Experimental Eye Research 79 (2004) 75–83
www.elsevier.com/locate/yexer
Functional evaluation of retina and optic nerve in the rat
model of chronic ocular hypertension
Sinisa D. Grozdanica,b,*, Young H. Kwond, Donald S. Sakaguchib,c,
Randy H. Kardond, Ioana M. Soneab
a
Department of Veterinary Clinical Sciences, College of Veterinary Medicine, Iowa State University, Ames, IA 50011, USA
b
Department of Biomedical Sciences, College of Veterinary Medicine, Iowa State University, Ames, IA 50011, USA
c
Department of Zoology and Genetics, Iowa State University, Ames, IA 50011, USA
d
Department of Ophthalmology and Visual Sciences, University of Iowa Hospitals and Clinics, Iowa City, IA 52242, USA
Received 7 August 2003; accepted in revised form 20 February 2004
Abstract
Purpose. To functionally characterize the rat retina and optic nerve after chronic elevation of the intraocular pressure (IOP) using
electroretinography (ERG) and computerized pupillometry.
Methods. Chronic elevation of the IOP was induced in Brown Norway rats by combined injection of indocyanine green dye (ICG) into the
anterior chamber and diode laser treatment, followed by ERG and pupil light reflex (PLR) monitoring.
Results. Laser treatment induced significant elevation of the IOP in operated eyes for 6 weeks, with maximal values observed 14 days
postoperatively (ctrl ¼ 18·4 ^ 2·4 and operated ¼ 35 ^ 8·4 mmHg; mean ^ SD ). Preoperative values for the PLRratio were 68·5 ^ 4%
(mean ^ SEM ; %). Three days postoperatively the PLRratio decreased to 60·3 ^ 10·3%, but was not significantly different compared to
preoperative values (p . 0·05; Kruskal-Wallis non-parametric test with Dunn’s post-test). However, 7, 14 and 21 days postoperatively the
PLR function dramatically decreased to 14·6 þ 8·6, 11·5 ^ 6·7 and 12·6 ^ 4%, respectively, and was significantly smaller compared to
preoperative values ðp , 0·01Þ: At day 28 the PLR significantly recovered and was not significantly different compared to preoperative
values (PLRratio ¼ 38·5 ^ 8·6, p . 0·05). However, 35 days after surgery the PLR started to decrease once again in the operated eyes
(PLRratio ¼ 17·2 ^ 7·4%) and was significantly smaller again compared to preoperative values ðp , 0·05Þ: The PLR values continued to
decrease until the end of experiment (60 days postoperatively). ERG analysis of operated eyes revealed significantly decreased amplitudes of
a- and b-waves 10d postoperatively, while oscillatory potentials (OPs) and flicker ERG (flERG) amplitudes were not detectable. However, 28
days postoperatively OPs significantly, but temporarily recovered, while a-wave, b-wave and flERG amplitudes did not significantly change
compared to values observed 10d postoperatively. The ERG analysis of the operated eyes revealed significantly reduced amplitudes 60 days
postoperatively. Histological analysis revealed degeneration of all retina layers and optic nerve axons.
Conclusions. Chronic ocular hypertension in rats produces dramatic damage to all retinal layers and optic nerves observed by
morphological and functional methods which significantly correlate with the IOP elevation. Outer retina of glaucomatous rats seems to be
more susceptible to the damage due to chronic elevation of the IOP. Chronic hypertensive rat eyes have capacity to temporarily recover
function of the inner retina and optic nerve.
q 2004 Elsevier Ltd. All rights reserved.
Keywords: animal model; electroretinography; glaucoma; pupils; tonometry
1. Introduction
A better understanding of the pathophysiology of
glaucoma depends on the precise correlation of molecular
* Corresponding author. Dr Sinisa D. Grozdanic, Department of
Veterinary Clinical Sciences, College of Veterinary Medicine, Iowa State
University, Ames, IA 50011, USA.
E-mail address: sgrozdan@iastate.edu (S.D. Grozdanic).
0014-4835/$ - see front matter q 2004 Elsevier Ltd. All rights reserved.
DOI:10.1016/j.exer.2004.02.011
events and in vivo changes of the retina and optic nerve
function during the progression of the disease. Rodents (rats
and mice) have become important models for studying
glaucoma due to availability of genomic and proteomic
data, potential for use of transgenic animals, cost and ease of
maintenance (Goldblum and Mittag, 2002). Morphological
and molecular data from different rodent models which
mimic some of the glaucomatous changes significantly
76
S.D. Grozdanic et al. / Experimental Eye Research 79 (2004) 75–83
improved the amount of information about potential causes
of the retinal ganglion cell (RGC) death (Johnson et al.,
2000; Garcia-Valenzuela et al., 1995; Levkovitch-Verbin
et al., 2000; Mittag et al., 2000).
