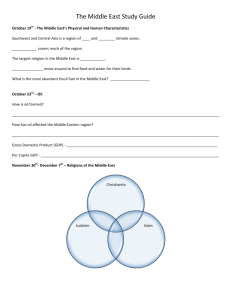
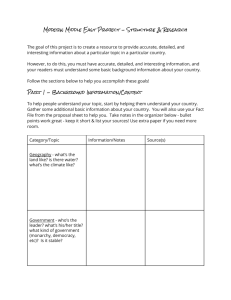
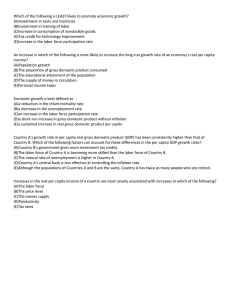
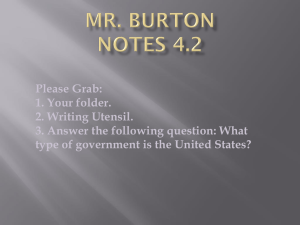
PRELIMINARY Not for quotation Health Spending, Health Outcomes, and Per Capita Income in Canada: A Dynamic Analysis Kathleen Day* and Julie Tousignant** May 29, 2003 * Department of Economics, University of Ottawa, 200 Wilbrod Street, Ottawa, K1N 6N5. e-mail: kmday@uottawa.ca ** Economic and Fiscal Policy Branch, Department of Finance, 140 O’Connor Street, Ottawa, K1A 0G5. e-mail: Tousignant.Julie@fin.gc.ca 1. Introduction While there has been much discussion of the rising cost of the health system in Canada, there does not seem to be much analysis of the relationship between spending on health and health outcomes (i.e. population health status) in Canada. Most existing studies of this relationship use either international cross-section data or time-series data pooled across countries. Some recent studies have found a positive relationship between spending on health and health outcomes (Or 2000a,b; Baldacci et al. 2002), but others did not find a significant relationship between the two variables (Filmer and Pritchett 1999, Thornton 2002). Still others, such as Baldacci et al. (2002), find that their results depend on the data set and/or estimation methods used. All studies find a positive and significant relationship between health outcomes and real per capita income. To date, it seems that only three papers on the topic have focused on Canada, although Canada is included in the panel data sets used by Or (2000a,b) and Hitiris and Posnett (1992). Crémieux et al. (1999) examine the relationship between health indicators such as infant mortality rates and life expectancy and total (public and private) per capita spending on health, using pooled time-series cross-section data for the ten provinces for the period 1978-1992 (Crémieux et al., 1999). Kee (2001) also uses pooled time-series cross-section data for the ten provinces for the 1975-1996 period. As do Crémieux et al. (1999), Kee regresses indicators of population health (infant mortality rates, life expectancy, and age-standardized mortality rates) on a number of variables, including real per capita public expenditures on health. However, unlike Crémieux et al. (1999), Kee uses instrumental variables estimation to control for possible simultaneity between health status and public spending on health. Both studies find a statistically significant relationship between health status and both health spending and per capita income. Finally, Deussing (2003), who used microdata from the 1996 National Population Health Survey for Canada, finds that provincial government spending on health has no impact on self-assessed health status. A related strand of literature has examined the determinants of health expenditures (Gerdtham et al. 1992, Hitiris and Posnett 1992, Di Matteo and Di Matteo 1998). Much of this literature has focused on the relationship between aggregate health spending and per capita GDP in OECD countries, with the most recent studies applying unit root and cointegration tests in an attempt to determine whether per capita health expenditures and per capita GDP are cointegrated (Hansen and King 1996, 1998; McCoskey and Seldon 1996; Blomqvist and Carter 1997; Gerdtham and Löthgren 2000, 2001; Okunade and Karakus 2001; Jewell et al. 2003). These studies were motivated by the suspicion that the counter-intuitive finding of earlier studies that health care was a luxury good, not a necessity, was a spurious result due to the presence of unit roots in time-series data on per capita health spending and GDP per capita. However, with the exception of Hitiris and Posnett (1992) these studies seem to have excluded health outcomes from their analysis. Furthermore, they focus on the long-run relationship between the variables and do not explore the short-run dynamics. 2 The exclusion of some indicator of health outcomes from studies of the long-run relationship between per capita health spending and per capita GDP is surprising given that several studies of the determinants of health outcomes have pointed to simultaneity between health outcomes and per capita health spending as a possible source of bias (Filmer and Pritchet 1999, Kee 2001). In addition, from the point of view of policy makers, it would be desirable to know more about the short-run dynamics of the relationship between health outcomes, health spending, and GDP per capita as well as about the long-run relationship between the variables. For example, they might be interested in knowing how a permanent increase in per capita health spending is likely to affect the economy in the short run as well as the long run. To this end, we explore the dynamic relationship between three variables: real per capita income (as measured by GDP or GNP), real per capita spending on health and an indicator of health outcomes, using time-series data for Canada. With data from the Historical Statistics of Canada we explore this relationship for the longest time period possible. In order to do this, we examine different subsets of variables during the periods 1926-1999 and 1950-1997. For purposes of comparison with earlier studies that used post-1960 panel data for OECD countries we also carry out an analysis for the period 1960-1997. Although other studies provide evidence that other variables (eg., demographic structure, tobacco and alcohol consumption, environmental quality) also influence per capita health care spending and health outcomes, in this paper we restrict our attention to a three-variable system because it is not possible to find extensive timeseries on many of these other variables. We also experiment with three different health indicators: the infant mortality rate, age-standardized mortality rate, and a composite of a group of standard health indicators constructed using principle components analysis. Unit root and cointegration tests are used to help identify the appropriate dynamic model. Our econometric analysis differs from that of previous studies in that we make use of a relatively new unit root test proposed by Elliot, Rothenberg, and Stock (1996), and a new lag selection criterion for unit root tests proposed by Ng and Perron (2001). The results indicate that the dynamic relationship between the three variables may be more complex than what previous studies have indicated. 