Quality Account for Garrow House, Northern Pathways
advertisement

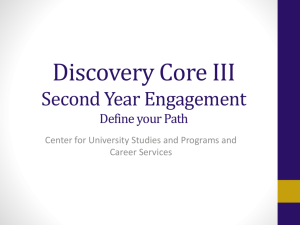
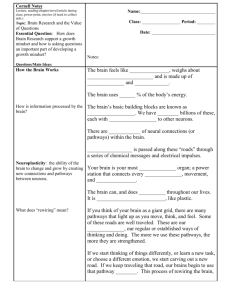
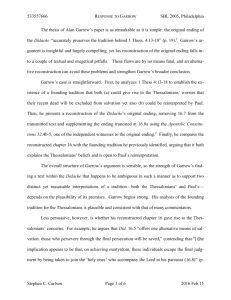
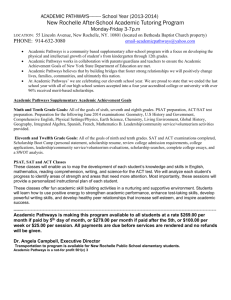
1 Quality Account for Garrow House, Northern Pathways 2011/2012 2 Contents Part One- Page 3 Statement on Quality from the Chair of the Northern Pathways Board Part 2- Page 4 Priorities for Improvement and Statements of Assurance from the Board Part 3-Page 9 Review of Quality Performance 3 Part One Statement on Quality from the Chair of the Northern Pathways Board Garrow House in York is a 12 bedded high support service for women stepping down from secure care. The service was developed by Northern Pathways, which is a joint venture between Turning Point and The Retreat. The service is part of a national Department of Health (DoH) pilot scheme and has been developed through a strategic partnership between the Department of Health, The Yorkshire and Humber Secure Services Commissioning Team (SSCT), Northern Pathways and the newly formed Leeds and York Partnership Foundation Trust (Formerly North Yorkshire and York). The service was developed in response to national high level policy guidance, including Women's Mental Health: into the Mainstream (2002) and the subsequent Implementation Guidance (2003), a regional strategy document, Forensic Services for Women a Strategy Document 2004-2008 and was informed by a strategic review of population need and service provision and a detailed service user involvement project. The result is a high quality service for women that enhances the care pathway for women in secure care. After several years in the planning, the service opened in January 2009 and as such 2011/12 has been its third full year of operation. A key aspect of the service development approach was to ensure that Garrow House was informed by the views of the women for whom the service was intended. A project was commissioned by the Forensic Catchment Group to consult with the women and to ensure their views were fully incorporated into the service specification and design of the building and service model. The result of this was the Women's Involvement Project (2007) which produced a comprehensive range of suggestions about the service philosophy, physical design and range of treatments and activities that should be offered within the service, all of which have been incorporated into the service. As a new service and a new company, we were committed to ensuring robust structures, and systems were set up from the outset to define, monitor and assess quality. These have included: • • • • • • • Development of Northern Pathways Board. Monthly Risk Management Group. A quarterly Northern Pathways Governance Committee including all key parties to ensure business and clinical governance. Implementation of Turning Point’s internal quality assurance tool (IQAT) mapped to the Care Quality Commission (CQC) Independent Hospital standards. Women’s involvement systems including the appointment of an Involvement Worker in the service set up phase and the following women’s involvement processes: weekly community meetings, weekly involvement group, one to one women’s sessions, monthly women’s governance meetings, representation from the women on the governance group and committee, the Department of Health (DoH) monitoring meetings, attendance at the steering group, the service model’s workshop and all away days and partners’ workshops. Also a representative attends the Regional Involvement Strategy and project groups. The women also sit on the newly formed Recovery and outcomes Group. Involvement in the DoH national evaluation of the pilots. Amendments to the staffing and management structure to create a Clinical Lead post to ensure clinical quality, and introduction of dedicated Project Worker posts leading on quality assurance and CQUIN Achievement. During the third year of the pilot, Garrow House has worked hard to maintain and develop a high quality service and we are very pleased with the results. In the 4th quarter of 2012 the service achieved all the innovation goals agreed between Northern Pathways and the regional commissioners for the provision of NHS services, through the Commissioning for Quality and Improvement payments framework and achieved all available incentive payments. Robust involvement systems are in place which means that the women within the service are actively involved in all aspects of their care and service delivery. To date this has resulted in high levels of satisfaction and development of a service which the women consistently state is meeting their needs. 