Currently, estimation of the damage in the experimental
rat models of the chronic ocular hypertension is typically
evaluated by histological or immunocytochemical analysis
after the experimental animal is euthanized. Several recent
studies described some of the electroretinographic properties of chronically hypertensive rat eyes (Mittag et al., 2000;
Bayer et al., 2001; Chauhan et al., 2002; Grozdanic et al.
2003b) and there is only one study (Grozdanic et al. 2003b)
that tried to evaluate function of the optic nerve in rodent
models of the chronic ocular hypertension. The morphological approach alone does not provide any information
about dynamics of the disease at different time points. The
principal goal of this study was to describe functional
responses (electroretinogram -ERG and pupil light reflexPLR) of rat eyes after laser-induced chronic elevation of the
intraocular pressure (IOP). Since monitoring of the PLR
reflects the combined function of the retina and optic nerve,
we were interested to use electroretinography (ERG) as an
additional method to evaluate if damage occurred in
different retinal layers besides the RGC layer. The functional
monitoring of the retina and optic nerve might provide
important information about changes observed in rodent
experimental models of chronic ocular hypertension before
occurrence of significant morphological changes observed
by light microscopy. Furthermore, the possibility to monitor
functional responses in the same animal at various time
points might provide valuable data about dynamics of the
damage caused by chronic ocular hypertension.
2. Materials and methods
2.1. Laser-induction of chronic ocular hypertension
All animal studies were conducted in accordance with
the ARVO Statement for Use of Animals in Ophthalmic and
Vision Research, and procedures were approved by the Iowa
State University Committee on Animal Care. Adult Brown
Norway rats (6 – 8 months of age, n ¼ 27) were used for
experiments. Rats were kept under 12 hr of light and 12 hr
of dark regimen.
Briefly, rats were anesthetized with 2·5%
isoflurane þ 100% oxygen; body temperature was maintained with use of a heating pad. Indocyanine green (10 ml,
10 mg ml21; Sigma, St Louis, MO, USA) was injected into
the anterior chamber of the eye at a very slow rate using a
Hamilton syringe attached to a microinjector pump to avoid
abrupt elevation of the IOP due to the procedure. Animals
were pretreated with 4% pilocarpine hydrochloride eye
drops, to increase an outflow of the dye into the trabecular
meshwork and episcleral veins. The pilocarpine treatment
also caused miosis, which served to protect the posterior
pigmented structures of the eye from the diode laser energy
(the pigmented iris served as a barrier for any potential stray
energy). Twenty minutes post-injection, a diode laser
(DioVet, Iridex Corporation, Mountain View, CA, USA)
was used to externally deliver 810 nm energy pulses through
a 50 mm fiberoptic probe to the region of the trabecular
meshwork and episcleral veins in close proximity to the
limbal region (Fig. 1). Careful positioning of the fiberoptic
probe insured that the orientation of the laser was away from
the pigmented structures of the retina. We delivered
between 50 and 60 laser spots through a 3008 range of the
limbal radius (350 mW energy, 1500 ms pulse time) in 18
rats. In order to examine whether is possible to manipulate
the elevation of IOP, additional 9 rats was operated with a
same distribution of the laser spots (50 spots, 300 degrees
range) but with significantly smaller amount of the applied
laser energy (300 mW, 400 ms pulse time). After surgery,
pain was controlled by acetaminophen (100 mg kg21) þ
codeine (75 mg kg21) in the drinking water for 7 days. To
prevent potential infection, antibiotic ointment
(neomycin þ polymyxin B þ bacitracin; Bausch and
Lomb Pharmaceuticals Inc; Tampa, FL, USA) was applied
topically after the procedure. Seven rats were euthanized in
the first 2 weeks after surgery due to either development of
the corneal ulcer ðn ¼ 3Þ; which prevented accurate IOP
measurement, or from rupture of the limbus ðn ¼ 4Þ due to
very high elevation of the IOP (. 50 mmHg).
2.2. Intraocular pressure monitoring
IOP was measured with a hand-held tonometer (Tonopen
XL, Mentor, Norwell, MA, USA). A calibration of the
Tonopen was performed by comparing IOP results measured
using invasive manometry as we previously described
(Grozdanic et al., 2002). Readings from the manometer
and Tonopen were obtained simultaneously and a regression
line was calculated (y ¼ 7·3029 ^ 0:7015x; r 2 ¼ 0·78).
Tonopen recordings were obtained preoperatively from
both eyes and from non-operated (control) and operated
eyes on days 3, 7, 14, 21, 28, 35, 42 and 60 postoperatively.
2.3. Computerized pupillometry
The PLR was evaluated with a custom-made computerized pupillometer (University of Iowa, Iowa City, IA, USA)
preoperatively and on days 3, 7, 14, 21, 28, 35, 42 and 60
postoperatively as we previously described (Grozdanic et al.,
2002a,b,c). Briefly, animals were anesthetized initially
with 4% halothane, 30% N2O and 70% O2. A light
plane of anesthesia was maintained with 1% halothane,
30% N2O and 70% O2 to avoid suppression of the PLR
response caused by the use of higher doses of anesthetic.
