PM
NV-Adm NV-0th
Observation DataTakCtgr
Figure 3-5: Time distribution by task
(RN)
-Nurse
Nurse Pracitloner (N=3)
100%
90%
Non-FS Work
80%
Task Category
-0
0%
6
40%
10%
___
20%
V-Pre
Source: MIT
V-Treat
V-Post
V-Adm
V-Oth
NV-Intra
NV-PM
NV-Adm
NV-Oth
Observation Data
Figure 3-6: Time distribution by task - Nurse Practitioner (NP)
45
Resident (N=2)
100%
90%
Work
80%
E
70%
60%
.0
UC
0
50%
40%
30%
LL
20%
10%
0%
V-Pre
V-Treat
V-Post
V-Adm
V-Oth
NV-Intra NV-PM
NV-Adm
NV-Oth
Task Category
Source: MITObservation Data
Figure 3-7: Time distribution by task - Resident
Attending (N=9)
100%
90%
Non-FFS Work
80%
E
0l
0
4-
70%
- -
-....
..
..-
60%
50%
.0
4-
0
40%
30%
LL
20%
-------------
----
10%
0%
V-Pre
Source: MIT Observation Data
V-Treat
V-Post
V-Adm
V-Oth
NV-Intra
NV-PM
NV-Adm
NV-Oth
Task Category
Figure 3-8: Time distribution by task - Attending (MD)
46
Preceptor (N=3)
-
-
100%90%-
E
Gj-
Non-FFS Work
0%
70%
60%
_
-
_-
60%
------
50%
-
-
040%-
ge0m-
-
-
NV-PM
NV-Adm
0%
L 20%
-
-
1lll11
1
10%
0%
V-Pre
Source: MIT Observation Data
V-Treat
V-Post
V-Adm
V-Oth
akC tg
NV-Intra
r
Figure 3-9: Time distribution by task - Preceptor
47
NV-Oth
THIS PAGE INTENTIONALLY LEFT BLANK
48
Chapter 4
Designing An Improved Prescription
Management Model
4.1
Current Process & Resource Use
Based on the data in Chapter 3, prescription management represents a significant consumer
of IMA resources and shows several opportunities for improvement, including: improvement
of the yield of prescription request, reducing excess prescription requests, improving the
number of prescriptions dealt with during appointments, and improving the overall workflow
so that proper prescription requests are fulfilled in the most efficient way.
In order to quantify resource utilization in terms of Full-Time Equivalent (FTE) staff, we
document the current state workflow, develop new operations metrics, and develop a network
flow model of to quantify resource utilization in the current and recommended future states.
The model shows the practice utilizes an average of 4.1 FTE to service non-appointment
prescription requests. This estimate is consistent with the utilization noted during direct
observation.
Direct observations and interviews with key practice members were used to generate
the current state workflow (Figure 4-1). This simplified model neglects some niche request
processes, such as direct emails to doctors or walk-ups, because these are workflow equivalent
to modeled workflows (a direct email to a doctor is routed similarly to a web request, a walkup is routed similarly to a voicemail request). It is important to note that, since each pod
49
PSC
Fax
Voiceail
.
MA
-
RN
WE
-Cosign.
MD/NP
Pharmacy
Figure 4-1: IMA current state prescription workflow - single pod
Fax
n
PSC
nsin
MA
Vicemail
nn
Web
RN
Cosign
MD/NP
PharMacy
Figure 4-2: IMA current state prescription workflow - all pods
50
is operationally independent, the actual practice workflow is highly parallel as illustrated in
Figure 4-2. This allows us to model an "average pod" as one fourteenth of the total practice.
4.2
Operational Challenges
IMA staff are frequently interrupted and spend significant time refilling prescriptions. As
expected from discussions and workflow, the prescription load falls heaviest on the nurses and
medical assistants. Note that, due to the IRB restriction to not be in the room with patients,
the NP/attending/resident fractions do not include prescription management that may have
happened during an appointment. This did not influence the final recommendations because
the process redesign is focused on the non-appointment prescription process.
Figure 3-1 shows the cumulative amount of time spent on prescriptions as a fraction of
total observed time. This work typically occurred in many very short (1-2 minute) increments
throughout a session. In addition to the time spend on handling the prescription, there is
an associated cost of switching tasks so frequently (see Section 2.3.2 for relevant literature).
Figure 4-3 shows the aggregate observed prescription workflow. Note that no single pod
was observed to execute all of the possible workflows; the complex nature of the workflow
in figure 4-3 is a result of high variance in the prescription workflow between pods. Within
any particular pod, the actual workflow also varied depending on the provider, drug, request
path, and output path.
4.3
Metrics
In addition to the extensive time studies discussed Chapter 3, a full characterization of
IMA resource utilization must include an analysis of the different input, processing, and
distribution channels for prescriptions. Metrics to quantify operational performance of each
channel are also developed.
51
OnCall'
Paper File
PCa
et
Rx Line
iHealthspace
Email
Pharmacy
Main Phone
Fax
Figure 4-3: Current state non-appointment prescription workflow - all pods
52
Prescription Flow - IMA 2012
Rx data from OnCall
Appt data from IDX
Issued
R qestday
of
90
8
4
MD/NP
81,264
4
18972
appointment
4,82
Request via
iHealthspace
4 40
538
Issued byyRRN
,343
33,
2
30,65
7,904
A
is,92
45
PMaatient
Ise
5
88,
84
5
5,54
183x655
Logged Rx
Hadc
Patient
5,341
by
Email hone/Fax
Other
Pharmacies
53
P26
6,65
CVS
Figure 4-4: 2012 Total prescription volume, by processing path
4.3.1
Prescription Volume
The prescription logs from the electronic medical record include the data for every prescription (patient, drug, dose, frequency, doctor, etc.), as well as a variety of useful metadata
(person who actually created the prescription, distribution channel, pharmacy, etc.). Analysis of this data with respect to the known location of each doctor and nurse within the
practice identifies, for each prescription, the corresponding pod and distribution channel.
We further make the assumption, supported by direct observation and interviews with support staff, that prescriptions issued for a patient on the day of an arrived appointment were
written by the doctor during face-time with the doctor.
This allows us to separate pre-
scriptions into appointment-based and non-appointment-based.
The annual traffic for the
entire practice by channel is shown in Figure 4-4. This can also be broken down by pod and
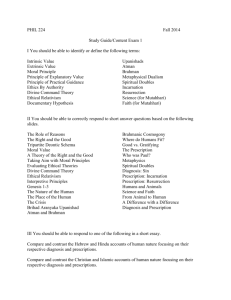
prescription issuer as shown in Figure 4-5.
Prescription volume can also be assessed in terms of delivery channel, as shown in Figure
4-6. Electronic prescriptions, by necessity, are coded with the destination pharmacy and this
data is captured in the prescription log. One retail pharmacy network is, by a wide margin,
the largest filler of electronic IMA prescriptions.
The second highest volume channel is
hard-copy prescriptions handed or mailed to the patient; the final destination of these hard-
53
Prescription Volume By Pod - 2012
URGENT CARE
U MA
N
10
1
MD
9
m NP
8
7
N RN
6
0
5
4C
4B
4A
3
2
1B
W
1A
0
5000
15000
10000
Issued Prescriptions
20000
25000
Figure 4-5: 2012 Total prescription volume, by pod, by role. 2010 and 2011 are qualitatively
similar.
54
100000
100%
90000
MVolume
80000
-Cummulative
%
80%
70%
70000
.0
90%
'
W
60000
60%
6%W
50%
50000
0000
30000
40%
30%
20000
20%
10000
10%
3'
0
3
E
0-0%
Prescription Delivery Channel
Figure 4-6: 2012 Total prescription volume, by delivery channel
copy prescriptions is invisible to the practice, which increases the challenging of tracking
prescriptions through fulfillment and ultimate drug adherence.
If we assume that hard
copy prescriptions are allocated among pharmacies in the same proportion as electronic
prescriptions, the primary retail network is handling more than 40% of the total practice
prescription volume. This is a reasonable assumption because the decision of how to deliver
a prescription and which pharmacy to deliver it to are essentially independent; the OnCall
system will support any delivery method for any pharmacy and patients can freely choose
both the delivery method (excluding controlled substances) and the pharmacy. Due to this
high volume, the pilot pharmacy intervention discussed in more detail in Section 4.6.1 was
conducted with a major retail pharmacy network.
55
Table 4.1: Requested vs. issued prescriptions - normalized to 2012 total request volume
4.3.2
Channel
Requested
Issued
Delta
Yield
Main Source
Web
Voicemail
Fax
3%
8%
47%
2%
5%
35%
<1%
3%
12%
93%
70%
74%
Patients
Patients
Pharmacies
Appointments
42%
42%
-
100%
Patients
Non-Actionable Prescription Requests (Yield)
The prescription logs are only recorded when a prescription is actually entered into the
medical system. There is currently no tracking of requests for prescriptions as an independent quantity even though this is the primary driver of workload to the Patient Service
Coordinators and Medical Assistants.
We therefore augmented the raw volume measure-
ments discussed in Section 4.3.1 with direct observations of the inbound fax, voicemail, and
web processes to determine how many prescription requests actually occur to generate the
recorded issued prescriptions, the yield of the process. The results are shown in Table 4.1.
Yield: The ratio of issued to requested prescriptions for a particular request path
Of particular note is the high fraction of total volume moving through the fax process,
the very high yield of the web process, and the low yield of the fax and voicemail processes.
This suggests several qualitative drivers for operational improvement:
" Any improvement to the fax process has disproportionate impact due to its dominant
volume
" The web process is the most effective but also the least utilized; IMA had already
recognized this prior to this project and is currently implementing a plan to significantly
increase the number of patients using the web portal
" The voicemail system is both low volume and low yield; there is opportunity to either increase the yield through system modification or reduce the volume by shunting
patients to other, more efficient, input channels
56
4.3.3
Spillover
During direct observation, many support staff commented on a perceived high frequency
of prescription requests happening immediately before and after appointments.
This was
somewhat unexpected, as the in-appointment prescription renewal process was perceived
to be very efficient and doctors stated they made a concerted effort make sure patients'
prescriptions were up-to-date during any appointment. In order to quantify this observation,
we developed a new metric, "Spillover":
Spillover: the percentage of prescriptions that occur within two days of a scheduled appointment (before and after), but not on the day of the appointment
As discussed in Section 4.3.1, prescriptions on the day of an arrived appointment are considered to have been issued during the appointment. The method to compute Spillover is as
follows:
1. For every entry in the prescription log, identify the closest scheduled appointment in
time for that patient
2. Calculate the time differential as PrescriptionDate- AppointmentDate (a negative
value means the prescription was issued before the appointment)
3. Count all prescriptions with a time differential of -2,
-1,
1, 2 (not 0) days
4. Divide the count from Stem 3 by the total number of non-appointment prescriptions.
The resulting value is "Spillover".