4 There has been a continual rolling quality action plan managed by the Service Manager and reported on to the Governance Committee which has covered all areas indentified where quality improvement has been required. We feel that there has been a proactive approach to quality assurance and that staff alongside service users have worked hard to identity areas where improvement is required and have taken the relevant actions to ensure that all areas are resolved and improved. Quality improvement is an ongoing priority for the service and it is always top of the agenda. I, Andy James, state that to the best of my knowledge the content of this report accurately reflects the account of quality activities and the current situation. Signed, Andy James, Chair Northern Pathways Part 2 Priorities for Improvement and Statements of Assurance from the Board 2.1 Priorities for improvement 2012-2013 In 2012 Northern Pathway’s three priorities reflect the Board and leaderships team`s commitment to continuously improving patient safety, clinical effectiveness and patient experience: Priority 1. The introduction of a new Risk Management Group and Policy Ratification Group. Rationale. In the CQC regular inspection at the end of 2011 it was identified that we needed to make improvements to our risk management and audit processes. The Risk Management Group was introduced to ensue that our risk management processes are clear. It will ensure incidents are rigorously reviewed and lessons learnt cascaded to the whole team. It is to be supported by attendance from Turning Point`s Risk and Assurance department. It will also take responsibility for audit in response to our CQC action plan. The Policy Group has been established to ensure that Northern Pathways develop operational policies that reflect its ethos of involvement. On behalf of the Clinical Governance Committee the Policy Ratification Group (PRG) will be responsible for the approval of all local Garrow House documents. The group will identify where there is a need for a local Garrow House policy and where it is more appropriate to follow a core Turning Point policy. Plan. Establish new risk management and policies groups including Terms of Reference and standing agendas by end of Q1. Establish new audit and policy review schedules by the end of Q2 Monitoring. • • By Risk and Assurance by their attendance at Risk Management Group meetings By the Northern Pathways Governance Committee through quarterly meetings. 5 • • • • By Northern Pathways Board through the reports provided by the Governance committee. By Commissioners through the monthly CQUIN reporting system, and contract meetings. By CQC inspections. Through the Internal Quality Assessment Process Reporting. Reporting will be through the Governance Group to the quarterly Governance Committee, who will report quarterly to the Board. Project Lead. Service Manager; Chris Dawson Senior Management Lead. Assistant Director Janine Strange Priority 2. In collaboration with the women who use our service, our partners and commissioners we will strengthen and improve our recovery pathway. This will be done by participating in and achieving Specialist Mental Health CQUINs 2012/13: • • • Shared Pathway – Recovery and Outcomes Implementing a standard secure pathway Secure Forensic Pathway Feasibility Project In addition to the monitoring measures described below a Recovery and Outcomes Group has been established in collaboration with the women. Rationale. Northern Pathways was established to support women who required a high level of support to move out of secure care. With a high level of involvement and socially inclusive activity it has successfully supported many women to live more independent and fulfilling lives. In 2012 -13 it will continue to focus its energy on improving its recovery pathway in preparation for the service participating in clustering and payment by results initiatives. Plan: • Establish a Recovery and Outcomes Group at Garrow House • Attend regional groups cascading good practice. • Participate in and achieve pathway related CQUINs Monitoring: • • • By the Northern Pathways` Governance Committee through quarterly meetings. By Northern Pathways` Board through the reports provided by the Governance committee. By Commissioners through the monthly CQUIN reporting system, and contract meetings. Reporting. This will be through the Service Manager and to Northern Pathways Board. Reports will be submitted to Commissioners within 20 working days of the end of each quarter. 6 Project lead: Clinical Development Specialist, Karen Abrahams and Involvement Lead, Holly Baker Senior Management lead Assistant Director, Janine Strange. Priority 3 Improve the services response to self harm by the introduction of a shared protocol (agreed with the women) on self harm and the provision of DBT training for staff. Rationale This priority reflects our awareness that while overall numbers of incidents are relatively low, self harm continues to be the most frequently reported area of concern. Our aim is to provide a collaborative supportive response to the women requiring support in this area. We also want to increase the staff team’s confidence in providing interventions around self harm. Plan. Establish a shared learning group related to self harm to enhance the teams skill and provide a forum to look at issues it raises. By end Q 1. Establish a community based “Managing Emotions” Group for the women by end Q 1 Write a protocol with the women relating to self harm outlining what the women can expect from the staff and what the staff can expect from the women. By end Q2 Provide training for the staff in therapeutic intervention in self harm.Q2 Q3 and Q4 Garrow House will participate in regional initiatives relating to self harm including work undertaken by a Sub Group of in the Adult Secure Providers Security and Operational Group. • • • • • Monitoring o o o By the Northern Pathways’ Governance Committee through quarterly meetings. By Northern Pathways’ board through the reports provided by the Governance committee. By the leadership team at weekly meetings Reporting This is a Northern Pathways Governance action but regular reports will also go to Risk Management and Leadership Groups Project Lead Consultant Psychologist, Lindsay Jones and Service Manager, Chris Dawson Senior Management Lead Assistant Director, Janine Strange. 