A one channel computerized pupillometer was used
to record the movement of the pupil from the control
(non-operated) eye, while a computer-controlled stimulus
light (light emitting diodes) was alternately turned on in front
S.D. Grozdanic et al. / Experimental Eye Research 79 (2004) 75–83
77
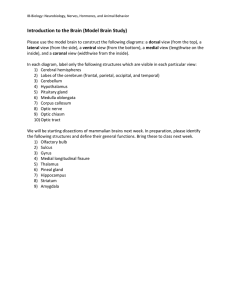
Fig. 1. Laser treatment of the indocyanine green injected eyes caused complete destruction of the trabecular meshwork without damaging peripheral retina.
(A) control eye (10 £ ) (B) operated eye (10 £ ) (C) control eye (20 £ ) (D) operated eye (20 £ ) (arrow-trabecular meshwork, ac, anterior chamber; l, lens;
pc, posterior chamber; cb, cilliary body; ret, retina).
of the control or operated eye (on time ¼ 0·2 s, off time ¼ 5
sec). The stimulus light intensities used were: 45·8, 82, 153
and 300 cd m22. A custom made software routine (Winnana
Software, University of Iowa, Iowa City, IA, USA) was used
to analyze the recorded tracings of the pupil movements in
response to light stimuli and to objectively determine the
timing and amplitude of the pupil reflex responses.
2.4. Electroretinography
To quantify potential damage to the retina due to chronic
elevation of the IOP, a simultaneous recording of electroretinogram from both eyes (control and operated) was
performed 10, 28 and 60 days post-operatively as previously
described (Grozdanic et al., 2002). Briefly, animals were
dark adapted for at least 6 hr. A Neuropack-MEB 7102
Evoked Potential Measuring System (Nihon-Kohden
America, Foothill Ranch, CA, USA) was used to deliver a
triggered output to the flash stimulator and collect signals
from both eyes. A flash ERG routine was delivered at a
0·2 Hz frequency (10 averaged signals per recording session,
sensitivity 100 mV mg division21 , low-cut frequency
0·5 Hz, high-cut frequency 10 kHz, analysis time 500 ms).
Oscillatory potentials (OPs) were recorded by delivering
light stimuli at a 0·2 Hz frequency (10 averaged signals per
recording session, sensitivity 100 mV mg division21, lowcut frequency 50 Hz, high-cut frequency 500 Hz, analysis
time 100 ms). Isolated cone responses were recorded from
previously light adapted eyes by delivering stimuli at 20 Hz
(50 averaged signals per recording session, sensitivity
50 mV mg division21, low-cut frequency 0·5 Hz, high-cut
frequency 10 kHz, analysis time 500 ms). To avoid potential
bias due to electrode differences, recordings were repeated
with electrodes switched to the opposite eyes.
Amplitudes and latency times for the scotopic flash ERG
a-wave were determined as difference between flash onset
and the most negative component of the tracing preceding bwave (a-wave spike) and for the b-wave as difference
between a-wave spike and b-wave spike as we previously
described (Grozdanic et al., 2002).
2.5. Histological examination
Sixty five days postoperatively, rats were deeply anesthetized with a high dose of phenobarbitol (100 mg kg21) and
perfused intracardially with ice-cold heparinized saline
followed by 4% paraformaldehyde/2% glutaraldehyde in
phosphate buffer (pH 7·4). The eyes and optic nerves were
harvested. Optic nerves were dissected and 3 mm thick
segments obtained 1 mm posterior to the globe were rinsed
in cacodylate buffer and postfixed in 2% osmium tetroxide
in cacodylate buffer, dehydrated in alcohol and embedded in
epoxy resin. Cross sections (1 mm thick) were cut with an
ultramicrotome, mounted on glass slides, and stained with
1% toluidine blue. Eye globes were paraffin embedded, and
7 mm thick sections of the retina were collected onto
poly-L -lysine coated glass slides, and stained with hematoxylin and eosin. Tissue sections were examined with a Nikon
Microphot FXA photomicroscope (Nikon Corporation, New
York, NY, USA). Images were captured using a Kodak
78
S.D. Grozdanic et al. / Experimental Eye Research 79 (2004) 75–83
The measurement of the PLR was used as an assay to
investigate development of deficits in the retina and optic
nerve function following a laser-induced chronic elevation of
the IOP. Damage to the retina or optic nerve reduces the
amplitude of the pupil contraction to light. Since the motor
output of the neuronal reflex of pupil contraction to light is
distributed to both pupils (although more output goes to
the pupil of the stimulated eye in Brown Norway rats
(Grozdanic et al., 2002)), monitoring the pupil from just the
non-operated eye is sufficient to assess any asymmetry of
light input between the operated and non-operated eye. All
pupil parameters were calculated by comparing values from
stimulation of the operated and non-operated (control) eyes
in the same animal. Chronic ocular hypertension induced
afferent defects of all PLR components (amplitude, latency
time and velocity) in all operated animals (Figs. 3, 4, 5 and 6).