The spillover concept is illustrated graphically in Figure 4-7. Spillover was 8.5% in 2012,
with comparable values in 2010 and 2011. The impact of spillover is shown in Figure 4-8:
spillover resulted in an extra 7,782 prescription requests going through the non-appointment
prescription renewal process in 2012, or 4% of the total prescription volume. The anecdotal
reports obtained during observations are supported by quantitative analysis; there is a high
volume of prescription activity surrounding each appointment. As a measure of effectiveness
of the in-appointment prescription process, spillover provides a useful measure of how much
unnecessary work the non-appointment renewal process performs to make up for prescriptions
57
(D
-2
1
0
1
Days From Arrived Appt
2
Figure 4-7: Metric schematic - spillover prescriptions
that, for whatever reason, were not issued during the appointment itself. Additional research
is required to determine the causes and addressability of any failures of the appointmentbased prescription process.
4.3.4
Excess Chronic & Stable
Prescription renewals benefit, at least in theory, from a relatively high degree of predictability.
The practice knows, via the electronic medical records, the prescribed drug therapy and
active prescription duration for every patient, therefore it should be relatively straightforward
to predict the incoming volume of renewal requests for at least certain classes of drugs and
patients. Absent other constraints (controlled substances, dose titration, one-time therapy),
the practice will always write a one year prescription.
Although the practice does not
currently monitor the list of outstanding prescriptions to predict when renewals should arrive,
we hypothesize that patients on chronic medications at constant dosage should be renewing
every 11-12 months (1.0-1.1 prescriptions per year). To test this hypothesis, we develop a
58
2012 Prescription Requests
2-day Spillover
Appt Spillover,
7782, 4%
Figure 4-8: 2012 Total spillover prescriptions
metric called "Excess Chronic & Stable":
Excess Chronic & Stable: Average prescriptions per year per patient for each
constant dose chronic medication prescribed for more than one year to that patient
The method to compute Excess Chronic & Stable is as follows:
1. Identify those classes of drugs typically prescribed chronically (multi-year therapies)
at constant dosage. For this study, these were:
" Anti-hypertensives
" Anti-lipemics
" Oral anti-diabetics
* Thyroid simulators
2. Filter the prescription list for the drug families identified in step 1.
As these are
annual prescriptions, this list must span multiple years for the calculation to be valid.
2010-2012 were used for this study.
59
3. Filter the resulting list for patients who have multiple prescriptions.
Patients with
only one are assumed to have either started or stopped therapy within the window of
interest, hence do not have a stable prescription pattern.
4. Filter the resulting list for prescription renewals at the same dose.
Dose changes
may indicate titration, revised lab results, or other clinical actions that prevent the
prescription pattern from being stable.
5. Calculate the average number of prescriptions per patient per year for the chronic &
stable prescriptions identified in step 4. This value defines "Excess Chronic & Stable."
If our hypothesis is correct, "Excess Chronic & Stable" should have a value of 1.0 - 1.1,
signifying patients renewing as their prescriptions run out at month 11 or 12. This expected
pattern is illustrated in the upper half of Figure 4-9.
However, processing of actual logs
shows a value of 1.8, equivalent to renewing every 7 months and shown in the lower half
of Figure 4-9 (t-test P-value
< 0.0001 against expected value of 1.1). This implies that a
significant fraction of prescription requests are not clinically necessary; the patient has an
active prescription with available refills but, for whatever reason, the patient is requesting
a new prescription well ahead of the expiration of the old one. This generates additional
workload on the practice for no clinical benefit and increases the likelihood of a prescription
linking error at the pharmacy. The volume generated by these excess requests is shown in
Figure 4-10. In 2012, prescriptions for chronic & stable drug therapies represented 20% of
the total volume, while almost half of that (8% of total volume) were excess. Reduction
of excess renewal requests represents a significant opportunity to reduce total prescription
volume without any impact to patient care.
In addition, as this definition of chronic &
stable is conservative, it is likely that a significant fraction of the remaining 80% of total
prescriptions are also renewed early. Thus, we expect 8% to be a lower bound for the amount
of excess renewals flowing through the system.
60
Expected: 1.0-1.1 renewals per year
I I I I
2010
2012
2011
2013
Observed: 1.8 renewals per year (avg)
I
2010
I111
2012
2011
2013
Figure 4-9: Metric schematic - excess chronic & stable prescriptions
2012 Prescription Requests
Chronic & Stable (C&S)
Figure 4-10: 2012 Total excess chronic & stable prescriptions
61
4.4
Rationale For Proposed Solution
A network flow model is built utilizing the observed workflow for the current state. Adding
nodes and arcs to the model allows alternative workflows to the overlaid on the current
state workflow, estimating volume and resource requirements for each potential prescription
workflow design.
The final network flow model is shown in Figure 4-11. The black network presents the
current state while the gray network represents the proposed future state. Separate processing and wait times are assigned to each arc. The model is formulated as a linear program
that attempts to minimize total processing time subject to flow constraints and traffic splits
that correspond to the observed metrics discussed in Section 4.3. In both the current state
and future state models, the constraints are binding, such that the feasible region is a single
point. As such, the model could also be developed as a series of linear equations and solved
directly. However, the network flow/optimization approach provides the option to introduce
arcs (workflows) that may expand the feasible region, preserving flexibility to find optimal
workflows during the iterative phase of experimenting with alternative process designs.
4.5
Modeling
The model takes, as input, the following:
Patients: Total patients, fraction of patients on medications, average prescriptions per patient per year, and daily standard deviation of prescription demand
Request Channels: The fraction of requests coming by the four primary channels (Appointment, Web, Voicemail, & Fax)
Metrics: The yield of each request channel (Section 4.3.2), spillover prescriptions (Section
4.3.3), and chronic & stable request ratios (Section 4.3.4)
Times: Task times based on the direction observation results (Section 3.4) and wait times
estimated with a dedicated discrete event simulation model
62
.2---------------------------------------Pharm.
A pts
p
Yield8
illage
/I .3
Ieb
1
Patients
6
Vmai
Yield
9
4
F
7
yied
10
Exce
12
Trash'
-+
-+
-
Calculated paths
Centralized paths
+ Constrained paths (logs)
Figure 4-11: Network flow model schematic
63
The model also includes parameters to account for the impact of various potential interventions and redesigns:
Interventions: Staffing level for the central prescription group, how many pods worth of
traffic to run through the centralized group, and the expected specialization and process
time savings in the central group.
Based on these inputs, the model calculates the input traffic of prescription requests by
channel (source nodes), and the output traffic of issued prescriptions (sink nodes). Metrics,
such as yield and spillover, define the ratio of traffic on different arcs. These calculations
are expressed as linear constraints and combined with the flow constraint that net flow on
non-source/sink nodes be zero. The cost matrices use the task and wait times to assign a
cost to each arc. The optimization model is built in Excel for easy portability and solved
using OpenSolver (the number of decision variables exceeds the capability of the native
Excel solver).
on each arc.
Solving the model to minimize total processing time provides the traffic
Total processing time on all arcs measures the FTE expended to serve the
prescription volume, while total weighted average wait+process time along all source-to-sink
paths provides the average expected cycle time.
The model also assumes that each pod's traffic can be modeled as one of fourteen independent identically distributed random variables that sum up to the observed practice
volume and standard deviation. As a result, the model can predict the mean and standard
deviation of volume for the separate pods and for the centralized prescription group.
The model outputs:
Volume: Total prescriptions issued, total non-actionable requests, total spillover and total
excess prescriptions issued
Variability: Coefficient of variation for the practice, each pod, and the central group, including average, +1-, and +2o- daily demand and FTE required
Savings: Average cycle time and wait time, including improvement against the current state
baseline
Resources: Total FTE, FTE by role, and utilization by role
64
4.5.1
Model Formulation
ij :Number of prescriptions flowing from node i to node
j
Nij :Node adjacency matrix, Ni= 1 if there is an arc from node i to
Cij :Wait time, per prescription, from node i to node
C
j,
0 otherwise
j
: Processing time, per prescription, from node i to node
M: "Infinity", larger than the largest value on any arc,
j
= 106
F : Indicator for use of central clinical processing, F = 1 when central clinical processing is
used, 0 otherwise
d:
The set of source (supply) nodes
.6:
The set of sink (demand) nodes for complete prescriptions
/
:The set of arcs from central administrative scrub node(s) to central clinical processing
node(s)
6: The set of arcs that carry excess prescriptions
0 : The set of sink nodes for waste prescriptions
Y :The set of arcs that carry spillage prescriptions
Decision Variables: xij
C
Minimize:
ij subject to:
ii
>
(Nixij) = Requestsi
Vi E q/
S (Nixij) = Outputs,
Vj E 9
5(Nijxij)
=
Waste,
65
Vj E 0
Z(Niixi)
= Excessii
Vij c g
Z(Nijxij) = Spillagei,
Vij c Y
ii
ii
Xij < (I - F)M
Z(Njxj)
-
Z(Nixji)
i
Vij E /
=
0
Vj 3 W
,//
i
As formulated, the model has 152 = 225 decision variables, one for each possible arc, and
27 constraints. In the final design, due to the relatively sparse network, there are only 29
active decision variables.
None of the arcs or nodes in this formulation are capacity limited as no portion of
the current IMA workflow saturates purely due to prescription load. A network including
capacity limits might be appropriate for future models that attempt to incorporate other
workflows that compete for practice resources, or if the prescription utilization of any node
in the workflow approaches 100%.
The model was validated by running it against actual input values from 2012 with no
process improvements (no centralization or specialization benefits) and comparing the model
outputs of predicted volumes to the actual logs of prescription outputs in 2012. The predicted FTE per pod was also compared to the fraction of time spent on prescription management found during direct observation (Figure 3-1), with essentially equivalent results after
accounting for pod-to-pod variation in workflow and load.
Screen shots of the as-implemented model inputs, adjacency matrix, and outputs are
provided for reference in Appendix E.
4.5.2
Modeling Results
Modeling shows that the practice currently devotes approximately 4.1 FTE to non-appointment
prescription management. This is notable for several reasons:
* This is the first time the practice has a quantitative estimate for the resource consumption of any dispersed parallel task
66
"
IMA is large enough that the prescription management task significantly exceeds one
FTE, therefore it is at least possible to make this a dedicated position. Most primary
care practices are too small to have dedicated staff for prescriptions but IMA has an
opportunity to leverage their scale to utilize specialized and dedicated roles.
" Based on bench-marking against other MGH primary care practices, IMA's prescription
management process is resource intensive. The next largest practice, Bullfinch Medical
Group, performs prescription management for 20,000 patients (2/3 of IMA's patient
population) using 1.0 - 1.5 FTE.