2. Econometric Methods The objective of this paper is to build a simple dynamic model of the relationship between three variables. Since the choice of specification for a dynamic model depends on whether or not the included variables have unit roots, we begin our analysis by testing for the presence of unit roots in the data during each of the time periods considered. Many different unit root tests have been proposed and it is well-known that many of them suffer from a lack of power.1 Previous studies of the relationship between per capita health expenditures and per capita GDP have used a variety of different tests, including the augmented Dickey-Fuller (ADF) test (Hansen and King 1996, Okunade and Karakus 2001, Gerdtham and Löthgren 2001) the Phillips-Perron (PP) test (Blomqvist and Carter 1 See Maddala and Kim (1998) for a recent survey of unit root tests and their properties. 3 1997, Okunade and Karakus 2001), the Im, Pesaran, and Shin (IPS) (2003) panel unit root test (McCoskey and Selden 1998, Gerdtham and Löthgren 2001, 2001; Okunade and Karakus 2001), and the Im, Lee, and Tieslau (ILT) (2002) panel unit root test that allows for an unknown structural break (Jewell et al. 2003). Because we are restricting our attention to Canada alone, panel unit root tests are out of the question. Instead, we use the ADF test with GLS detrending, called the ADF-GLS test, proposed by Elliot, Rothenberg, and Stock (1996). Elliot et al. show that the power of the ADF test in the case of series with a constant mean and/or a deterministic trend is improved considerably by the method they propose to estimate the coefficients of the deterministic terms. Usually the coefficients of these terms are estimated simultaneously with the test statistic by including a constant or a constant and trend in the test equation. Elliot et al. suggest estimating these coefficients before estimating the test statistic, using OLS applied to quasi-differences of the original series and the deterministic terms. Then these estimated coefficients are used to detrend the original series, and the ADF test is applied to the detrended residuals. To be more precise, the ADF-GLS test is based on the equation k ∆~ yt = β 0 ~ yt −1 + ∑ β j ∆ ~ yt − j + ε tk , (1) j =1 where yt is the series to be examined, εtk is a random error term, ~ y t = y t − ψˆ ′z t , zt is a p by 1 vector of deterministic terms, ψˆ is the OLS estimator of the vector y in the regression of ya = (y1, y2 - a y1 , …, yT - a yT −1 )′ on za = (z1, z2 - a z1 , …, zT - a zT −1 )′ , and a = 1 + c / T . Elliot et al. (1996) recommend that c be set equal to –7 when zt consists solely of a constant and equal to –13.5 when zt includes a constant and a trend. The test of the null hypothesis of a unit root is based on the t ratio of β̂ 0 , the estimated coefficient of ~ y t −1 . In the case where zt includes a constant term only, the critical values for the test are identical to those for the standard ADF test with neither constant nor trend. Elliot et al. (1996) provide asymptotic critical values for the case where zt includes a constant and a trend, as well as critical values for 50, 100, and 200 observations. The standard ADF test should be used in cases where yt is believed to have a zero mean (in which case no deterministic terms are necessary). Like the standard ADF test, the ADF-GLS test is sensitive to the choice of k, the number of lagged terms to be included in the test equation. Recently Ng and Perron (2001) have demonstrated that additional gains in the power of the ADF-GLS test can be achieved by using a modified version of the AIC criterion, which they call the MAIC. We therefore use this criterion to choose k for the ADF-GLS test.2 When data series are found to contain unit roots, the next step in the analysis is to test for cointegration between the variables. Most econometric analyses of cointegration have focused on the case where all variables are I(1), or integrated of order 1. In this case, we 2 Both the ADF-GLS unit root test and automated lag length selection based on the MAIC have recently been implemented in EViews 4.1, which we used to carry out our analysis. 4 apply Johansen’s trace test and maximum eigenvalue tests, described in Johansen (1995a). Prior to the application of the tests we use a system AIC to choose a lag length for each unrestricted VAR model. The analysis of systems with I(2) variables is left to future research. 3. Data For the purposes of this study, we need data on three variables: a measure of the population’s health, a measure of real per capita spending on health, and a measure of real per capita income. As there is no general agreement as to what is the best measure of the overall health of the population, we use several different measures, all of which are discussed in section 3.1. In addition, in order to obtain long time series of data on health spending and income per capita, certain assumptions had to be made about how to link overlapping data series. Further details about data sources and the construction of the data are provided in the data appendix, while the behaviour of the data over the sample period is discussed in sections 3.2 and 3.3. 