Preoperative values for the PLRratio (ratio ¼ indirect/
direct PLR, Fig. 3) were 68·5 ^ 4% (mean ^ SEM ; %).
Three days postoperatively the PLRratio decreased to
60·3 ^ 10·3%, but was not significantly different compared
to preoperative values (p . 0·05; Kruskal – Wallis nonparametric test with Dunn’s post-test, Fig. 3). However, 7
days postoperatively the PLR function dramatically
decreased to 14·6 þ 8·6% and was significantly smaller
compared to preoperative values ðp , 0·01Þ: Fourteen days
postoperatively, the PLR function further decreased to
11·5 ^ 6·7% ðp , 0·01Þ and 21 days postoperatively the
PLRratio was 12·6 ^ 4% ðp , 0·05Þ: At day 28 the PLR
significantly improved and was not significantly different
compared to preoperative values (PLRratio ¼ 38·5 ^ 8·6%,
p . 0·05; Kruskal –Wallis non-parametric test with Dunn’s
post-test, Figs. 3 and 4). However, 35 days after surgery the
PLR started to decrease once again in the operated eyes
(PLRratio ¼ 17·2 ^ 7·4%) and was significantly smaller
again compared to preoperative values ðp , 0·05Þ: The
PLRratio continued to decrease and was 9·5 ^ 7·3% (42d
postoperatively; p , 0·01) and was 4·2 ^ 4·2% at the last
recording time point (60d postoperatively, p , 0·001).
Detailed analysis of tonometry and pupillometry data
revealed significant correlation between ocular hypertension
expressed as a coefficient of IOP elevation and PLR
amplitude deficits ((IOPoperated eyes 2 IOPcontrol eyes) £
Fig. 2. Tonometry analysis of the laser-operated eyes. An elevation of the
IOP revealed the peak values 14 days after surgery, however, IOP values
started to decrease after 14 days and completely normalized 60 days after
surgery. Symbols represent mean values ^ SEM (* for p , 0·05; *** for
p , 0·001).
Fig. 3. Temporary recovery of the PLR. At day 28 the PLR displayed
significant recovery but function started to decrease again at 35 days
postoperatively. Black line connects median values for each group, symbols
represent individual animals (light stimulus ¼ 300 cd/m22).
Megaplus Camera (Model 1·4; Kodak Corp, San Diego, CA,
USA) connected to a MegaGrabber Framegrabber in a
Macintosh 8100/80 AV computer (Apple Computer,
Cupertino, CA, USA) using NIH Image 1·58 VDM software
(W. Rasband, NIH, Bethesda, MD, USA).
2.6. Statistical analysis
Statistical analysis was performed by using Paired t-test
and Kruskal – Wallis non-parametric test with Dunn’s posttest (as indicated in the text) with the GraphPad (GraphPad,
San Diego, CA, USA) software. A p value of , 0·05 was
considered significant.
3. Results
3.1. Tonometry
Laser cauterization of the indocyanine green pretreated
eyes proved to be a successful procedure for the induction of
chronic elevation of the IOP in rat eyes. The IOP was
significantly elevated in all operated rats after laser-induced
surgery compared to control (non-operated) eyes (Fig. 2).
3.2. Assessment of optic nerve function using the pupil
light reflex
S.D. Grozdanic et al. / Experimental Eye Research 79 (2004) 75–83
79
velocity (p ¼ 0·0014; Kruskal –Wallis non-parametric test)
and increase in the latency time (p ¼ 0·0001; Kruskal –
Wallis non-parametric test) after stimulation of the
operated eye compared to the stimulation of the nonoperated (control) eye (Fig. 5). Velocity and latency
followed the pattern of recovery detected when PLR
amplitudes were analyzed and temporary recovered 28
days postoperatively.
3.3. Electroretinography
Fig. 4. Original tracings from one of the rats that displayed a temporary
recovery of pupil light reflex function. Function started to recover 21 days
postoperatively, reached a peak of recovery on 28 days postoperatively,
and then started to decline. 60 days after surgery pupil light reflex was not
present after stimulation of the operated eye (I, indirect PLR: operated
eye stimulated while control eye monitored; D, direct PLR: control eye
stimulated and monitored; arrow-detectable indirect PLR; black box-light
stimulus 300 cd m22, 0·2 sec).
duration of hypertension (mmHg £ days) vs. PLR amplitudes expressed as a ratio (operated/control, %)):
r 2 ¼ 0·2; p , 0·0001:
We analyzed latency time and velocity of the PLR in
operated eyes and detected significant decrease of the PLR
ERG was used to evaluate the functional status of the
inner and outer retina. To evaluate the effect of the chronic
elevation of the IOP on different populations of retinal cells
we used full field scotopic flash ERG, full field scotopic
oscillatory potentials and photopic flicker ERG (flERG).