Modeling also shows that pooling all pods into a central prescription management group
would reduce daily coefficient of variation from 0.655 (per pod) to 0.175, assuming 14 average
and equal pods working in parallel (Figure 4-12). This compares favorably to the coefficient
of variation computed from the historic prescription logs, with an average pod coefficient of
variation of 0.49 dropping to 0.19 with full pooling for 2012 data. In FTE terms, this implies
that a
+2o- demand day (covering 98% of all days) would require an extra 0.7 FTE in an
individual pod, a 130% increase, but only an extra 1.4 FTE for the entire practice, a 35%
increase. The revised workflow with centralization is illustrated in Figure 4-13.
Centralization, by itself, does not imply a reduction in total workload since all the same
work must still be done. As a result, the model estimate of 4.1 FTE for the current state
also applies to the central prescription management group absent any other improvement.
However, the variability reduction of pooling means that a centralized prescription group does
not require as many resources to handle higher-than-average workload days. It is also well
established in operations literature that segmenting a particular process away from others
allows employees to focus and specialize, reducing task times and improving throughput,
simplifying change implementation, and easing troubleshooting. We undertook a series of
pilot studies to quantify how much improvement could be expected at IMA.
67
2012 Non-Appt Rx Load By Pod (N=145356)
200
0.50
a
i-I
180
A
160
0.45
.
0.40
- -T-i
--.-
-
4
.X Avg Pod
0.35
140
C
Each Pod
120
________-____________
100
.
80
0.30.!
Coefficient Of Variation
(CIN)
___T__I-
_______
Total Practice
-
-- - ----
----- -- -T
-- -
---
.
--K-v--+_____________/__)
0.25 0
C
0.20 tr~
60
- .
40
-
0.10
20
.
0.05
0
-
0.15
,
la
lb
1c
labc
2
3
4a
4b
Pod
4c
5
6
7
8
9
0.00
10
Figure 4-12: 2012 daily prescription volume distribution and coefficient of variation, by pod
68
Fax
Dupliates
Central
~
Voicemail
VoicmailMgmt
Drugq4-W011
MD/NP
Web
Pharmacy
R
Figure 4-13: IMA future state workflow
4.6
Implemented Interventions
Pilot interventions were conducted around reducing fax volume, improving voicemail yield,
and redesigned workflows to estimate how much the model inputs could be improved.
Incorporating the pilot results into a centralized prescription management process shows
that 2.0 - 2.5 FTE should be able to handle the entire non-appointment prescription load for
the practice, a 37% decrease in resource utilization. The central prescription management
process also provides the foundation for several future interventions necessary to implement
proactive medicine tracking and management for patients.
4.6.1
Prescription Linking At The Pharmacy
As discussed in Section 4.3.2, a significant fraction of total prescription requests are due
to non-actionable faxes. These typically take the form of duplicate renewal requests from
pharmacies: they request renewal of a prescription that has not yet expired or that was
recently renewed. MGH Back Bay, a smaller primary care practice, had previously worked
69
with a major retail pharmacy network to successfully reduce the number of duplicate faxes
but was unsure what exact fixes the pharmacy had applied or whether it would be applicable
to a practice the size of IMA.
As the provider of 30-40% of IMA's total prescription fulfillment, any improvement at
the primary retail pharmacy network could make a meaningful impact to overall practice
prescription volume. We contacted one major retail network to examine the issue further.
They have a centrally administered IT system but operational execution of prescriptions,
including renewals, is performed at the store level. They were very interested in determining
the source of duplicate faxes as this represents additional non-value-added work for their
stores.
Retail stores in this network will initiate a renewal request fax if a patient contacts them
for a refill and their current therapy has no remaining refills. In order for patients to have
continuous therapy, the pharmacy links new prescriptions to old ones. This linking processes
is performed manually at the store level. If a store fails to link the prescription, the new
prescription goes into a "Hold" status.
It is available to be activated when the patient
requests a refill but the pharmacy technician must locate and activate the held prescription;
it is often simpler for the pharmacy technician to request a renewal than to search for
a potentially held prescription.
The central office hypothesized that the stores were not
linking prescriptions and simply relying on renewal faxes.
In order to test this theory, the pharmacy network offered to take a list of IMA doctors,
identify all patients under those doctors using their pharmacies, then intervene with the
affected pharmacies to manually link all held prescriptions in their system. Since the central
office has no visibility into individual store actions with respect to fax requests, this had to
be a cooperative effort between the central office and IMA to provide sufficient visibility to
both sides of the process.
We provided a list of all attending doctors and related identifying information for IMA
Pods 2 & 3 to the central office and began monitoring the fraction of faxes from that pharinacy network that were labeled as duplicates, defined as no IMA action required because
an appropriate prescription had already been issued. During the control period ahead of the
linking implementation, the mean fraction of duplicate faxes was 23%. After the intervention
70
the mean duplicate fraction was 15%, a 35% reduction in duplicate fax volume suggesting a
significant shift in duplicate faxes (P-value < 0.05).
This retail pharmacy network plans to implement automated prescription linking across
their stores starting in mid-2014. We expect a comparable reduction in duplicate faxes from
this network for all IMA pods as this implementation rolls out, reducing total fax volume to
the practice by > 9000 faxes per year.
This pilot also shows that meaningful improvement in prescription request volume is
possible through better pharmacy coordination; under the prior IMA prescription workflow
this was effectively impossible, as such coordination would involve approximately 28 people,
none of whom had primary responsibility or accountability for the efficiency of the overall
process. By segmenting and centralizing the prescription group, the process of pharmacy
coordination is much simpler and we can reasonably expect comparable improvements from
all of the major pharmacy partners.
4.6.2
Voicemail Renewal Line Retirement
As discussed in Section 4.3.2, voicemails are a relatively low traffic and low yield request
process.
They also take significantly longer to process (mean 4m13s) compared to faxes
or web requests (mean 2m27s) due to having to transcribe data from the voicemail to the
renewal form at the speed of the patients' speech and constrained by the voicemail system
script. Staff and patients both expressed dissatisfaction with the voicemail system due to a
perceived difficult interface, time consuming input process, and frequent patient reports of
unfilled prescriptions.
Investigation of the issue through interviews and direct observations revealed the follow-
ing:
* Both pharmacies and the practice would prefer that patients directly contact the pharmacy, rather than the practice, when a renewal is required. As discussed in Section
4.3.4 and 4.6.1, the practice frequently receives renewal requests significantly before
the prior prescription has expired. If the pharmacy linking procedure is functioning
properly, the pharmacy can identify if a renewal is required and does not need to
71
contact the practice unless the current prescription has actually expired.
" Patients frequently do not have the information necessary to complete the prompts in
the voicemail script, resulting in incomplete voicemail messages or hangups.
" The voicemail system itself occasionally loses messages. A parallel research effort by a
Harvard Medical School student researched this issue by placing test messages at known
times into the system and then tracking whether they were picked up by the relevant
Medical Assistants.
Approximately 10% of messages were lost without explanation,
validating the patient claim of unfilled prescriptions. As of this writing, MGH telecom
services group is still attempting to identify the root cause of the missing messages.
" The prescription renewal lines use the term "refill" and "renewal" interchangeably
despite the fact that these clinically very different. A refill is a quantity of drugs to
be dispensed at a time; one prescription can authorize multiple refills. A renewal is
a new prescription. The practice hypothesized that this ambiguous terminology may
be leading patients to call the renewal line to leave a voicemail when they only need
a refill, which should require no action from the practice. Pharmacies identified that
they are aware of this ambiguity within the general patient population and this is one
of the reasons they prefer that patients contact the pharmacy first, rather than going
directly to the practice.
After extensive consultation with nurses, medical assistants, and the IMA operations
manager, a new voicemail script was developed to replace the existing script, making the
following changes:
* All references to "refill" are consistently changed to "renewal"
o Patients are encouraged to contact their pharmacy first, or use the web interface, and
only leave a voicemail if their request cannot be serviced by any other channel
* Patients are prompted with the information that will be required and given the opportunity to pause and collect the required data prior to recording their request
72
* The information prompts are condensed to require less button pushing by the patient
and speed up transcribing for the medical assistant
Once implemented, these changes are expected to reduce the volume of voicemail requests
(by shunting that traffic to the more efficient fax and web systems) and improve the yield of
the remaining voicemails (by improving the information contained in each message). As of
writing, the script is currently being implemented by MGH telecom services. A schematic
of the revised script is provided for reference in Appendix C.
The revised voicemail system will serve as a bridge; the ultimate goal is to retire the
voicemail system completely and send all calls directly to the Patient Service Coordinators,
where all other calls are currently handled today. The PSCs are in the best position to
interactively capture the required information and route it to the appropriate staff member
for action.
4.6.3
Prescription Renewal Workflow
As discussed in Section 4.5, centralizing prescription management provides benefits in terms
of reduced variability through pooling; and improved specialization and cycle times through
segmentation. However, centralization requires two significant changes from the current state
workflow shown in Figures 4-1 and 4-2:
Signature compliance: The current state workflow relies on nurses to issue the prescription to the pharmacy. However, only doctors and nurse practitioners are licensed to
issue prescriptions. IMA currently accommodates this requirement by having the doctor/NP cosign the medication note in the electronic medical record system but this
cosign can occur days or weeks after the prescription is issued. MGH has identified
that all primary care practices will need to transition to a process where a physician's
prescription order is provided before the prescription is sent to the pharmacy or patient.
Standard review: Under the current workflow, the degree of review performed by the
Medical Assistant and Nurse varies significantly from pod to pod and from provider to
provider. Each localized team has developed their own unique division of review tasks
73
with little coordination between pods. A central model must use a uniform process in
order to capture the benefits of centralization, so a standard review that is acceptable
to all providers must be included.
In order to accommodate these requirements the future state workflow (Figure 4-13)
includes a standard review, followed by clinical message to the provider for prescription
approval prior to releasing the prescription to the pharmacy. In order to prove that this
workflow was feasible, two pilots were conducted in the following manner:
1. Begin holding prescriptions from two pods at noon the day prior to the pilot, in order
to build an artificial backlog of prescriptions for processing
2. On the morning of the pilot, assemble a team of two medical assistants, two providers,
and an on-call nurse, each with a computer
3. Process the backlogged prescriptions using the medical assistants serving the role of
the central prescription group, the providers responding to the medical assistants via
clinical messaging, and the nurse providing clinical support to the medical assistants
as necessary
4. Record any discrepancies found during each prescription and update the draft standard
work document as necessary
The first pilot focused on non-controlled substances with a focus on determining the
appropriate level of detail required from the medical assistant review to enable the doctor
to quickly assess the appropriateness of the renewal request and rapidly respond. This pilot
demonstrated that clinical messaging could support the planned interaction and that the
existing standard review document was adequate to provide sufficient information to the
physician.