3.1 Measures of population health Health status, which refers to the level of health of an individual, group or population, is difficult to estimate and there is no universally accepted indicator that captures all the aspects of health. Different measures of health status are available but they provide only a partial perspective on the population’s level of health. The most commonly used indicators are based on mortality data. These indicators capture the decrease in mortality and therefore provide an indication of improvement in the quantity of life, not in the quality of life. This means that even if these measures show an improvement in longevity, they are not sufficient to indicate that health status has improved. The following is a list of commonly used measures:3 1) Potential Years of Life Lost (PYLL) consists of the number of years of life “lost” when a person dies before age 70 or age 75. It provides an indirect estimate of how many deaths could be potentially avoided. The rate per 100,000 population is more useful because it takes into account the effect of the size of the population. 2) The Infant Mortality Rate (IMR) refers to the number of deaths per 1,000 live births. It generally reflects the level of mortality and the effectiveness of preventive care and the attention paid to maternal and child health. 3) The Perinatal Mortality Rate (PMR) consists in the count and rate of fetal deaths of 28 or more weeks gestation and infant deaths under 1 week per 1,000 total births. This indicator reflects standards of obstetric and pediatric care, as well as the effectiveness of public health initiatives. 3 This list is taken from http://www.statcan.ca/english/freepub/82-221-XIE/free.htm . 5 4) The Age-Standardized Mortality Rate (ASM) is the number of deaths per 100,000 of total population, standardized for the age composition of the population. The use of a standard population adjusts for variations in population age distributions over time and across different geographic areas. 5) Life Expectancy (LE) is the number of years a person would be expected to live, starting from birth (for life expectancy at birth) or at age 65 (for life expectancy at age 65), on the basis of the mortality statistics for a given observation period. It measures quantity rather than quality of life. 6) Probability of Survival from Birth to Age 80 is the probability of a newborn infant surviving to age 80, if subject to prevailing patterns of age specific mortality rates. This measure is recent and not widely used. Statistics Canada provides it for the period 1986 to 1996. Recently, other measures have been developed that aim at measuring the quality as well as the quantity aspect of life associated with health, such as Health-Adjusted Life Expectancies (HALEs) and Disability-Adjusted Life Years (DALY).4 Essentially, these measures adjust life expectancy for quality of life mainly by using years of life without any activity limitation. In this study, only five of the indicators will be used as measures of health status because of the absence of data for a long period of time. These measures are the infant mortality rate (IMR), the perinatal mortality rate (PMR), the age-standardized mortality rate (ASM), life expectancy at birth (LEB), and life expectancy at 65 (LE65). The infant mortality rate is used for our analysis because it is available for the 1926-1999 time period. The IMR and the ASM are both used in our analysis of the 1950-97 and post1960s periods. Figure 1 shows the evolution of IMR, PMR, ASM, LEB and LE65 between 1950 and 1997. All the indicators show an improvement in health status between 1950 and 1997.5 The greatest improvements (in percentage terms) over the 1950-1997 period have been in IMR and PMR, while LEB and LE65 improved the least. The improvements in IMR and LEB reflect observations made in previous work which suggest that life expectancy at birth has increased primarily as a result of the reduction in infant mortality rates, since the effect on life expectancy is larger when mortality rates fall at younger ages. The percentage improvement in ASM lies between that of the other four measures over the period 1950-1997. 4 See Jee and Or (1998) for a discussion of these and other alternative health indicators. The indicators have been converted to indexes with their first year equal to 100, thus any improvement in the measure reflects improvement in the population health status. IMR, ASM, PYLL and PMR would ordinarily show an improvement in the health status of the population through a decline in their levels (i.e, a decline in mortality means children are healthier), but to make them comparable to life expectancy in the figures their growth rates were multiplied by –1. 