7 2.2 Statement of Assurance from the Board Review of Services During 2011/12 Northern Pathways provided 1 NHS service, namely Garrow House. Northern Pathways has reviewed all the data available to them on the quality of care in the 1 NHS service. The income generated by the NHS services reviewed in 2011/12 represents 100% of the total income generated from the provision of the NHS services by Northern Pathways for 2010/11. Participation in Clinical Audits During 2010/11 0 national clinical audits and 0 confidential enquiries covered NHS services that Northern Pathways provides. During 2010/11 Northern Pathways participated in 0 national clinical audits and 0 national confidential enquires, of the national clinical audits and confidential enquiries it was eligible to participate in. The reports of 7 local clinical audits were reviewed by the provider in2011/2012 and Northern Pathways intends to take the following actions to improve the quality of healthcare provided: • • • Set up a new Risk Management Group Provide increased training in area indicated as requiring improvement.eg Self harm, 12 essential standards of CPA Rapid Tranquilisation and electronic record keeping system. Increased monitoring of all SUI and audit actions through leadership and Risk Management Groups. In addition to the local audits Northern Pathways participates in an Internal Quality Assessment tool hosted by one of the partner organisations Turning Point. This Internal Quality Assessment tool (IQAT) is a set of audit tools that detail how the service will deliver regulated activities and meet the essential standards of Quality and Safety. The Service also provides a quarterly report to the North of England Specialist Commissioning Group (Yorkshire and Humber) of Key Performance Indicators. Research The number of patients receiving NHS services provided or sub-contracted by Northern Pathways in 2011-2012 that were recruited during that period to Participate in research approved by a research ethics committee was 0 Garrow House has participated in a Department of Health commissioned evaluation of all services within the Department of Health High Support Services pilot scheme being undertaken by London Metropolitan University. The findings of this pilot are pending. A National Service Evaluation- Women's Pathways of Care in Secure Services: Garrow House participated in this Research by The University of Central Lancashire. The purpose of the study was to assess whether women are appropriately placed and examine obstructions and facilitators to moving women on. With other providers in the region Garrow House took part in this evaluation study and received positive verbal feedback from the researchers on the ethos of the service. Goals Agreed with Commissioners 8 A proportion of Northern Pathway` income in 2012/11 was conditional on achieving quality improvement and innovation goals agreed between Northern Pathways and the regional commissioners for the provision of NHS services, through the Commissioning for Quality and Improvement payments framework. The following CQUINs were participated in in 2011/2012: • • • • • • Essence HoNOS Length of Stay 25 hours of meaningful activity Involvement, Choice and Responsibility Recovery Planning We achieved 70% compliance In Q2 and 80% compliance in Q3 We have addressed areas where we didn’t achieve the CQUIN payment by improving our governance and reporting systems. What Others Say About Us Garrow House, Northern Pathways is required to register with the Care Quality Commission and its current registration status is registered. The Care Quality Commission has not taken any enforcement action against Northern Pathways during 2011/2012. Northern Pathways is subject to periodic reviews by the Care Quality Commission and a regular inspection was conducted in December 2011.Of the 22 essential standards 6 were specifically reviewed on the day of the inspection of these 3 required compliance actions and one required an improvement action. Northern Pathways has not participated in any special reviews or investigations for the CQC during the reporting period. Data Quality Northern Pathways did not submit records during 2011/12 to the Secondary Users service for inclusion in the Hospital Episode Statistics.. Northern Pathways was not subject to the Payment by Results clinical coding audit during 2011/12 by the Audit Commission. Northern Pathways was not subject to scoring for Information Quality and Records Manager assessed using the information Governance Toolkit 9 Part 3 Review of Quality Performance 3.1 Review of Quality Performance in 2011 – 2012 One of the most important aims for the service must be to look back and objectively review our performance and position throughout 2011/12 in order to ensure that we build on the success of the pilot service which officially ends in March 2013. The priorities we identified over the last financial year have been listed as below and updates made for the board. Update on priorities 2011-2012. 