The second pilot focused on controlled substances and showed that the fundamental
workflow developed during the first pilot would also work for controlled substances. This
pilot also exposed several discrepancies in nuanced interpretation of the controlled substance
rules between the pods and weaknesses in the existing controlled-substance checklist; changes
were incorporated into the standard work and checklist to remedy these discrepancies.
74
The pilots demonstrate that the proposed workflow to support the central prescription
management group is practical and allows prescription processing at a comparable rate to
the current workflow. The pilots also serve as a powerful motivator for change within the
practice by putting a practical face on research that had, until this point, been primarily
theoretical and analytic.
75
THIS PAGE INTENTIONALLY LEFT BLANK
76
Chapter 5
Recommendations & Conclusions
5.1
Results
Based on the data, analysis, and modeling detailed in Chapter 3 & 4, we demonstrate that:
* The current state workflow is highly parallel and does not take advantage of IMAs
scale.
" The prescription flow can be modeled as a network flow problem to estimate the total
resources required to serve non-appointment prescriptions: 4.1 FTE. This result agrees
well with direct observation of practice operations.
* Pooling the prescription workflows between pods should reduce coefficient of variability
of daily demand from 0.49 to 0.19 based on 2012 prescription logs
" Pooling the prescription flows into a central prescription management group and segmenting this workflow from other practice operations will allow staff to develop stable, standard, dedicated workflows and begin to address chronic prescription issues:
spillover prescription requests, excess prescription requests, and non-actionable prescription requests.
" Coordination with pharmacies to properly link renewed prescriptions can reduce duplicate (non-actionable) fax renewal requests by > 35%.
77
"
Voicemail is a sub-optimal method of requesting renewals from the point of view of the
practice, pharmacies, and patients. Use of the voicemail system should be minimized
or eliminated; until it can be eliminated, revisions to the voicemail script to reduce
frequent patient errors can help increase voicemail yield.
" A centralized workflow where medical assistants perform a standardized review of each
prescription request, followed by provider confirmation via clinical messaging, is practical and effective.
As the central prescription group becomes established and stable, we expect the following
future state is attainable:
" Daily variability reduces > 50% due to pooling
" Fax yield increases to 87% due to improved prescription linking consistent with the
CVS pilot
" Voicemail renewal lines are closed
" 50% of excess and spillover prescriptions are eliminated due to dedicated employees
with a mandate to correct process errors
" Task time decreases 30% due to specialization enabled by segmentation
Under these assumptions, our model predicts that total resource use to serve non-appointment
prescriptions will drop from the current 4.1 FTE to 2.0-2.5 FTE, a 37% reduction. At the
same time, we expect improved patient care due to faster cycle times, less errors, and better
drug adherence.
5.2
Performance Metrics
Currently, none of the data sets or computations used to generate the metrics discussed in
Chapter 3 can be run continuously or in real-time due to IT system limitations. Prescription
and appointment logs can be run on an ad hoc basis at short (< 5 day) lead time, followed
by offline processing of the data to generate updated metrics. However, the PCOI patient
78
Table 5.1: Future state metrics
Current State
Target
Total FTE
4.1
4
Variability Per Day (Coefficient Of Variation)
0.6 (per pod)
4
Avg. Cycle Time [h:mm]
7:45
4
Non-actionable Requests
Excess Chronic & Stable
15%
8%
4
4
Spillover
4%
4
Metric
processing is run annually against a much larger third-party dataset, therefore any analysis
based on patient characteristics such as comorbidities or practice loyalty can only be run
after each calender year.
We propose rerunning the available metrics (volume, variability, spillover, excess chronic
& stable, and yield) after the first full month of operation of the central prescription group.
Relative to the current state, we expect the changes shown in Table 5.1.
As the practice does not currently track any prescription-related patient outcomes, there
are no defined patient outcome metrics.
There is opportunity for future research to tie
existing drug-related metrics, such as ED admissions or health-outcomes for drug-managed
conditions, back to prescription management processes.
5.3
Pooling & Segmentation
As is generally proven in the operations literature, pooling will lead to reduced variability.
Analysis of past data and modeling both show an expected 50% reduction in daily coefficient
of variation by pooling the full practice prescription traffic into a central group.
Segmenting this group's workflow away from other practice processes provides the opportunity to reduce interruption to patient-facing staff and allow dedicated prescription
management staff to specialize and standardize to a degree that is impossible under the
current workflow.
This process design also lays the foundation for any future change management with
respect to prescriptions, as it reduces the amount of coordination for any change from 28
79
people to 2.
5.4
Proactive Medicine Management
Prescription renewal is inherently predictable to a large extent; the current system functions entirely by patient-pull primarily because the practice does not have the resources or
processes to take advantage of the predictability inherent in the prescription data in the
electronic medical record.
We hope that, once the process improvements identified by this research are implemented,
the next step will be to experiment with proactive prescription management. As one simple
example, the algorithms developed during this research could generate a list of patients
expected to have a prescription renewal for particular drugs in any given time period (e.g. the
coming week). A central prescription management group could then proactively issue those
prescriptions and notify the patient, rather than waiting for patient contact and potentially
missing a drug non-adherence.
Once the capabilities are in place to proactively identify what patients should receive
which prescriptions when, and a dedicated staff is available to enact such policies, many
exciting options become available for future improvements in prescription management.
5.5
Future Work
In addition to implementation and monitoring of the recommended prescription management
system, the data analysis and observations inform several possible productive avenues of
future research:
5.5.1
Scheduling
Rescheduling
A significant number of PSC activities involve scheduling and rescheduling appointments.
Approximately 40% of booked appointments never arrive and the recovery rate (ability to
80
re-fill a canceled slot) is low.
In theory, the schedule system provides tools to manage
recovery rate via the waitlist function but observations showed that this function is rarely
employed by the PSCs due to perceived lack of utility and user-unfriendliness of the IDX
implementation. Interventions that can improve schedule utilization would lower the PSC
workload and improve patient access by opening up provider schedules.
Appointment Duration
The average appointment is both delayed and overrun (see Section 3.5.1 for details). Observations showed poor correspondence between the schedule and actual appointment time,
with predictable trends based on provider and patient. In virtually all cases, when asked,
providers could correctly predict which patients would overrun. This suggests the possibility
for a predictive model to better match appointment duration to patient needs.
5.5.2
Capacity Planning
Adjustment For Patient Complexity
There is a significant discrepancy between medical complexity (current computed by Risk
Adjusted Panel Score) compared to "patient complexity" (how much effort and intensity is
required by the provider to treat the patient). As a result, practice resources allocated based
purely on medical complexity (e.g. case managers) may not correspond well to the actual
practice resources required to care for the patient. A medically complex patient might be
straightforward if they are also very proactive in their care, while a medically simple patient
with significant psycho-social needs may take up significant practice resources for both their
visits and intravisit care.
Capacity Analysis - Panels
IMA has been asked to increase panel sizes while most attendings have closed panels. There
is currently no model to allocate new patients or to take account of the various metrics of
patient complexity or current resource utilization. IMA will require a mechanism to allocate
new patients that optimally balances available practice capacity.
81
Capacity Analysis - Support Staff
Observations show a consistent sentiment within pods that they are either under- or (rarely)
over-staffed with respect to various support roles. Quantitative data supports this sentiment.
For example, preliminary staffing ratio analysis shows that, although the overall provider to
medical assistant ratio is approximately 1.0-1.75 (depending on the session), the range within
any particular pod can be 0.0-3.0. This is supported by the role observations, where MAs
sometimes had no providers on session and at other times had three. There appears to be a
significant opportunity to alter the MA:provider mapping (either through provider schedule
changes or MA reassignment) to level out the support ratio.
82
Appendix A
Role Observation Form
83
o Preceptor
o Attending
o Nurse Practitioner
" Nurse. o Medical Assistant
o Patient Service Coordinator
Other
" Resident
o
start iime
Location:
btaTT rresent:
Activity:
WR ER Lab Desk
MD R NP RN MA PSC Oth
Visit: Pre Treat Post Oth
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
I
ITOther
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
MD R NP RN MA PSC Oth
MD R NP RN MA PSC Oth
MD R NP RN MA PSC Oth
MD R NP RN MA PSC 0th
MD R NP RN MA PSC Oth
MD R NP RN MA PSC
Oth
Oth
MD R NP RN MA PSC Oth
MD R NP RN MA PSC
MD R NP RN MA PSC Oth
MD R NP RN MA PSC
Oth
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
_______RNP
_NMA_______
Oth
MD R NP RN MA PSC Oth
MD R NP RN MA PSC
MD R NP RN MA PSC
Oth
WR ER Lab Desk
IT Other
MD R NP RN MA PSC
Oth
WR ER Lab Desk
MD R NP RN MA PSC Oth
ITOther
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR ER Lab Desk
IT Other
WR
ER Lab Desk
WR ER Lab Desk
ITOther
Visit: Pre Treat Post Oth
Oth
Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PMV Intra Admn Oth
Visit: Pre Treat Post Oth
Non-Visit: PM intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
WR ER Lab Desk
ITOther
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm
IT Other
WR ER Lab Desk
Notes:
Non-Visit: PM Intra Adm
MD R NP RN MA PSC Oth
Pod:
Name:
FTE:
MD R NP RN MA PSC
Oth
MD R NP RN MA PSC
Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm
MD R NP RN MA PSC Oth
Visit: Pre Treat Post Oth
MD R NP RN MA PSC Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm
MD R NP RN MA PSC Oth
MD R NP RN MA PSC
Oth
MD R NP RN MA PSC Oth
MD R NP RN MA PSC Oth
MD R NP RN MA PSC
Oth
Oth
MD R NP RN MA PSC Oth
MD R NP RN MA PSC
VD R NIPRN MAPSC Oth
M__RNPRNMAPC___h
Property of MGH
IMA -
Oth
Oth
Oth
Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM Intra Adm Oth
Visit: Pre Treat Post Oth
Non-Visit: PM intra Adm Oth
Visit: Pre Treat Post Oth
PM Intra
Non-Visit:
Post Adm
0th Oth
Visit:
Pro Treat
Visit: Pre Treat Post 0th
Non-Visit: PM Intra Adm
Oth
Page
DO NOT RECORD P/PHI ON THIS FORM - Apply PHI controls
Figure A-1: Role observation form, page 1
84
of
Time Info:
Date: The date of the observation
Block: Whether this is a morning or afternoon block (circle one)
Seeing Pts?: Whether the role is scheduled to be seeing patients during this block (circle one)
Role Info:
Preceptor: An attending working on supervising residents (this does not include an attending seeing their own patients)
Attending: An attending working on their own patients
Pod: The hemipod where the person is working (i.e. if in "2" put "2", not "2/3")
Name: The person's name (First Initial. Last Name)
FTE: The amount of Full-Time-Equivalent that the person typically works (can be obtained from Arlene if unknown)
Observations:
Start Time - The starting time (hh Imm ss) for that line. No end time is needed (it's the start time of the next line).