Chronic elevation of the IOP caused significant reduction of
electroretinographic activity (Figs. 6 and 7).
Electroretinographic analysis of operated eyes revealed
dramatic decrease of a- and b-wave amplitudes and
complete loss of OPs and flERG amplitudes 10 days
postoperatively (Fig. 7(A)): a-wave ¼ 21· ^ 6·2% (data are
represented as a ratio ¼ operated/control; mean ^ SEM , %),
b-wave ¼ 13·5 ^ 2·6, OPs ¼ 0 and flERG ¼ 0%. However,
28 days postoperative OPs amplitudes showed significant
improvement of function (OPs ¼ 7·6 ^ 2·2%; 7/11 rats)
while a-wave amplitudes (10·1 ^ 1·8%) continued to
decrease. The b-wave (13·3 ^ 3·8%) and flERG amplitudes
(0%) did not significantly change compared to the values
observed 10 days postoperatively.
Sixty days after surgery OPs and flERG amplitudes were
non-detectable in all operated rats, while a-wave
(8·9 ^ 2·7%) and b-wave amplitudes (7·8 ^ 2·6%) further
decreased.
Fig. 5. Pupil light reflex velocity and latency time data (B) Twenty eight days postoperatively, velocity deficits recovered and were not significantly different
comparing to preoperative values (p . 0·05; Kruskal–Wallis non-parametric test with Dunn’s post-test, n ¼ 11). (A) The latency deficits (interocular
difference in between latency times the direct and indirect PLR) followed a similar pattern of recovery 28 days postoperatively (p . 0·05; Kruskal–Wallis
non-parametric test with Dunn’s post-test). * p , 0·05; ** p , 0·01; *** p , 0·001:
80
S.D. Grozdanic et al. / Experimental Eye Research 79 (2004) 75–83
Fig. 6. Electroretinographic characteristics from one rat with chronic elevation of the IOP which displayed temporary recovery of OPs 28 days postoperatively
and improvement of the latency time for the a- and b-wave. Left panel represents ERG tracings from the scotopic flash condition, middle panel shows
oscillatory potentials (L1-L5), and right panel shows photopic flicker ERG, photopic flERG amplitudes were not detectable postoperatively. Scotopic flash
ERG: L1, flash onset; L2, the peak a-wave point; L3, the peak b-wave point, L1–L2, latency time for a-wave; L1–L3, latency time for b-wave; Scotopic OPs:
L1, flash onset; L1– L2, latency time for OPs.
3.4. Histological analysis
Light microscopy analysis revealed the reduction of the
cellular organization of all retinal layers and reduced
thickness compared to control (non-operated) eyes, which
suggests that chronic ocular hypertension damaged both
inner and outer retina structures (Fig. 8).
Detailed analysis of the optic nerve cross sections
revealed primary degeneration and swelling of large
diameter axons (Fig. 9). Semi-quantitative analysis, performed as previously described (Johnson et al., 2000),
revealed significantly greater grade of optic nerve histological damage of operated eyes compared to control (nonoperated) eyes: control ¼ 1; operated ¼ 2·24 ^ 0·3
(p ¼ 0·02; Paired t-test). Detailed analysis of tonometry
and optic nerve morphometry data revealed significant
correlation between ocular hypertension expressed as a
coefficient of IOP elevation and optic nerve damage
((IOPoperated eyes-IOPcontrol eyes) £ duration of hypertension
(mmHg £ days) vs. optic nerve damage grade: r 2 ¼ 0·43;
p , 0·05:
4. Discussion
Evidence from the experimental animal models of
glaucoma imply that retinal ganglion cells die in a slow
manner via apoptosis (Quigley, 1999). In order to achieve a
better understanding of the glaucomatous pathology, and
eventually develop new strategies for the protection of the
optic nerve from glaucomatous neuropathy, it is essential to
develop animal models and adequate tools for the in vivo
monitoring of function during progression of the disease.
The experimental approach used in this study allowed us
to monitor dynamics of the retina and optic nerve damage
Fig. 7. The dynamics of the full field flash ERG, OPs and flERG (A) OPs
followed dynamics of the PLR recovery (ratio for rats w/o detectable
response was calculated as zero, ratio for healthy (non-operated) rats for all
tested parameters was around 100%-data not shown) The OPs significantly
increased from10 days to 28 days postoperatively (***p , 0·001) (B)
Latency time at post-op time points were significantly longer compared to
the control, non-operated eyes (32d: a-wave latency p ¼ 0·02; b-wave
latency p ¼ 0·03; 42d: a-wave latency p ¼ 0·007; b-wave latency p ¼
0·024; Paired t-test). Bar ¼ mean ^ SEM .