1. Maintain registration with CQC as Northern Pathways and achieve full compliance with CQC standards, so enhancing our clinical effectiveness. The service received positive feedback from the inspectors around respecting and involving people who use our services. However, the service was non compliant in 3 areas, an action plan has been written to address these. Quality standards were also consistently monitored through the Internal Quality Assessment Tool (IQAT). This is modelled on the CQC standards and provides a systematic framework for reviewing each standard. Garrow House has consistently achieved the majority of these standards and has action plans to address the few outstanding standards. 2. Achievement of the Quality and Innovation standards (CQUIN) as detailed in the annual contract, linked to the patient experience. These included: • • • • Risk - Use of HoNOS, HCR 20 Assessment tools Innovation - Use of Essence Climate Scale Environmental scale Service User experience – Involvement choice and responsibility, CPA Standards, Dining Experience and 25 hour Structured Meaningful Activity Effectiveness - Use of recovery planning tool, Recovery Star, Arrow Toolkit The service successfully has successfully implemented all the tools and initiatives described in CQUINs leading to positive improvements for the women who use our service. A number of new tools are now firmly embedded in our electronic records management systems. The women have also benefitted from increased therapeutic activity including complimentary therapies and a dining experience that supports both communal and self catering experiences .In the third quarter 80% of the CQUINs were achieved with only the quality of one report requiring improvement. In the fourth quarter the service achieved 100% of the CQUIN requirements. 3. Reduction in incidents (particularly self harm and aggression) by proactive trend and clinical analysis and improved intervention measures, links to patient safety. Garrow House provides a very safe environment in the least restrictive environment necessary to maintain the safety of women who had previously been cared for in higher security. This is reflected in relatively low levels of incidents in all area, with the exception of self harm. For example there are rarely incidents of physical aggression. At Garrow House the prevalence of self harm as a coping strategy is also characteristic of some the women the service supports and remains a priority Therefore the service will continue to proactively develop a strategy to address self harm. 10 3.2 Outcomes To enable us to evidence that the women are able to move forward significantly in their recovery, Garrow, we utilise a number of outcome measures within the service. CQUIN (Recovery Star, HoNOS and the Essences Environmental Scale), data has also been collected using the Symptom Checklist- 90 (HCR-20). The data from routine risk assessments (HCR-20 and START) is also being recorded as an outcome measure. All women have an initial Recovery Star within 2 weeks of admission to the service and thereafter complete a self assessment, with a staff member, quarterly, to evidence their recovery journey. The results of these are entered into our Client Information Management (CIM) system, and the results are shown on a distance travelled pie chart for April 2012. This data is based on the 6 active clients who have more than one Star reading. The % of people improved/decreased or stayed the same is based on the difference in scores between the first Star reading and the most recent star reading. 17% % Improved % No Movement 50% 33% % Decreased 11 Outcomes of Involvement Involvement has been and continues to be integral to the ethos of Garrow House. Everyone within the service plays a key role within involvement. Involvement is not owned, it is shared, and there is a culture of involvement across the organisation. The women within the service are empowered to be involved in their own recovery, service development, regional involvement development and national involvement agendas. Within the service the clinical governance structure and the community meetings ensure that there is an opportunity to communicate the ideas and opinions of the women and to feedback any service development, with the women attending or chairing these meetings. It is recognised that involvement aids recovery, and as such the women are involved as much as possible in all aspects of their recovery and in anything that affects their experience at Garrow House, from co writing all their recovery plans, to being consulted about any service changes or delivery that is being proposed before any changes take place. In this way the women we support are active participants within the service and drive their own recovery and experiences here. The priorities for involvement within the service are based on the User Defined Standards. The outcomes from these standards are increased involvement, greater choice, speedier recovery, and enhanced empowerment and control. A large piece of work was recently undertaken by the Involvement Coordinator