Location - Where, physically, the person is (circle one):
WR: Waiting Room
ER: Exam Room (record which in the notes)
Lab: Blood or EKG lab (record which in the notes)
Desk: The person's normal workspace (office/MA desk/etc.)
IT: In Transit (moving from one location to another)
Other: Anything else (record where in the notes)
Staff Present - All practice members present with the person being o bserved (circle as many as needed).
If multiple of one role, put a number by the role:
MD: Attending
R: Resident (if an MD is present and NOT the preceptor, put that in the notes)
NP: Nurse Practitioner
RN: Nurse
MA: Medical Assistant
PSC: Patient Service Coordinator
Oth: Other (record who in the notes). Do not record people who came with the patient (family members, etc.)
Activity - What the person is doing:
Visit: Work associated with a specific billable/scheduled visit (past, present, or future)
Pre: Work to prepare for the patients' visit
Treat: Working with a patient
Post: Work to follow-up on patients' visits that already occurred
Oth: Anything else related to a particular visit (record in the notes)
Non-visit: Work not associated with a specific billable/scheduled visit
PM: Population management (as defined by IMA role documents) - when in doubt, ask
Intra: Care for patients not directly tied to a visit (letters, emails, calls, consultations, perscriptions, etc.)
Adm: Administrative work not related to any patient or population need
Oth: Anything else
Notes - Free text to elaborate on anything
Any time any of the observation fields change, you should start a new line. The time difference is then the duration for
the prior line.
Figure A-2: Role observation form, page 2
85
THIS PAGE INTENTIONALLY LEFT BLANK
86
Appendix B
Patient Observation Form
87
Start Time
Location:
Staff Present:
WR Vitals ER
I Lab thsE
WR
MD
MD RR NP
NP RN
RN MA
MA PSC
PSC Oth
0th
Wait
Wait Treat
Treat Adm Oth
0th
IT Labth
MD R NP RN MA PSC 0th
Wait Treat Adm 0th
WR Vitals ER
MD R NP RN MA
Wait Treat Adm
o'""Othe
Wait Treat Adm Oth
Wait Treat Adm 0th
Wait Treat Adm Oth
Walt TreatAdmoth
Wait Treat Adm Oth
WaIt Treat Adm 0th
WaIt Treat Adm Oth
Walt Treat Adm 0th
Wait Treat Adm Oth
Wait Treat Adm 0th
WaIt Treat Adm Oth
Wait Treat Adm 0th
WaIt Treat Adm Oth
Walt Treat Adm 0th
Wait Treat Adm Oth
Wait Treat Adm 0th
WaIt Treat Adm Oth
Walt Treat Adm 0th
Wait Treat Adm Oth
Wait Treat Admn Oth
MD R NP RN MA PSC Oth
MD R NP RN MA PSC Oth
Wait Treat Ad
Wait Treat Adm
WR Vitals ER
MD R NP RN MA PSC Oth
Wait Treat Adm Oth
WR Vitas ER
MD R NP RN MA PSC Oth
Walt Treat Adm
Oth
WR Vita s ER
MD R NP RN MA PSC Oth
Wait Treat Adm
Oth
Mit 0tIMA
IT RLab0t
Vit
MD R NP RN MA PSC 0th
MD R NP RN MA PSC 0th
F
Wait Treat Ad
Wait Treat Ad m 0th
WR Vitals ER
IT Lab Oth
WR Vitals ER
IT Lab Oth
WR Vitals ER
MIRNPRMAPCOh
MRNRMPCt
MDRN
NM
S
t
MRNRMPCt
II
PR
APCOh
WiTraAdn t
Watrtdmt
IT Lab0t
R Vit
MD R NP RN MA PSC 0th
Walt Treat Admn 0th
itabs
0th
MD IR NP RN MA PSC 0th
Wait Treat Admr 0th
R Vitabs
0th
MID R NP RN MA PSC 0th
Wait Treat Ad~m 0th
MID R NP RN MA PSC 0th
WalIt Treat Adm 0nth
MD R NP RN MA PSC 0th
Wait Treat Adm 0nth
I Vabs
0th
WIR Vitals ER
VDRNRNM
R Vitas
0th
S
t
MID R NP RN MA PSC 0th
IT Lab Oth
IDNRMPCt
WR Vitals ER
MDRN
NM S
t
MRNRMPCt
ITTLab Oth
Property of MGH IMA
oth
Oth
Ath
aI ra dr t
Watradmh
Wi
ra
dr
t
aITrtAdnOh
Wa It Treat Admn 0th
WaIra~mt
aI ra dr t
Watrtdmt
UPage
-
MD R NP RN
Oth
Wait Treat Adm 0th
IT Lab0t
R Vit
"
Pod:
Name:
Type:
Notes:
MD R NP RN MA PSC Oth
MD R NP RN MA PSC 0th
MI R NP RN MA PSC Oth
MDRNPRN MAPSCOth
MD R NP RN MA PSC Oth
MD R NP RN MA PSC 0th
MD R NP RN MA PSC Oth
MD R NP RN MA PSC 0th
MD R NP RN MA PSC Oth
MD R NP RN MA PSC 0th
MD R NP RN MA PSC Oth
MD R NP RN MA PSC 0th
MD R NP RN MA PSC Oth
MD R NP RN MA PSC 0th
MD R NP RN MA PSC Oth
MD R NP RN MA PSC 0th
MD R NP RN MA PSC Oth
MD R NP RN MA PSC 0th
MD
NP RN
MA PSC
MID R
R NP
RN MA
PSC Oth
Oth
WI
I
I
Oth
o Follow-up ci
WR Vitals ER
R VIT
ab E
WR Vitals ER
I
II
PSC
N
MD R NP RN MA PSC 0th
ITIE
II
II
Y
RIVIT
ab E
WR Vitals ER
R VIT
a 0th
WR Vita s ER
R VIT
a0th
WR Vita s ER
ER
IT a
WR Vitals ER
IT Lab 0th
WR Vitals ER
E
ITa
WR Vitals ER
VIT s ER
WR Vitals ER
IT
sER
WR Vita
WR
Vitalss ER
ER
RVITLab Oth
WR Vitals ER
WR Vitals E R
rpr
oAwvInjection
oB''
o New Pt. o Reassign
"3Annuai
Dat:
Appt. Time:
Sch. Duration.
Activity:
Patcomn #:
Notified of wait time?
of
DO NOT RECORD P1/PHI ON THIS FORM - Apply PHI controls
Figure B-1: Patient observation form, page 1
88
Pt Info:
Patcom #: Unique identifier for each appointment in IDX. Available from the PSC and on the schedule report. Also
recoverable after observation using provider name/time.
Notified of wait time?: Was the patient notified by a member of the practice (typically the MA) of the expected wait
time? This is follow-up tracking for a prior IMA time study.
Time Info:
Date: The date the observation is made
Appt. Time: The scheduled time of the appointment
Sch. Duration: The scheduled duration of the appointment
Appt. Info:
Tick off the type of the appointment that was scheduled (available from the PSC). If the content of the appointment
changes, that will be captured in the observation notes.
Provider Info:
Pod: The number of the hemipod (e.g. if you're in 2 put "2", not "2/3")
Name: The provider's name (First Initial. Last Name)
Type (circle one) -The type of provider that was scheduled:
MD: Attending
R: Resident
NP: Nurse Practiotioner
RN: Nurse
Observations:
Start Time - The starting time (hhlmmss) for that line. No end time is needed (it's the start time of the next line).
Location - Where, physically, the patient is (circle one):
WR: Waiting Room (includes the PSC desk)
Vitals: The vital signs measurement area (in the back hallway for most pods)
ER: Exam Room (record which in the notes)
IT: In Transit (moving from one location to another)
Lab: Blood or EKG lab (record which in the notes)
Oth: Anything else (record where in the notes)
Staff Present - All practice members present with the patient (circle as many as needed). If multiple of one role, write
the number beside the circle and capture that in the notes:
MD: Attending
R: Resident (if an MD is present and NOTthe preceptor, put that in the notes)
NP: Nurse Practitioner
RN: Nurse
MA: Medical Assistant
PSC: Patient Service Coordinator
Oth: Other (record who in the notes). Do not record people who came with the patient (family members, etc.)
Activity - What the patient is doing:
Wait: Waiting (i.e. not interacting with any member of the practice)
Treat: Receiving treatment (physical or verbal) from any member of the practice
Adm: Administrative work (appointment scheduling, pre- or post-visit paperwork, insurance, copay, etc.)
Oth: Anything else (record in the notes)
Notes - Free text to elaborate on anything
Any time any of the observation fields change, you should start a new line. The time difference is then the duration for
the prior line.
Figure B-2: Patient observation form, page 2
89
THIS PAGE INTENTIONALLY LEFT BLANK
90
Appendix C
Revised Renewal Line Voicemail
Script
91
Cal Refil Line
a
reached the
51rucrure
al the opi-
You hawe
Ms sachuses General Hospital
Intemal Medicine Associat ix medication ref voicemalas of[DATE]: please lisen to
This is new menu
to obtain
We've found haithe faste vtway tor you
your
medication refil isfor you to cal your phanacy directly. It
needed, your pharmacy il contact us to ensure orste
medications are ready for you.
on t Inie.
and
I you cannot reach your p harnacy, you can also quic*
request a medicaui on reil n the web at
wwwiheahispace.org. It Du have not yet signed up for
p*es- press I for more information or stay
NHeallhspace,
number,also
before
to e
old
do not have
you
it cannot contact you r pharmacy
access to ifiealtspace, yo .al need your MG4 medical
known as your blue card numbeir and your
'ou leave a messae. Please
prescription ready
ive a meaM.a
press 2
insoucoons for ie althspace enrolmet
We
your
wil
hours.
refil within 48
medication
process
iHeahspace enroliment instructions, press 1.
reil by voicemal, press 2.
odbye.
for caling ieemal Medicine Associales.
To request your
To repeat the
Thank you
Press 2
1
P-axe]
press
-Pes2your
[P-1
inorder to complete your refil,
me
of
flW-*d
Prss #
#
Pase]
{Pause]
Press
key.
I
the
Press
will need your: MGHt medical record
number, name. dale of birth, name
of your pharmacy. and medication
when you are ready
to proceed, please press p.
your MG
medical record number,
folowed by the #xkey.
Record
#
state your name
folowed by the
R cP-d
the
voice
Record
name
Please state
pharmacy,
by # key.
Pre.cI
frs
[Paus1
being refiled
thw #
the name of
need
key.