5 6 When we consider a longer time horizon, between 1926 and 1997, the greatest improvements (in percentage terms) are again observed for IMR and PMR, while LEB and LE65 improved the least (Figure 2). However, the improvement in LEB is greater when 1926 serves as the base year, while the evolution remained comparable for the other three variables. Lise (2000) notes that prior to the mid 1960s, the increase in life expectancy at birth was the result of more people surviving childhood and early working years and living to old age. Since the mid 1960s, while falling childhood mortality has continued to be an important factor, there have also been increased gains resulting from falling mortality rates over age 55, leading to increased years of old age. However, the total improvement in LEB since the mid 1960s has been only about half of the gain during the previous 40 years. Finally, for the 1950-1997 and 1960-1997 periods we also use a composite indicator constructed from five of the individual measures. While the health status indicators discussed above provide different perspectives on population health, they are all derived from vital statistics data on death rates and are highly correlated. A summary indicator that could account for a high proportion of the variation in the group of indicators considered may serve as a good overall indicator of health status. To construct a summary indicator, principal components analysis was used.6 This mechanical procedure produces a single indicator of health status (the first principal component) summarizing the information contained in multiple measures using a linear function that applies a different weight to each variable. An indicator summarizing IMR, ASM, PMR, LEB and LE65 was computed (Figure 3). Its behaviour throughout the 1950 and 1997 period shows a clear improvement in population health status. Other indicators can be computed for different time periods and different subsets of the individual indicators. 3.2. Public/Private Health Spending in Canada Figure 4 presents a brief portrait of the evolution of health spending in Canada. Since 1975, public health spending (real per capita, age-adjusted, internal calculations)7 has fluctuated somewhat but has increased overall from approximately $9,000 in 1976 to $12,000 in 2001. Private health spending (real per capita, age-adjusted) over the same period increased from $3,000 to $5,000. Between 1975 and 1991, public sector spending grew rapidly but between 1993 and 1997 it decreased in real per capita terms. This reduction coincides with the period in which Established Programs Financing (EPF) and the Canada Assistance Plan (CAP) were consolidated into the Canada Health and Social Transfer (CHST) and total cash payments under this program were reduced. 6 For more information, see chapter 7 of Morrison (1967). The authors would like to thank Harriet Jackson and Alison McDermott, economists at Finance Canada, Fiscal Policy Division, for providing these numbers. 7 7 Since real per capita age adjusted expenditures are only available for a short period of time, total real health expenditures per capita, i.e. the sum of private and public spending, will be used. This is done to capture the variation in spending between the two sectors and because the breakdown is not available historically as far as we would like. Since 1945, total real health expenditures per capita have increased (Figure 5), aside from the 1993 to 1997 period where they remained stable, reflecting the public sector spending period mentioned above. 3.3 Real income per capita Real income per capita is measured by GDP per capita in most studies of the determinants of health spending and health outcomes. However, real GDP is not available for Canada for the entire 1926-1999 period. Therefore we use real GDP per capita only for the 1950-1997 and 1960-1997 periods. For the 1926-1999 period, we use real GNP per capita. Figure 6 illustrates the behaviour of the two series, in millions of 1997 dollars, over the 1926-1999 period. It can be seen that the two series behave in a very similar fashion and increased overall throughout time. 4. Results In this section we report the results of unit root and cointegration tests for the three different time periods analyzed: 1960-1997, 1950-1997, and 1926-1999. All tests were applied to the natural logs of the variables. 4.1 1960-1997 As noted in the introduction, recently a number of authors have tested for unit roots and cointegration between real per capita health expenditures and real per capita GDP in OECD countries, using different unit root and cointegration tests. The sample period covered by these studies varies, but all begin in 1960. Their results for Canada are summarized in Table 1. A glance at Table 1 reveals substantial disagreement between the previous studies on the order of integration of real per capita health expenditures and real per capita GDP in Canada. Even studies which appear to use the same data (they cite the same sample period and data source) obtain different results. In some cases these differences may be due to the fact that not all studies tested explicitly for the order of integration; of the four studies that used data for the period 1960-1997, only Okunade and Karakus (2001) and Gerdtham and Löthgren (2000) provide the results of unit root tests for both the levels and the first differences of variables, which may help to explain why Okunade and Karakus (2001) are the only ones to conclude that for Canada, health expenditures were 8 integrated of order 2 (using both the ADF and PP tests).8 The ADF tests (but not the PP tests) carried out by Okunade and Karakus also implied that per capita GDP was integrated of order 2. Jewell et al. (2003), on the other hand, using a panel unit root test that allows for the possibility of structural break, found that per capita GDP was trendstationary (with no breaks) for Canada. The results of the ADF-GLS tests for real per capita total health expenditures (LTHE), real per capita public health expenditures (LPHE), real GDP per capita (LGDP), and three alternative indicators of health outcomes (the composite indicator, age-standardized mortality rate, and the infant mortality rate) are presented in Table 2. To determine the order of integration of each variable for each time period, we apply the ADF-GLS test to the levels, first differences, and if necessary, the