S.D. Grozdanic et al. / Experimental Eye Research 79 (2004) 75–83
81
Fig. 8. Chronic ocular hypertension induced histological degeneration of retinas. Histological examination of the operated eyes revealed decreased thickness of
all retinal layers. (A) Control eye; (B) Central retina from one of the rats which had 40% deficits in ERG amplitudes; (C), Central retina from one of the rats
which did not have detectable ERG responses: inner retina neurons are completely absent, outer segments of the photoreceptors are damaged and thickness of
the outer nuclear layer is decreased (GCL, ganglion cell layer; IPL, inner plexiform layer; INL, inner nuclear layer; OPL, outer plexiform layer; ONL, outer
nuclear layer, OS, outer segments, RPE, retinal pigment epithelium; bar ¼ 100 mm).
during chronic elevation of the IOP. Laser cauterization of
the indocyanine green pretreated eyes proved to be a
successful procedure for the induction of chronic elevation
of the IOP in rat eyes for approximately 42 days.
We previously demonstrated that monitoring and analysis of the PLR and ERG parameters are very effective
strategies for the functional monitoring of different cell
populations in the retina of rats with acute (Grozdanic et al.,
2003a) and chronic ocular hypertension (Grozdanic et al.,
2003b). In this study we showed that the PLR and inner
retinal functional parameters (OPs, b-wave) are most
dramatically affected. However, chronic ocular hypertension also showed a significant effect on photoreceptor
function, which is in agreement with previous results from
the mouse (Bayer et al., 2001; Grozdanic et al., 2003c) and
rat models (Grozdanic et al., 2003b) of the chronic ocular
hypertension. Interestingly, morphological and functional
deficits of the outer retina were also described in
glaucomatous human (Panda and Jonas, 1992; Nork et al.,
2000) and monkey eyes (Nork et al., 2000; Raz et al., 2003).
However, two studies which evaluated morphology of
glaucomatous patients and monkeys with experimental
glaucoma did not demonstrate significant loss of the
photoreceptors (Kendell et al., 1995; Wygnanski et al.,
1995).
One intriguing finding of this study was detection of the
transient, but significant recovery of the OPs and PLR
function in some of the operated animals at approximately
28 days postoperatively. We recently reported the similar
timing of temporary recovery of the PLR function in a rat
model of the acute ocular ischemia (Grozdanic et al., 2003a)
and also demonstrated spontaneous capability of rat retinas
and optic nerves to functionally recover after chronic ocular
hypertension (Grozdanic et al., 2003b). Taken together,
these data raise a number of provocative questions about the
existence of potential mechanisms which may act to rescue
the function of the inner retina and optic nerve. A partial or
complete recovery of visual function in patients with optic
neuritis is a well recognized phenomena, but is almost
exclusively correlated with the resolution of the optic nerve
oedema (Nikoskelainen, 1975; Dunker and Wiegand, 1996;
Brady et al., 1999). Furthermore, temporary loss of visual
function has been described due to central retina artery
occlusion (Perkins et al., 1987), choroidal ischemia
Fig. 9. Chronic ocular hypertension induced histological degeneration of optic nerves. (A) Cross section analysis of the optic nerve sections revealed
degeneration and swelling of axons; (B) Images from the control (non-operated) optic nerve (bar ¼ 25 mm).
82
S.D. Grozdanic et al. / Experimental Eye Research 79 (2004) 75–83
Fig. 10. Titration of the laser energy corresponds to the elevation of the IOP and ERG deficits. (A) Application of decreased amounts (0·3 W, 0·4 sec pulse) of
the laser energy resulted in milder elevation of the IOP (IOP elevation is presented as IOP integral value ¼ (IOPoperated eyes 2 IOPcontrol eyes) £ duration of
hypertension). (B) Mild elevation of the IOP resulted in smaller but still significant ERG deficits (ERG amplitudes are presented as ratio% ¼ operated eye
amplitude/control eye amplitude).
(Kinyoun and Kalina, 1986), giant cell arthritis (Quillen
et al., 1993) or as a result of the intraretinal gray lesions due
to prolonged ophthalmic artery hypoperfusion (Cherny et al.,
1991). We cannot exclude the possibility that observed
changes in laser-treated rats were not the result of choroidal
ischemia or severe obstruction of the retinal circulation
since we observed dramatic deficits of the a-wave
amplitudes and latency time. However, lack of the recovery
of the a-wave, b-wave and flicker ERG amplitudes at the
time point (28 days postoperatively) when recovery of the
OPs and PLR function was observed might point to a
mechanism(s) which acts very selectively toward recovery
of specific cell populations (amacrine cells and RGCs). An
attractive hypothesis of temporary recovery of the amacrine
cells as the principal generators of OPs, and RGCs as
essential elements for the transmission of the PLR would be
specific up-regulation of different growth factors as
previously suggested (Wahlin et al., 2000). Indeed, Wahlin
et al. (2000) reported direct action of brain-derived
neurotrophic factor (BDNF), basic fibroblast growth factor
(FGF2) and ciliary neurotrophic factor (CNTF) on Müller
cells, amacrine cells and RGCs and identified these specific
cell types as primary targets for growth factor action.