Please state
the
medicAti you
refiled, toddowed by
Record
TIMELINE
Nov 1-15: Finalize draft script wi stakeholders
Nov 18-22: Approval from practice management
Nov 25-29: Develop test mailbox
Dec 2-6: Trial test mailbox & iterate script
Dec 10: Go-live approval
Dec 1113: Train affected podmembers
Dec 16: Switchover Pod 7/8 refil line
04
I-I
UD
C1'
Appendix D
Additional Time Study Observations
" All roles stay on task for the vast majority of the day. Items such as personal discussions, bathroom trips, coffee breaks, etc. were categorized as NV-Oth, which combines
with several other items and so is not immediately visible in the quantitative data.
However, all observers noted some surprise at the very low level of non-work activity
compared to other organizations they have seen. There may be an element of bias, in
that people being observed may alter their work habits due to the presence of the observer, but in no cases did the observers perceive any obvious examples of substantially
altered workflow or behavior.
" The level of patient care not attributable to a visit (and hence not reimbursed under
most current insurance plans) was surprisingly high. As IMA transitions to a PCMH
model with capitated reimbursement this will become less of an issue but, during the
transition period, the mismatch between resource expenditure and practice income
may exacerbate discussions around appropriate panel sizes, billing, and provider compensation.
* The level of observed cross-pod interaction was very low. Most roles interact with other
roles within their own pod several times a day but have very few, if any, interaction
with IMA staff from other pods. Several current initiatives should help address this
but the level of day-to-day knowledge sharing at the tactical level seemed very low.
" Each pod as its own "personality", reflected in the cultural norms of each pod and
93
their perception of their own status relative to other pods. This is not inherently bad
or good, and likely serves as a powerful way to build connections with an organization
the size of IMA, but does present change implementation challenges as each pod views
their own needs, workflows, and strengths differently from each other.
" In many cases, the observers saw many different members of the practice struggle with
small IT problems that generated considerable rework and confusion:
non-working
printers, QuickSilver clinical messaging lockup, CRMS referral system's inability to
save partial work, and inability for particular workstations to login to IDX scheduling.
The team also observed many different deployments of the same function for different
purposes (notably use of QuickSilver) and the use of different functions for the same
purpose (email vs. QuickSilver vs. greensheets vs. mailboxes). This problem became
more acute with cross-pod interactions or staff members floating between pods because
of the lack of consistent use of tools.
" Huddle conduct was very inconsistent across pods and providers.
Some teams did
not conduct a huddle at all, some had a very perfunctory meeting with only some
of the recommended roles present, and some had everyone and were very thorough.
The location also varied, with some huddles conducted in the MA area "in the middle
of things" with others conducted behind a closed door in the provider's office. More
thorough huddles appeared to correlate with pods and teams that the practice deemed
as "higher performing" but this study did not determine whether this was a causative
or correlative relationship.
" Many roles and pods have no structured plan for breaks, including lunch. In some
cases where there is only one person present (e.g. nurses), the only observed solutions
either disrupt the pod workflow or drive the staff member to eat lunch on the fly.
Even in pods where there are multiple staff for the same role, the workload jump going
from two to one staff is significant and resulted in large phone backlogs in at least two
observed occasions.
* It is difficult to have conversations in the front office that are not audible to patients
94
at the desk talking to the coordinators. There were no observations of this causing any
problem or noticeable patient discomfort but may present HIPAA concerns.
* A large portion of non-appointment patient contact takes place through the phone.
Although some email and iHealthspace web messaging was observed for all roles, it
was a small fraction relative to requests by phone. This was a source of consistent and
unpredictable interruption for everyone observed.
Several staff members with work
history at other practices commented that IMA handled an unusually high volume of
interaction via phone.
" There is low consistency of assignment of tasks to roles. The same task may be done by
a coordinator, a medical assistant, or a nurse depending on the pod and provider. In
several cases, there were locally designed "custom" workflows to support one particular
provider. Although sometimes effective at the local level, this caused difficulty during
staff substitutions.
95
THIS PAGE INTENTIONALLY LEFT BLANK
96
Appendix E
Network Flow Model Screenshots
97
_______________
Population
Total Patients
Variable
Patient
%On Meds
Rx Per Pt Per Year
Daily SD
Mean
I
Definition
OnCall rx
OnCall rx log, 2010-2012
lot 2020-2012
Source
RxDailySD
TotaPts
PctMeds
RxPerPt
Nama
- r
Uoh
OnCall rx log daily SD, excluding holidays/Sat/Sun
Inf
-
each
%
rx/pt
Unique MRNs per year
Fraction of "Total Patients" with at least one prescription
Average number of prescriptions per patient that has a prescription
Standard deviation of daily practice Rx demand, excluding holidays/Saturday/Sunday
IMA layout: la, 1b, 1c, 2, 3, 4a, 4b, 4c, 5, 6, 7, 8, 9, 10
N/A
N/A
Hours per week per FTE
Day per week when prescriptions are processed
Duration to calculate traffic over the network
Must be bigger than the largest value on any arc
_______________________________________________
rx/day
Number of Independent prescription processing streams
Number of weeks per year
Number of total days per year
Number of working hours per week per FTE
Number of workdays per week per FTE
Length of time for the model to span (normally 1 year 36S days)
Constant for use in the solver no physical meaning
ApptYield
Assumed, wIll be updated based on spillage estimate
Frequency that a prescriptions requested at an appointment can become a prescription
WebYleld
iHeaothspace log of refused/total requests, 2010-2012
Frequency that an lHealthspace request becomes a successful prescription
VmailYield
Pod 1/2/7/8 observation, Sep 30-lct 7
Frequency that a voicemafl request becomes a successful prescription
FaxYeld
Pod 2/3 observations, pre-CVS intervention
Frequency that a fax request becomes a successful prescription
ExcessRenewal
Average prescriptions per patient per year for chronic, stable dose meds (antihypertensive, antilipt OnCall prescription log with processing
ExcessTarget
Value of "Excess Renewals" with a perfect system
Target prescriptions per patient per year for chronic, stable dose meds
StableRxPct
OnCall prescription log with processing
Fraction of all prescriptions that are chomic and stable In the "Excess Renewals" calculation
Assumption: Fraction ofexcess renewals that can be eliminate ExcessYield
Fraction of excess renewals that are caught by improved patient Intevention
SptlPct
From OnCall/lDX log processing (2-dayspilil)
Fraction ofprescriptions that land within 2 days of a scheduled appointment
Assumption: Fraction of spilled prescriptions that can be shift. SpllYield
Fraction ofspilled renewals that could be done at the appointment with improved processes
RxVmaflPct
RxWebPct
RxApptPct
WksPerYear
DaysPerYear
WorkWeek
WkDaysWeek
Duration
NumPods
each
weeks
days
hours
days
days
N/A
%
Request Channels
Constants
Number Of Pods
Weeks Per Yer
Days Par Year
WorkWeek
Work Days Per Week
Duration
"Infiniy"
RxFaxPct
%t
Prescription
OnCall prescription log processed against IDX log
OnCall prescription log & IlHealthspace log
Based on observed .125/.875 split vmail/fax
Based on observed .125/.875 split vmail/fax
%Rx By Apprk
" By By Web
" Rx By Vmall
%
%
Fraction of all prescriptions currently Issued on a day with an arrived appointment
Fraction of all prescriptions issued via iHeakthspace
Fraction of all prescriptions issued in response to a voicemafl on the renewal line
Fraction of all prescriptions issued in response to a fax
% Rx By Fax
Appt Yield
Web Yleld
Vmal Yield
Ideal
Fax Yield
Excess Renewels
Excess
Chronic & Stable %
Excess Yield
SpIN %
spil Yield
b
n
a
bD
.-
Cn
--
bO
CI
-4-
L~
oc
0agistIc Regression - Arrivals in Time
Monday
Tuesday
Wednesday
Thursday
Friday
Saturday
Sunday
Task Times
Fax Split
Fax Saub
Vmail Scrub
Web Scrub
Admin Calibration
Clinical Scrub
Clinical Calibration
Walt Times
Appt
Web
VM81a
Fax
Central Staffing
Admin
Clinical
Prescriber
Interventions
Centralized Pods
Centraled Cinical
Saved
Spedallzatioen
Prooss
FTE
Cyde
Time
Baseline Values
nm:ss.s
nm:sszs
nm:ss.s
nm:ss.s
nm:ss.s
received on Monday
received on Tuesday
received on Wednesday
received on Thursday
received on Friday
received on Saturday
receied on Sunday
Logistic regression fit in JMP - RxDemandtyDay_2010-2012_pv PctMon
PctTue
PctWed
PctThu
PctFr
Pctsat
PctSun
of requests
ofrequests
of requests
ofrequests
of requests
of requests
of requests
Fraction
Fraction
Fraction
Fraction
Fraction
Fraction
Fraction
Pod 1 observations, Sep 30-Oct 7
PTFaxSplit
Pod 2/4ab/3/7 observations, Oct 7-Nov 1
PTFaxScrub
Pod 1/3/4ab/7 observations, Sep 30-Oct 9
PTVmailScrub
PT WebScrub
Assumed equal to fax scrub due to equivalent information
Calibration factor for admin time, If needed (1 =no calibration PTAdmnCal
PTClinicalScrub
Pod 214b/10 observations, Nov 8-11
Calibration factor for clinical time if needed (1 =no calibration PTClinicalCal
CtriPods
CtrIClinical
PctSpecllzed
CtriClinical
CtrIPresc
CtrfIAdmin
FaxWat
VmalWait
Assumed to equal average appointment time
ApptWaft
Simulation - IMADualPodCurrentState_2013111 WebWat
MedModel
Future state variabie - to be determined
Future state variable - to be determined
Future state variable - to be determined
requested at an appointment
requested at an appointment
requested at an appointment
requested at an appointment
Headcount for central processing- administrative scrub
central processing- clinical scrub
central processing - prescription authorization
a prescription
a prescription
a prescription
a prescription
Average time to distribute one fax to the appropriate person for scrub
Average time to do administrative scrub of one fax
Average time to do administrative scrub of one vmail
Average time to do administrative scrub of one liealthspace request (assumed equal to fax)
Model calibration factor. 1 = no change from observations
Average time to do clinical scrub of one prescription request
Model calibration factor. 1 = no change from observations
Average cycle time for
Average cycle time for
Average cycle time for
Average cyde time for
,h:mm
ih:mm
ih:mm
Headcountfor
Future state variable - to be determined
1
Headcount
na
for
Number of pods to feedinto the central proscription processing
ih:mm
!a
!a
a
Central clinical control. S = no central clinical proces.
Reduction in process time due to specialization
Reduction in process time due to changed workflow
staff
Flag. = centrm clinical scrub, 0 = central admin scrub only
Expected reduction in process time due to specialization of central
Expected reduction in process time due to improved workfiow
nm:ss.s
Ior
6
Calculated for 2012 Input data - baseline for savings
Calculated for 2012 input data - baseline for savings
with existing
Total FTE required in 2012 with existing workflow - reference for comparisson of other options
cycle time in 2012
workflow - reference for comparisson of other options
Average
Q)
C\1
0
Cd
r14
-D
CO.