second differences of the series. Since the graphs in section 3 indicate that all the data series exhibit clear trends, for tests on the levels of all variables, zt is assumed to consist of a constant and a trend; for the first differences, only a constant term is included in zt; and for the second differences, which appear to have a zero mean, the standard ADF test with neither constant nor trend is used. In all three cases the MAIC was used to select the appropriate number of lagged terms to include in the test equation. While for most of the variables the results with respect to the order of integration during the 1960-1997 period are clear, in the case of total health expenditures it is not entirely clear whether the series is I(1) or I(2). We can reject the null hypothesis of a unit root in the first difference of LTHE, but only at the 10% level of significance. The second difference of LTHE is definitely stationary, at even the 1% level of significance. Public health expenditures, however, are clearly I(2), and as in most of the previous studies, per capita GDP is found to be I(1). Of the three indicators of health outcomes, only the agestandardized mortality rate (LASM) is I(1), while the infant mortality rate (LIMR) and the composite indicator (LHS) are both I(2). These findings have important implications for cointegration testing. If in fact the orders of integration of total health expenditures and GDP are different, then they cannot be cointegrated in a bivariate model. This would contradict the findings of Blomqvist and Carter (1997) and Gerdtham and Löthgren (2000, 2001). Furthermore, cointegration would also be impossible in a trivariate model including LTHE, LGDP, and LASM since such a model would include only one I(2) variable. The possibility remains that cointegration might exist in a trivariate model in which either LHS or LIMR were used as the indicator of health outcomes, but the most widely-used tests for cointegration, Johansen’s trace and maximum eigenvalue tests, would not be valid in this I(2) model. It is also possible that public health spending may be cointegrated with LGDP and either LHS or LIMR. 8 In footnote 15 of their paper Gerdtham and Löthgren (2000) note that ADF tests applied to the first differences of the log of per capita health expenditures (with a constant but no trend included in the test equation) led to the conclusion that this variable was I(1) in all but four of the 21 countries they examined. However, they do not indicate the countries in which per capita health spending was I(2). 9 If instead LTHE is I(1), then we can use Johansen’s trace and maximum eigenvalue tests to test for cointegration between the I(1) variables LTHE, LGDP, and LASM, or between any pair of these variables. Table 3 presents the results of cointegration tests for I(1) vector error correction models (VECM) involving these three variables. Except where indicated, the tests were carried out under the assumption that both a constant and a trend appear in the cointegrating equations. For the trivariate model including per capita total health expenditures, per capita GDP, and the age-standardized mortality rate, it is possible to reject the null hypothesis of no cointegrating vectors at the 10% level of significance. However, the test statistics are only marginally significant; if we were to apply the degrees of freedom correction proposed by Reimers (1992) it would be impossible to reject the null hypothesis.9 Similarly, when a trend is included in the cointegrating equation we do not find cointegration in any of the bivariate models analyzed. With respect to the bivariate model that includes per capita total health spending and per capita GDP, our results thus contradict the earlier findings of Blomqvist and Carter (1997), and Gerdtham and Löthgren (2000, 2001). This finding raises the possibility that the results of previous studies of the relationship between these variables that did not test for cointegration may not be reliable. 4.2 1950-1997 For the 1950-1997 period, the results of the ADF-GLS tests are presented in Table 4. For all of the variables the results with respect to the order of integration during the period are clear: the series are I(2). The second differences of all variables are definitely stationary at the 1% level of significance, but neither the levels nor first differences are stationary at even the 10% level of significance. Again, these results have important implications for cointegration testing. Since all variables are of the same order of integration, cointegration may exist in either a trivariate or a bivariate system. However, the most widely-used tests for cointegration, Johansen’s trace and maximum eigenvalue tests, are not valid in an I(2) model. The problem of testing for cointegration in I(2) systems with a deterministic trend has recently been discussed by Rahbek et al. (1999), but we have not applied their tests in this paper.10 4.3 1926-1999 For the 1926-1999 period, the results of the ADF-GLS tests for real GNP per capita and the infant mortality rate are presented in Table 5. As in the shorter sample periods, the 9 The results of the trace and maximum eignevalue tests assuming a constant but no trend for the other models are not reported here, as they either were the same as for the case reported or indicated that the variables were stationary. The latter conclusion conflicts with the results of the unit root tests and can be regarded as a sign of model misspecification. 10 Testing and estimation in I(2) systems is also addressed in Johansen (1995b). 