Histological analysis revealed damage of all retinal
layers, however, the inner retina and optic nerve were the
most dramatically affected. We recently reported similar
type of changes in the laser-induced chronic ocular
hypertension in mice (Grozdanic et al., 2003c); however,
functional and morphological deficits were not as strongly
expressed as observed in this study. Histological and
morphological data strongly suggest that observed damage
was result of the ischemia which affected all retinal layers.
Fig. 11. Titration of the laser energy resulted in milder elevation of the IOP and relatively spared ERG function. Left panel represents ERG tracings from the
scotopic flash condition, middle panel shows oscillatory potentials (L1–L5), and right panel shows photopic flicker ERG. Mild elevation of the IOP resulted in
minimal a-wave deficits and moderate deficits of the b-wave, OP and flicker ERG amplitudes. Scotopic flash ERG: L1, flash onset; L2, the peak a-wave point;
L3, the peak b-wave point; L1–L2, latency time for a-wave; L1 –L3, latency time for b-wave; Scotopic OPs: L1, flash onset; L1–L2, latency time for OPs.
S.D. Grozdanic et al. / Experimental Eye Research 79 (2004) 75–83
Since we observed dramatic physiological and morphological changes of all retinal layers, we were interested
whether we can manipulate elevation of the IOP by
decreasing the strength and duration of the applied laser
energy and by these means create changes which would
mimic more closely changes observed in human glaucoma.
Decrease in the duration and energy of the laser pulse
proved to be an effective strategy to induce mild elevation of
the IOP followed by relatively small retinal deficits
observed by ERG (Figs. 10 and 11).
Simultaneous PLR and ERG monitoring proved to be
a useful and sensitive, non-invasive method for the
evaluation of the retina and optic nerve function. Since
strategies for the induction of damage due to chronically
elevated IOP usually involve surgery of one eye,
monitoring of the pupil parameters of the control, nonoperated eye, provided very precise information about
retinal and optic nerve functional integrity.
In order to better understand the pathological mechanisms which occur during chronic ocular hypertension and
evaluate potential success of neuroprotective strategies, it is
essential to use techniques which would be sensitive enough
to detect disruption of the retina and optic nerve function
even before occurrence of the cellular death.
Acknowledgements
The authors would like to thank John Morrison, Elaine
Johnson William Chepurna and Lijun Jia for help with optic
nerve sections analysis. This work was supported by a
Special Research Incentive Grant from the College of
Veterinary Medicine-Iowa State University, an InterInstitutional Grant from the College of Veterinary Medicine-Iowa
State University and the College of Medicine-University of
Iowa, The Glaucoma Foundation, NY, an unrestricted grant
from Research to Prevent Blindness (Depatment of Ophthalmology, University of Iowa), NY and a Merit Review Grant
from the Veterans Administration (R.H.K.). R.H.K. is also a
Lew Wasserman Scholar (Research to Prevent Blindness).
References
Bayer, A.U., Danias, J., Brodie, S., Maag, K.P., Chen, B., Shen, F., Podos,
S.M., Mittag, T.W., 2001. Electroretinographic abnormalities in a rat
glaucoma model with chronic elevated intraocular pressure. Exp. Eye
Res. 72, 667–677.
Bayer, A.U., Neuhardt, T., May, A.C., Martus, P., Maag, K.P., Brodie, S.,
Lütjen-Drecoll, E., Podos, S.M., Mittag, T., 2001. Retinal morphology
and ERG response in the DBA/2NNia mouse model of angle-closure
glaucoma. Invest. Ophthalmol. Vis. Sci. 42, 1258–1265.
Brady, K.M., Brar, A.S., Lee, A.G., Coats, D.K., Paysse, E.A., Steinkuller,
P.G., 1999. Optic neuritis in children: clinical features and visual
outcome. J AAPOS 3, 98–103.
Chauhan, B.C., Pan, J., Archibald, M.L., LeVatte, T.L., Kelly, M.E.,
Tremblay, F., 2002. Effect of intraocular pressure on optic disc
topography, electroretinography, and axonal loss in a chronic pressureinduced rat model of optic nerve damage. Invest. Ophthalmol. Vis. Sci.
43, 2969–2976.
83
Cherny, M., O’Day, J., Currie, J., 1991. Intraretinal gray lesions as a sign of
reversible visual loss following prolonged ophthalmic artery hypoperfusion. J. Clin. Neuroophthalmol. 11, 228–232.
Dunker, S., Wiegand, W., 1996. Prognostic value of magnetic resonance
imaging in monosymptomatic optic neuritis. Ophthalmology 103,
1768–1773.