Z0
UO
Total
183474
14166
7782
0
Fax
Appt
Web
Vmail
1524
0
1084.16
11559
750411
183475
IISS9
91554
5697
16442
101407
215100
Issued
Pre-Spill Spill Recovery ITotal
91554
91554
5321
5321
75041
183475
rx2/day
rx2/day
rx2/day
Requests
Pods
5697
16442
101407
123546
Central
Mean
Total
Per Pod
Central
376
4883
26366
316251
ITotal
0
01
0
0
A
13105.36
137
0:02:41 Average process time for a waste prescription [weighted average of individual process times]
Prescription Output
Total Issued
Chronic Excess Rx
Spilled Rx (2-day)
Excess Rx Diverted
Spilled Rx Diverted
Process Times
Variance
All - Per Day
Per Pod
Central
a
0
01
Central
3761
48831
01
0
0.032
CoV
263661
3162Sf
Waste
Pods
rx
rx
0
1.4
-4-D
10z
Froma'
naa
AA
'iji
n
Figure E-4: Screenshot
-
network adjacency matrix
101
0
From
5"*
-4M
00a
0~0
I-IM
4-
0
-4
0
t,
0
00
-4
t.n
0
0
Figure E-5: Screenshot
-
decision variables (current state)
102
0
0 0Conservation
Justification
Sign Const.
Delta
In
0 Source node
7782
-215100 <=
Conservation
99336.09
Conservation
5697
Conservation
16442
101407
Conservation
Conservation
16442
101407
Conservation
Conservation
5697
Conservation
11559
Conservation
75041
Sink node: complete prescriptions
183475
0 Sink node: redundant prescriptions
31625
31625 >=
0
Conservation
Conservation
Network Constraints
Out
222882.1
99336.09
5697
16442
101407
16442
101407
5697
11559
75041
0
0
0
0
U
0
a
C-6
;-a)D
Path Constraints
Value
Sign Const.
Justification
Match RxAtAppt to logs
Match RxFromWeb to logs
Match RxFromVmail to logs
Match RxFromFax to logs
Central process - Web
Central process - Vmail
Central process - Fax
Prescriptions diverted due to excess reduction
Prescriptions diverted due to spillage
Waste -Web
Waste -Vmail
Waste - Fax
Waste prescription from central processing
Force centralized clinical processing if enabled
0
0
)
Cl)
S-4
b-
Ouputs
Should match to input, within rounding error, to verify model integrity
hould match to input, within rounding error, to verify model integrity
91921 Prescriptionsissued outside appointments (not on a day with an arrivedappointment)
91554 Prescriptions issued at appointments (on a day with on arrivedappointment)
215100 Estimate of number of requestsfor prescriptions
31625 Estimate of number of requests that do not result in a prescription (duplicates, incomplete info, wrong patient, etc.)
14166 Estimate of number of requests that were not clinicallynecessary
7.7% Estimate offraction of prescriptions issued that were not clinically necessary
7782 Number of prescriptions that could have been handled at the appointment (2-day window) but were not
25 Mean daily prescription request demand, each pod
0 Mean daily prescription request demand, central team
353 Mean daily prescription request demand, total practice
0.655 Standard Deviation/mean prescription demand per pod
0.000 Standard Deviation/mean prescription demandfor centralized processing (depends on # of centralized pods)
0.175 Standard Deviation/mean prescription demandforfull practice (equivalent to complete centralization)
Per Pod
Central
All Practice
414
42 Mean + 1SD daily prescription request demand, each pod
0 Mean +1SD daily prescription request demand, central team
Mean +1SD daily prescription request demand, total practice
Per Pod
Central
All Practice
58 Mean +2SD daily prescription request demand, each pod
0 Mean +25 Ddaily prescription request demand, central team
476 Mean +2SD daily prescription request demand, total practice
Per Pod
Central
All Practice
Total # Of Prescriptions
Total Patients w/ Prescriptions
Non-appointment Prescriptions
Appointment Prescriptions
Prescription Requests
Waste Requests
Excess Requests
Excess Renewal %
Spillover Prescriptions
Prescription Volume CoV
Daily Load
+1 SD [84%}
+2 SD [98%]
Per Pod
Central
All Practice
b-4
a)
C)
Q)
$A
6-4
7:4S
0
0
Average prescription cycle time fhh:mm], including both processing and wait time
Total hours of processing time saved due to process redesign
Total FTE saved due to specialization
Total FTE requiredfor the complete practice (individual & centralized pods)
0:00 Average cycle time reduction
4.07
4.1 Total FTE requiredfor the complete practice on an average demand day
Total FTE requiredfor an individual pod on an average demand day
Total FTE requiredfor the central team on an average demand day
0.3
0.0
0.5
0.0
4.8 Total FTE requiredfor the complete practice on an average + 1 SD demand day
Total FTE requiredfor an individual pod on an average + I SD demand day
Total FTE requiredfor the central team an an average +1 SD demand day
All Practice
Per Pod
Central
5.5 Total FTE requiredfor the complete practice on an average +2 SD demand day
0.7 Total FTE requiredfor an individual pod on an average + 2 SD demand day
0.0 Total FTE requiredfor the central team on an average + 2 SD demand day
0.2 Total FTE (aveage demand day) per role
2.5
1.3
0.0
0.0
00,
0.0 1
0.01,
9.1%
1.7% Average utilization per role
18.2%"
Prescriber
Clinical
PSC
MA
RN
MD/NP
none
Admin
All Practice
PerPod
Central
All Practice
Per Pod
Central
Average Cycle Time
Process Redesign Time Saved
Specialization Time Saved
Cycle Time Saved
Total FTE
Daily Avg
+1 SD [84%I
+2 SD 198%]
By role
Utilitzation
RN
0.0%
0.0%
0.0%"
0.0%
0.0%1.
PSC
MA
MD/NP
none
Admin
Clinical
Prescriber
(1)
ce7
C.)
A-D
0
0
14
(3)
CI)
af)
-4
44
-
Bibliography
[1] Hospital overview - massachusetts general hospital. http://www.massgeneral.org/
about/overview.aspx, February 2014. [Online; accessed 06-Feb-2014].
[2] Massachusetts general hospital primary care home. http://www.massgeneral.org/
primarycare/, February 2014. [Online; accessed 06-Feb-2014].
[3] Richard Adair, Jon Christianson, Douglas R. Wholey, Katie White, Robert Town, Suhna
Lee, Heather Britt, Peter Lund, Anya Lukasewycz, and Deborah Elumba. Care guides:
Employing nonclinical laypersons to help primary care teams manage chronic disease.
Journal of Ambulatory Care Management, 35(1):27-37, 2012.
[4] Richard Adair, Douglas R. Wholey, Jon Christianson, Katie M. White, Heather Britt,
and Suhna Lee. Improving chronic disease care by adding laypersons to the primary
care TeamA parallel randomized trial. Annals of Internal Medicine, 159(3):176-184,
August 2013.
[5] Murray Aitken and Silvia Valkova. Avoidable costs in US healthcare. Technical report,
IMS Institute For Healthcare Informatics, June 2013.
[6] Anthony J. Avery, Sarah Rodgers, Judith A. Cantrill, Sarah Armstrong, Kathrin Cresswell, Martin Eden, Rachel A. Elliott, Rachel Howard, Denise Kendrick, Caroline J.
Morris, Robin J. Prescott, Glen Swanwick, Matthew Franklin, Koen Putman, Matthew
Boyd, and Aziz Sheikh. A pharmacist-led information technology intervention for medication errors (PINCER): a multicentre, cluster randomised, controlled trial and cost-
effectiveness analysis. Lancet, 379(9823):1310-1319, April 2012.
[7] H Backer and S Mackell. Potential cost-savings and quality improvement in travel advice
for children and families from a centralized travel medicine clinic in a large group-model
health maintenance organization. Journal of travel medicine, 8(5):247--253, October
2001. PMID: 11703907.
[8] John W Bennett, Paul Glasziou, Christopher Del Mar, and Frederick De Looze. A
computerised prescribing decision support system to improve patient adherence with
prescribing. a randomised controlled trial. Australian family physician, 32(8):667-671,
August 2003. PMID: 12973881.
[9] Thomas Bodenheimer, Edward H. Wagner, and Kevin Grumback. Improving primary
care for patients with chronic illness. Journal Of The American Medical Association,
288(15):1909-1914, October 2002.
107
[10] A.d. Brown and A.m. Garber. Cost effectiveness of coronary heart disease prevention
strategies in adults. PharmacoEconomics,14(1):27-48, July 1998.
[11] Marie T. Brown and Christine A. Sinsky. MEDICATION ADHERENCE: we didn't ask
and they didn't tell. Family Practice Management, April 2013.
[12] Asa Carlsson, Fredrik Borgstrom, Jan Stalhammar, Evo Alemao, Don Yin, and Linus
Jonnsson. Cost of care for patients treated with lipid-lowering drugs. PharmacoEconomics, 22:25-35, March 2004.
[13] Niteesh K. Choudhry, Michael A. Fischer, Jerry Avorn, Joshua N. Liberman, Sebastian
Schneeweiss, Juliana Pakes, Troyen A. Brennan, and William H. Shrank. The implications of therapeutic complexity on adherence to cardiovascular medications. Archives
of Internal Medicine, 171(9), May 2011.
[14] Benjamin A. Christensen, School of Management Sloan, Institute of Technology Massachusetts, and for Global Operations Program Leaders. Improving ICU patient flow
through discrete-event simulation. 2012.
[15] David H Cousins, David Gerrett, and Bruce Warner. A review of medication incidents
reported to the national reporting and learning system in england and wales over 6
years (2005-2010). British journal of clinical pharmacology, 74(4):597-604, October
2012. PMID: 22188210 PMCID: PMC3477327.
[16] Guido Alejandro Davidzon, University-MIT Division of Health Sciences Harvard, and
Technology. Using EMR transactionaldata for personalized clinical decision support.
2010.
[17] R F DeBusk, N H Miller, H R Superko, C A Dennis, R J Thomas, H T Lew, 3rd
Berger, W E, R S Heller, J Rompf, D Gee, H C Kraemer, A Bandura, G Ghandour,
M Clark, R V Shah, L Fisher, and C B Taylor. A case-management system for coronary
risk factor modification after acute myocardial infarction. Annals Of Internal Medicine,
120(9):721-729, May 1994.
[18] L Dolovich, K Pottie, J Kaczorowski, B Farrell, Z Austin, C Rodriguez, K Gaebel,
and C Sellors. Integrating family medicine and pharmacy to advance primary care
therapeutics. Clinical Pharmacology &#38; Therapeutics, 83(6):913-917, March 2008.