10 results indicate that the infant mortality rate is integrated of order 2, as we can reject the null hypothesis that the second difference of LIMR has a unit root at the 1% level of significance. In the case of real GNP per capita, the results indicate that we can reject the null hypothesis of a unit root in the level of LGNP at the 5% level of significance, which suggests that real GNP per capita is trend stationary with no unit roots. This result is somewhat surprising, since real GDP per capita was found to have a unit root in the shorter sample periods. The fact that the orders of integration of the two variables are different means that LGDP and LIMR cannot be cointegrated in a bivariate model. Thus no further analysis of this long time period is possible without the addition of more variables to the system. 5. Conclusion Despite considering three different health indicators and two different measures of health spending, in this paper we have not managed to achieve our objective of building a simple dynamic model of the relationship between per capita health spending, per capita GDP, and health outcomes. But several conclusions can be drawn from the analysis. First of all, the results of the unit root tests are clearly sensitive to the choice of sample period. For example, real per capita GDP was found to be integrated of order 2 and integrated of order 1, depending on the sample period. Similarly, the order of integration of some health indicators and measures of per capita health spending seems to depend on the choice of sample period. Second, we found little evidence of cointegration between per capita health spending, per capita GDP, and health outcomes during the 1960-1997 period. Furthermore, the infant mortality rate and per capita GDP do not seem to be cointegrated during the longer 19261999 time period. Cointegration tests were not carried out for the 1950-1997 period because during this period, all the variables examined appeared to be integrated of order 2. Further testing and estimation of a more complex model for I(2) variables along the lines proposed by Rahbeck et al. (1999) is required to pinpoint the number of cointegrating vectors and analyze the dynamic behaviour of the variables. What do these results imply regarding the relationship between per capita health spending, per capita GDP, and health outcomes? Although on the surface the results seem to suggest the lack of a long-run relationship between the variables, in fact what they may really imply is that the simple bivariate and trivariate models analyzed in this paper are inadequate. There are at least two possible directions for further research worth pursuing. First, it may be the case that as Jewell et al. (2003) conclude, the variables we have examined are in fact stationary around a broken deterministic trend. Although a break is not obvious in the plots of the data, both public and private health spending are likely to have been affected by such major policy changes in the funding of health care medicare in Canada. The application of unit root and/or cointegration tests that allow for the possibility of unknown structural breaks would therefore be a good idea.11 11 Recently Peron and Rodriguez (2003) have extended the unit root tests of Elliot et al. (1996) and Ng and Perron (2001) to the case of single unknown structural break. 11 Second, the observed lack of cointegration between the I(1) variables examined may be an indication of model misspecification rather than the absence of any long-run relationship between the variables. If so, it would be worthwhile to develop a more complete structural model of the interactions between per capita health spending, per capita GDP, and health outcomes (in addition to estimating an I(2) model for the 19501997 period). While the sample period available for the estimation of such a model would necessarily be more restricted than that employed here, it is possible that cointegration might in fact exist in a properly specified model. 12 REFERENCES Baldacci, E., M.T. Guin-Siu, M.T., and L. de Mello (2002) “More on the Effectiveness of Public Spending on Health Care and Education: A Covariance Structure Model.” IMF Working Paper WP/02/90, Washington, International Monetary Fund. Blomqvist, Å.G., and R.A.L. Carter (1997) “Is Health Care Really a Luxury?” Journal of Health Economics 16, 207-229. Crémieux, P.-Y., P. Ouellette, and C. Pilon (1999) “Health Care Spending as Determinants of Health Outcomes.” Health Economics 8, 627-639. Deussing, M.-A. (2003) “An Empirical Analysis of the Relationship between Public Health Spending and Self-Assessed Health Status: An Ordered Probit Model.” M.A. Major Paper, Department of Economics, University of Ottawa, Ottawa. Di Matteo, L., and R. Di Matteo (1998) “Evidence on the Determinants of Canadian Provincial Government Health Expenditures: 1965-1991.” Journal of Health Economics 17, 211-228. Elliott, G., T.J. Rothenberg, and J.H. Stock (1996) “Efficient Tests for an Autoregressive Unit Root.” Econometrica 64(4), 813-836. Filmer, D., and L. Pritchett (1999) “The Impact of Public Spending on Health: Does Money Matter?” Social Science and Medicine 49, 1309-1323. Gerdtham, U.-G., J. Søgaard, F. Andersson, and B. Jönsson (1992) “An Econometric Analysis of Health Care Expenditure: A Cross-section Study of OECD Countries.” Journal of Health Economics 11, 63-84. Gerdtham, U.-G., and M. Löthgren (2000) “On Stationarity and Cointegration of International Health Expenditure and GDP.” Journal of Health Economics 19, 461-475. Gerdtham, U.