Garcia-Valenzuela, E., Shareef, S., Walsh, J., Sharma, S.C., 1995.
Programmed cell death of retinal ganglion cells during experimental
glaucoma. Exp. Eye Res. 61, 33–44.
Goldblum, D., Mittag, T., 2002. Prospects for relevant glaucoma models
with retinal ganglion cell damage in the rodent eye. Vision Res. 42,
471– 478.
Grozdanic, S., Sakaguchi, D.S., Kwon, Y.H., Kardon, R.H., Sonea, I.M.,
2002. Characterization of the pupil light reflex, electroretinogram and
tonometric parameters in healthy rat eyes. Curr. Eye Res. 25, 69 –78.
Grozdanic, S., Sakaguchi, D.S., Kwon, Y.H., Kardon, R.H., Sonea, I.M.,
2003a. Functional characterization of retina and optic nerve after acute
ocular ischemia in rats. Invest. Ophthalmol. Vis. Sci. 44, 2597– 2605.
Grozdanic, S., Betts, D.M., Sakaguchi, D.S., Kwon, Y.H., Kardon, R.H.,
Sonea, I.M., 2003b. Temporary elevation of the intraocular pressure by
cauterization of vortex and episcleral veins in rats causes functional
deficits in the retina and optic nerve. Exp. Eye Res. 77, 27 –33.
Grozdanic, S., Betts, D.M., Sakaguchi, D.S., Allbaugh, R.A., Kwon, Y.H.,
Kardon, R.H., 2003c. Laser-induced mouse model of chronic ocular
hypertension. Invest. Ophthalmol. Vis. Sci. 44, 4337– 4346.
Johnson, E.C., Deppmeier, L.M., Wentzien, S.K., Hsu, I., Morrison, J.C.,
2000. Chronology of optic nerve head and retinal responses to elevated
intraocular pressure. Invest. Ophthalmol. Vis. Sci. 41, 431– 442.
Kendell, K.R., Quigley, H.A., Kerrigan, L.A., et al., 1995. Primary openangle glaucoma is not associated with photoreceptor loss. Invest.
Ophthalmol. Vis. Sci. 36, 200–205.
Kinyoun, J.L., Kalina, R.E., 1986. Visual loss from choroidal ischemia.
Am. J. Ophthalmol. 101, 650 –656.
Levkovitch-Verbin, H., Harris-Cerruti, C., Groner, Y., Wheeler, L.A.,
Schwartz, M., Yoles, E., 2000. RGC death in mice after optic nerve
crush injury: oxidative stress and neuroprotection. Invest. Ophthalmol.
Vis. Sci. 41, 4169–4174.
Mittag, T.W., Danias, J., Pohorenec, G., Yuan, H.M., Burakgazi, E.,
Chalmers-Redman, R., Podos, S.M., Tatton, W.G., 2000. Retinal
damage after 3 to 4 months of elevated intraocular pressure in a rat
glaucoma model. Invest. Ophthalmol. Vis. Sci. 41, 3451– 3459.
Nikoskelainen, E., 1975. Later course and prognosis of optic neuritis. Acta
Ophthalmol. (Copenh) 53, 273–291.
Nork, T.M., Ver Hoeve, J.N., Poulsen, G.L., et al., 2000. Swelling and loss
of photoreceptors in chronic human and experimental glaucomas. Arch
Ophthalmol. 118, 235–245.
Panda, S., Jonas, J.B., 1992. Decreased photoreceptor count in human eyes
with secondary angle-closure glaucoma. Invest. Ophthalmol. Vis. Sci.
33, 2532–2536.
Perkins, S.A., Magargal, L.E., Augsburger, J.J., Sanborn, G.E., 1987. The
idling retina: reversible visual loss in central retinal artery obstruction.
Ann. Ophthalmol. 19, 3–6.
Quigley, H.A., 1999. Neuronal death in glaucoma. Prog. Retin. Eye Res.
18, 39–57.
Quillen, D.A., Cantore, W.A., Schwartz, S.R., Brod, R.D., Sassani, J.W.,
1993. Choroidal nonperfusion in giant cell arteritis. Am. J. Ophthalmol.
116, 171–175.
Raz, D., Perlman, I., Percicot, C.L., et al., 2003. Functional damage to inner
and outer retinal cells in experimental glaucoma. Invest. Ophthalmol.
Vis. Sci. 44, 3675–3684.
Wahlin, K.J., Campochiaro, P.A., Zack, D.J., Adler, R., 2000. Neurotrophic
factors cause activation of intracellular signaling pathways in Muller
cells and other cells of the inner retina, but not photoreceptors. Invest.
Ophthalmol. Vis. Sci. 41, 927–936.
Wygnanski, T., Desatnik, H., Quigley, H.A., Glovinsky, Y., 1995.
Comparison of ganglion cell loss and cone loss in experimental
glaucoma. Am. J. Ophthalmol. 120, 184– 189.