[19] Colin R Dormuth, Tarita A Miller, Anjie Huang, Muhammad M Mamdani, David N
Juurlink, and Canadian Drug Safety and Effectiveness Research Network. Effect of a
centralized prescription network on inappropriate prescriptions for opioid analgesics
and benzodiazepines. CMAJ: Canadian Medical Association journal = journal de
l'Association medicale canadienne, 184(16):E852-856, November 2012. PMID: 22949563
PMCID: PMC3494359.
[20] Michael A Fischer, Margaret R Stedman, Joyce Lii, Christine Vogeli, William H Shrank,
M Alan Brookhart, and Joel S Weissman. Primary medication non-adherence: analysis
of 195,930 electronic prescriptions. Journal Of General Internal Medicine, 25(4):284290, April 2010.
108
[21] David C. Grabowski, Darius N. Lakdawalla, Dana P. Goldman, Michael Eber, Larry Z.
Liu, Tamer Abdelgawad, Andreas Kuznik, Michael E. Chernew, and Tomas Philipson.
The large social value resulting from use of statins warrants steps to improve adherence
and broaden treatment. Health Affairs, 31(10):2276-2285, October 2012.
[22] Joshua A. Hanson, Design System, Management Program, and Institute of Technology Massachusetts. The medication mismanagement system: causes, evidence of user
innovation, and a view towards a product/service solution for the elderly. 2010.
[23] B. R. Hemmelgarn, W. A. Ghali, and H. Quan. A case study of hospital closure and
centralization of coronary revascularization procedures. CanadianMedical Association
Journal, 164(10):1431-1435, May 2001. WOS:000168696900020.
[24] P Michael Ho, Chris L. Bryson, and John S. Rumsfeld. Medication adherence: Its
importance in cardiovascular outcomes. Circulation June 16, 2009, 119(23):3028-3035,
2009.
[25] Jenna Howard, Elizabeth C. Clark, Asia Friedman, Jesse C. Crosson, Maria Pellerano, Benjamin F. Crabtree, Ben-Tzion Karsh, Carlos R. Jaen, Douglas S. Bell, and
Deborah J. Cohen. Electronic health record impact on work burden in small, unaffiliated, community-based primary care practices. Journal of General Internal Medicine,
28(1):107-113, August 2012.
[26] Jane Hummer and Cristina Daccarett. Improvement in prescription renewal handling
by application of the lean process, June 2009.
[27] Brent C. James and Lucy A. Savitz. How intermountain trimmed health care costs
through robust quality improvement efforts. Health Affairs, 30(6):1185-1191, 2011.
[28] Jae Kennedy, Iulia Tuleu, and Katherine Mackay. Unfilled prescriptions of medicare
beneficiaries: prevalence, reasons, and types of medicines prescribed. Journal of managed care pharmacy: JMCP, 14(6):553-560, August 2008. PMID: 18693779.
[29] Jeannie K. Lee, Karen A. Grace, and Allen J. Taylor. Effect of a pharmacy care program
on medication adherence and persistence, blood pressure, and low-density lipoprotein
cholesterol. JAMA: The Journal of the American Medical Association, 296(21):25632571, December 2006.
[30] Els Mehuys, Koen Boussery, Els Adriaens, Luc Van Bortel, Leen De Bolle, Inge Van Tongelen, Jean--Paul Remon, and Guy Brusselle. COPD management in primary care:
an observational, community pharmacy-based study. The Annals of pharmacotherapy,
44(2):257-266, February 2010. PMID: 20103611.
[31] Suzanne 0. Minassian, Michael J. Muller, and Daniel Gruen. Diverse strategies for
interruption management in complex office activities. Poster submitted to CSCW, 2004.
[32] Stephen Monsell. Task switching. Trends in Cognitive Sciences, 7(3):134-140, March
2003.
109
[33] Donald E. Morisky, Lawrence W. Green, and David M. Levine. Concurrent and predictive validity of a self-reported measure of medication adherence. Medical Care, 24(1):6774, January 1986.
[34] Andrew B Morris, Jingjin Li, Kurt Kroenke, Tina E Bruner-England, Jim M Young,
and Michael D Murray. Factors associated with drug adherence and blood pressure
control in patients with hypertension. Pharmacotherapy,26(4):483-492, April 2006.
PMID: 16553506.
[35] Paul J Nietert, Barbara C Tilley, Wenle Zhao, Peter F Edwards, Andrea M Wessell,
Patrick D Mauldin, and Pam P Polk. Two pharmacy interventions to improve refill
persistence for chronic disease medications: a randomized, controlled trial. Medical
care, 47(1):32-40, January 2009. PMID: 19106728.
[36] Marwa Noureldin, Kimberly S Plake, Daniel G Morrow, Wanzhu Tu, Jingwei Wu, and
Michael D Murray. Effect of health literacy on drug adherence in patients with heart
failure. Pharmacotherapy,32(9):819-826, September 2012. PMID: 22744746.
[37] Vincent Pradel, Catherine Delga, Frank Rouby, Jo??lle Micallef, and Maryse LapeyreMestre. Assessment of abuse potential of benzodiazepines from a prescription database
using 'doctor shopping' as an indicator. CNS drugs, 24(7):611-620, July 2010. PMID:
20527997.
[38] Devon J. Price, School of Management Sloan, Institute of Technology Massachusetts,
for Global Operations Program Leaders, and General Hospital Massachusetts. Managing variability to improve quality, capacity and cost in the perioperative process at
Massachusetts General Hospital. 2011.
[39] Ashleigh Royalty Range, School of Management Sloan, Institute of Technology Massachusetts, and for Global Operations Program Leaders. Improving surgical patient
flow through simulation of scheduling heuristics. 2013.
[40] Haim Reuveni, Boaz Sheizaf, Asher Elhayany, Michael Sherf, Yehuda Limoni, S. Scharff,
and Ronit Peled. The effect of drug co-payment policy on the purchase of prescription
drugs for children with infections in the community. Health Policy, 62(1):1, October
2002.
[41] Pablo Santibanez, Vincent Chow, John French, Martin Puterman, and Scott Tyldesley.
Reducing patient wait times and improving resource utilization at BCCA's ambulatory
care unit through simulation. In CIHR Team Working Paper Series. CIHR.
[42] Matthew R. Schlanser, School of Management Sloan, Institute of Technology Massachusetts, and for Global Operations Program Leaders. Optimization of surgical supply
inventory and kitting. 2013.
[43] Trevor A. Schwartz, School of Management Sloan, Institute of Technology Massachusetts, and for Global Operations Program Leaders. Improving surgical patient
flow in a congested recovery area. 2012.
110
[44] Tait D. Shanafelt, Sonja Boone, Litjen Tan, Lotte N. Dyrbye, Wayne Sotile, Daniel
Satele, Colin P. West, Jeff Sloan, and Michael R. Oreskovich. Burnout and satisfaction
with work-life balance among US physicians relative to the general US population.
Archives of Internal Medicine, 172(18):1377, October 2012.
[45] S. A. Shipman and C. A. Sinsky. Expanding primary care capacity by reducing waste
and improving the efficiency of care. Health Affairs, 32(11):1990-1997, November 2013.
[46] C. A. Sinsky, R. Willard-Grace, A. M. Schutzbank, T. A. Sinsky, D. Margolius, and
T. Bodenheimer. In search of joy in practice: A report of 23 high-functioning primary
care practices. The Annals of Family Medicine, 11(3):272-278, May 2013.
[47] Thomas A. Sinsky and Christine A. Sinsky. A STREAMLINED APPROACH TO
prescription management. Family, page 11, December 2012.
[48] Michael C. Sokol. Impact of medication adherence on hospitalization risk and healthcare
cost. Medical Benefits, 22(16):4-4, August 2005.
[49] James E. Stahl, Mark S. Roberts, and Scott Gazelle. Optimizing management and
financial performance of the teaching ambulatory care clinic. Journal of general internal
medicine, 18(4):266--274, 2003.
[50] J F Steiner, T D Koepsell, S D Fihn, and T S Inui. A general method of compliance
assessment using centralized pharmacy records. description and validation. Medical care,
26(8):814-823, August 1988. PMID: 3398608.
[51] L R Strandberg, G W Dawson, D Mathieson, J Rawlings, and B G Clark. Effect of comprehensive pharmaceutical services on drug use in long-term care facilities. American
journal of hospital pharmacy, 37(1):92-94, January 1980. PMID: 6987865.
[52] Craig Tanio and Chr??stooher Chen. Innovations at miami practice show promise for
treating high-risk medicare patients. Health Affairs, 32(6):1078-1082, June 2013.
[53] D J Tanner. Comprehensive pharmacy services in an 85-bed hospital. American journal
of hospital pharmacy, 33(4):340-349, April 1976. PMID: 817598.
[54] Jonathan M Teich, Jerome A Osheroff, Eric A Pifer, Dean F Sittig, Robert A Jenders,
and CDS Expert Review Panel. Clinical decision support in electronic prescribing:
recommendations and an action plan: report of the joint clinical decision support workgroup. Journal of the American Medical Informatics Association: JAMIA, 12(4):365-
376, August 2005. PMID: 15802474 PMCID: PMC1174880.
[55] J. I. Westbrook, E. Coiera, W. T. M. Dunsmuir, B. M. Brown, N. Kelk, R. Paoloni, and
C. Tran. The impact of interruptions on clinical task completion. Quality and Safety
in Health Care, 19(4):284-289, May 2010.
[56] M C S Wong, J Y Jiang, and S M Griffiths. Adherence to lipid-lowering agents among
11,042 patients in clinical practice. Internationaljournal of clinical practice, 65(7):741-
748, July 2011. PMID: 21676117.
111
[57] Martin C S Wong, Wilson W S Tam, Clement S K Cheung, Ellen L H Tong, Antonio
C H Sek, N T Cheung, Stephen Leeder, and Sian Griffiths. Medication adherence to
first-line antihypertensive drug class in a large chinese population. Internationaljournal
of cardiology, 167(4):1438-1442, August 2013. PMID: 22560948.
[58] M W J M Wouters, H E Karim-Kos, S le Cessie, B P L Wijnhoven, L P S Stassen,
W H Steup, H W Tilanus, and R a E M Tollenaar. Centralization of esophageal cancer
surgery: does it improve clinical outcome? Annals Of Surgical Oncology, 16(7):1789-
1798, July 2009.
[59] Jamie Young, Alistair Thompson, Iain Tait, Lynsey Waugh, and Gillian McPhillips.
Centralization of services and reduction of adverse events in pancreatic cancer surgery.
World Journal of Surgery, 37(9):2229-2233, September 2013. WOS:000323369400028.
[60] Yuting Zhang, Joseph P Newhouse, and Katherine Baicker. Are drugs substitutes or
complements for intensive (and expensive) medical treatment. American Economic
Review, 101(3):393-397, May 2011.
112