-G., and M. Löthgren (2002) “New Panel Results on Cointegration of International Health Expenditure and GDP.” Applied Economics 34, 1679-1686. Hansen, P., and A. King (1996) “The Determinants of Health Care Expenditure: A Cointegration Approach.” Journal of Health Economics 15, 127-137. Hansen, P., and A. King (1998) “Health Care Expenditure and GDP: Panel Unit Root Test Results – Comment.” Journal of Health Economics 17, 377-381. Hitiris, T., and J. Posnett (1992) “The Determinants and Effects of Health Expenditure in Developed Countries.” Journal of Health Economics 11, 173-181. 13 Im, K.S., J. Lee, and M. Tieslau (2002) “Panel LM Unit Root Tests with Level Shifts.” Mimeo, Department of Economics, University of Florida. Im, K.S., M.H. Pesaran, and Y. Shin (2003) “Testing for Unit Roots in Heterogeneous Panels.” Journal of Econometrics, in press-. Jee, M., and Z. Or (1998) “Health Outcomes in OECD Countries: A Framework of Health Indicators for Outcome-Oriented Policymaking.” Labour Market and Social Policy Occasional Paper No. 36, OECD, Paris. Jewell, T., J. Lee, M. Tieslau, and M.C. Strazicich (2003) “Stationarity of Health Expenditures and GDP: Evidence from Panel Unit Root Tests with Heterogeneous Structural Breaks”. Journal of Health Economics 22, 313-323. Johansen, S. (1995a) Likelihood-based Inference in Cointegrated Vector Auto-regressive Models. Oxford: Oxford University Press. Johansen, S. (1995b) “A Statistical Analysis of Cointegration for I(2) Variables.” Econometric Theory 11, 25-29. Kee, G.-S. (2001) “An Empirical Analysis of Canadian Public Health Care Spending and Health: 1975 to 1996.” Master’s Thesis, Calgary, University of Calgary. Leacy, F.H., ed. (1983) Historical Statistics of Canada. Ottawa: Statistics Canada, Catologue 11-516-XIE. Available on the internet at http://www.statcan.ca:80/english/freepub/11-516-XIE/free.htm . Lise, Jeremy (2000) “Changes in Life Expectancy and Mortality Rates: 1926-1966.” Ottawa: Health Canada, Applied Research and Analysis Directorate, Information, Analysis and Connectivity Branch, March 28. Maddala, G.S., and I.-M. Kim (1998) Unit Roots, Cointegration, and Structural Change. Cambridge: Cambridge University Press. McCoskey, S.K., and T.M. Selden (1998) ‘Health Care Expenditures and GDP: Panel Data Unit Root Test Results.” Journal of Health Economics 17, 369-376. Morrison, Donald F. (1967) Multivariate Statistical Methods. New York: McGraw-Hill Book Company. Ng, S. and P. Perron (2001) “Lag length Selection and the Construction of Unit Root Tests with Good Size and Power.” Econometrica 69(6), 1519-1554. Okunade, A.A., and M.C. Karakus (2001) “Unit Root and Cointegration Tests: Timeseries versus Panel Estimates for International Health Expenditure Models.” Applied Economics 33, 1131-1137. 14 Or, Z. (2000a) “Exploring the Effects of Health Care on Mortality across OECD Countries.” OECD Occasional Papers 46, Paris, Organisation for Economic Cooperation and Development. Or, Z. (2000b) “Determinants of Health Outcomes in Industrialised Countries: a Pooled, Cross-Country, Time-Series Analysis.” OECD Economic Studies No.30, Paris, Organisation for Economic Cooperation and Development. Perron, P., and G. Rodríguez (2003) “GLS Detrending, Efficient Unit Root Tests and Structural Change.” Journal of Econometrics, in press. Rahbek, A. H.C. Kongsted, and C. Jørgensen (1999) “Trend Stationarity in the I(2) Cointegration Model.” Journal of Econometrics 90, 265-289. Reimers, H.E. (1992) “Comparisons of Tests for Multivariate Cointegration.” Statistical Papers 33, 335-359. Thornton, J. (2002) “Estimating a Health Production Function for the US: Some New Evidence.” Applied Economics 34, 59-62. 15 Data Appendix 1. The data for Age-Standardized mortality rate per 100,000 population comes out of the Statistics Canada’s Health Indicators 1999 CD-ROM. 2. The data source for Infant Mortality Rate for 1921 and 1990 is the Selected Mortality Statistics, Canada, 1921-1990, Catalogue 82-548, while the data source for 1990 to 1999 is Cansim II table 102-0030, Statistics Canada. 3. The Perinatal Mortality Rate data was taken from the Selected Infant Mortality and Related Statistics, Canada 1921-1990, Catalogue 82-549 for 1921 to 1990, while the data source for 1990 to 1999 is the Statistics Canada’s Health Indicators 1999 CD-ROM. 4. Because the data for Life Expectancy going back to 1920 is only presented for fiveyear intervals, life expectancy for Canada used in this article was computed using internal calculations on a yearly basis.12 Calculations were made using data on death rates and population numbers provided by Statistics Canada’s Life Tables. 5. Total health expenditures uses data from the 1945 to 1975 series B513, Total Health Expenditures, of Statistics Canada’ Historical Statistics and from the 1975 to 1999 series Total Health Expenditures from a publication13 of the Canadian Institute for Health Information (CIHI). 6. Public health expenditures used the following data sources: a) Series H307, All governments, gross general expenditure on health from Statistics Canada’s Historical Statistics, 1965 to 1975 b) Series H150, All governments, net general expenditures on health, also from the Historical Statistics, 1945 to 1969 c) Series Total Public Sector Health Expenditures from the CIHI publication14, 1975 to 1999 7. Total population is the result of merging three series: a) Series A1, from Statistics Canada’s Historical Statistics , 1926 to 1961 b) Population series from the Statistics Canada’s Health Indicators 1999 CD-ROM, 1961 to 1970 c) Series V466668, Total population, from Cansim II Table 051-0001, Statistics Canada, 1971 to 2000 12 The authors would like to thank Allan Pollock, economist at Finance Canada, Economic Studies and Policy Analysis Division, for computing these numbers. 13 National Health Expenditures Trends, 1975-2001._ Canadian Institute for Health Information, Ottawa, 2001, p.77, Table A.2.1. 14 National Health Expenditures Trends, 1975-2001._ Canadian Institute for Health Information, Ottawa, 2001, p.77, Table A.2.1. 16 8. Implicit price index for government current expenditure uses data from the price index available through Statistics Canada’s Historical Statistics (1945 to 1975) and the price index available through CIHI’s publication15 (1975 to 1999). 9. GDP data was taken from Finance Canada’s economic forecasting model. This GDP measure is equal to Statistics Canada’ Series V1992067, Gross Domestic Product at market prices, from Cansim II Table 380-0002. 8. GNP uses the following data sources: a) Series F13, Gross National Product at market prices, from Statistics Canada’ Historical Statistics, 1926 to 1975 b) Series V499688, Gross National Product at market prices, from Cansim II Table 380-0015, 1961 to 1999. 9. GNP and GDP’s price deflator uses data from Series K172, Implicit Price Indexes of Gross National Expenditures at market prices, from Statistics Canada’ Historical Statistics (1926 to 1975) and from Series V1997756, Implicit Price Indexes, Gross Domestic Product at market prices from Cansim II Table 380-0003 (1961 to 1975). 15 National Health Expenditures Trends, 1975-2001._ Canadian Institute for Health Information, Ottawa, 2001, p.B-1, Table B.1. 17 Figure 1 Infant Mortaility Rate, Perinatal Mortaility Rate, Age-Standardized Mortality Rate, Life Expectancy at 65 and Life Expectancy at birth , Canada, 1950 to 1997 (1950=100) 210 190 IMR ASMR PMR LEB LE65 170 150 130 110 90 1950 1955 1960 1965 1970 1975 1980 1985 1990 1995 Figure 2 Infant Mortality Rate, Perinatal Mortality Rate, Life Expectancy at Birth and Life Expectancy at 65, Canada, 1926 to 1997 (1926=100) 210 190 170 IMR PMR LEB LE65 150 130 110 90 1926 1930 1934 1938 1942 1946 1950 1954 1958 1962 1966 1970 1974 1978 1982 1986 1990 1994 18 Figure 3 Summary Indicator of Health Status for Canada, 1950 to 1997 160 150 140 130 Summary indicator 120 110 100 90 1950 1954 1958 1962 1966 1970 1974 1978 1982 1986 1990 1994 Figure 4 Public/Private Health Expenditures, Real per Capita, Age-Adjusted, (1975 dollars), Canada, 1976 to 2001 14,000 12,000 8,000 Public Sector Private Sector 6,000 4,000 2,000 0 19 76 19 77 19 78 19 79 19 80 19 81 19 82 19 83 19 84 19 85 19 86 19 87 19 88 19 89 19 90 19 91 19 92 19 93 19 94 19 95 19 96 19 97 19 98 19 99 20 00 20 01 (In 1975$ ) 10,000 19 Figure 5 Total Real Health Expenditures per Capita, (1997 dollars), Canada, 1945 to 1999 3,500 3,000 (In 1997$) 2,500 2,000 1,500 1,000 500 0 1945 1950 1955 1960 1965 1970 1975 1980 1985 1990 1995 Figure 6 Real GNP per Capita and Real GDP per Capita, 1997 dollars, Canada 1926 to 2000 35,000 30,000 20,000 Real GNP per Capita Real GDP per Capita 15,000 10,000 5,000 0 19 26 19 29 19 32 19 35 19 38 19 41 19 44 19 47 19 50 19 53 19 56 19 59 19 62 19 65 19 68 19 71 19 74 19 77 19 80 19 83 19 86 19 89 19 92 19 95 19 98 (In 1997 dollars) 25,000 20 21 Table 1. Unit root test results for Canada: Results of previous studies Study Unit root test Sample period Hansen and King (1996) Blomqvist and Carter (1997) McCoskey and Selden (1998) Gerdtham and Löthgren (2000) Okunade and Karakus (2001) ADF PP IPS ADF, IPS, KPSS ADF, PP, IPS ADF, IPS 1960-1987 1960-1991 1960-1987 1960-1997 I(0) I(1) I(0) I(1) I(1) I(1) I(1) I(1) 1960-1997 I(2) I(2), I(1) 1960-1997 I(1) I(1) Gerdtham and Löthgren (2002) Jewell et al. (2003) Order of integration HE GDP Im et al. 1960-1997 I(1) I(0) (2002) Only Hansen and King (1996), Blomqvist and Carter (1997), and Okunade and Karakus (2001) test explicitly for the order of integration by testing both first and second differences of the variables for unit roots. 22 Table 2. Results of unit root tests, 1960-1997 Variable k T ADF-GLS LGDP ∆ LGDP 0 0 37 36 -1.060 -4.154c LTHE ∆ LTHE ∆2 LTHE 1 1 2 36 35 33 -1.914 -1.789a -2.531b LPHE ∆ LPHE ∆2 LPHE 2 8 1 35 28 34 -1.016 -0.003 -7.146c LHS ∆ LHS ∆2 LHS 0 6 0 37 30 35 -1.382 0.065 -12.702c LASM ∆ LASM 1 1 36 35 -2.075 -4.414c LIMR ∆ LIMR ∆2 LIMR a significant at the 10% level b significant at the 5% level c significant at the 1% level 0 4 0 37 32 35 -1.116 -0.856 -10.551c 23 Table 3. Results of Johansen tests for cointegration, 1960-1997 H0 λTrace H0 λmax LGDP, LTHE, LASM k = 1, n = 37; constant and trend in cointegrating equations r=0 39.664a r=0 21.381a 18.282 r=1 12.586 r≤1 5.697 r=2 2.697 r≤2 LGDP, LTHE k = 1, T = 37; constant and trend in cointegrating equation r=0 19.498 r=0 3.177 r=1 r≤1 16.321 3.177 LGDP, LTHE k = 1, T = 37; constant, no trend in cointegrating equation r=0 19.312b r=0 a 3.016 r=1 r≤1 16.296b 3.016a LGDP, LASM k = 2, T = 36; constant and trend in cointegrating equation r=0 19.498 r=0 3.177 r=1 r≤1 16.321 3.177 LASM, LTHE k = 3, T = 35; constant and trend in cointegrating equation r=0 19.498 r=0 r=1 3.177 r≤1 a significant at the 10% level b significant at the 5% level c significant at the 1% level 24 16.321 3.177 Table 4. Results of unit root tests, 1950-1997 Variable k T ADF-GLS LGDP ∆ LGDP ∆2 LGDP 1 9 0 46 37 45 -1.566 -0.924 -8.643c LTHE ∆ LTHE ∆2 LTHE 0 7 0 47 39 45 -1.063 -1.532 -10.817c LHS ∆ LHS ∆2 LHS 1 6 0 46 40 45 -1.599 -0.980 -16.422c LASM ∆ LASM ∆2 LASM 1 7 0 46 39 45 -1.808 -0.641 -16.067c LIMR ∆ LIMR ∆2 LIMR a significant at the 10% level b significant at the 5% level c significant at the 1% level 0 5 0 47 41 45 -1.432 -0.666 -10.689c 25 Table 5. Results of unit root tests, 1926-1999 Variable k T ADF-GLS LGNP ∆ LGNP 1 4 72 68 -3.566b -3.266 c LIMR ∆ LIMR ∆2 LIMR a significant at the 10% level b significant at the 5% level c significant at the 1% level 4 8 0 69 64 71 -1.627 -0.634 -16.816c 26
 0
0
advertisement


Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users