and the women at Garrow to write an Involvement Strategy for the service, what areas will be worked on, how progress will be tracked and what the outcomes will be. This piece of work will drive involvement and ensure that we keep pushing ourselves to enhance involvement at Garrow House and the women’s experiences here. Laura (Service User at Garrow House 2011-12) Laura is a 21 year old woman who came to Garrow House from a medium secure service in February 2011. She was lacking in confidence and struggled to trust and engage with staff initially. She frequently used self harm as a strategy to cope with her emotions. Her confidence slowly grew and she began to attend community meetings regularly in the house, expressing her views eloquently. She began to feel passionately about involvement and attended the regional Recovery Involvement for Improvement workshops with the Involvement Coordinator at Garrow. This also slowly developed over a period of a few months where she began to take a more active role in this setting, co chairing and planning these meetings with the regional involvement lead, the involvement coordinator from Garrow House and a staff member and service user from another hospital in the region. Towards the end of the Recovery workshops Laura was confident enough to stand up in front of 50-60 staff and service users from secure services across Yorkshire and Humber and co chair the workshops. Laura became informal within 4 months of coming to Garrow House, and although she struggled at times her self harm decreased significantly and her confidence grew. Laura also sat on interview panels for new staff coming into the service and wrote reports about her experiences on the Recovery workshops and piloting ChatNet (a web based involvement and discussion forum) for the YHSCG website. Laura was discharged from Garrow House in May 2012 and is now living in a flat in the community. She has not self harmed for the last 6 months, and is keen to get a job and help people in a similar situation to herself in the future. “Involvement supports women to have a voice, it helps women to communicate, and it’s a way forward. It boosts your self esteem because you feel listened to. You feel more self-aware, I think it helps you to think about the other women in the service; it’s like you’re not the only one with a voice so it makes you a better listener. Speaking for other women in the service makes you think of others as well as yourself; I think it is this that helps to build relationships in the house. I think it is very empowering to become an advocate and voice for the women, it makes you communicate on lots of levels, speaking, listening and supporting.” 12 Megan (Service User at Garrow House) “I have been involved with Garrow House for at least 5 years. I had input into the design of the service and what women wanted from a high support service. I then came into Garrow House 2 years ago. I think that Involvement empowers you to care for yourself and if you get involved as much as possible and see results it makes you feel valued. I go to different regional meetings and get to have a say in the way services are shaped across the region. I think that this helps the women to speak their minds and this happens most of the time at Garrow. Things have changed at Garrow and become more individual. The women are asked what they want to work on and what their interests are and the therapeutic timetables and recovery plans are done jointly with the women. I think that if you decide what you want to do and draw up the timetables and the recovery plans with the staff, it makes you want to do it more, so you take ownership of your work and recovery. If you are making your own decisions and are involved in all aspects of your recovery it means more and you get more out of what you are doing. Garrow House is different and it has changed, but this is not a bad thing as it is evolving to meet the needs of the women in the service. This means that it is doing what it said it would. ‘The service fits around the women, the women don’t fit around the service.” (Service User at Garrow House 2012). 3.3 Complaints, comments and compliments One measure of quality around patient experience used by Northern Pathways is the analysis of the complaints, comments and compliments made by the service users. We received two formal written complaints in 2012. Both were low risk and minor impact .They were investigated and resolved with the complainants. We received one concern that was resolved to the satisfaction the women concerned. Garrow House has a weekly Community meeting where complaints, concerns and compliments can be raised and resolved informally at the earliest opportunity. Compliments received through the community meetings centre around new women thanking everyone for making them feel welcome in the service, and staff thanking the women for their hard work in contributing to the day to day activities in the house, as well as how well the women support each other. Other compliments include the women thanking each other for the support they have received from peers, and thanking the staff for facilitating activities that they have particularly enjoyed. We also received a compliment from a visitor to the service for the women and the staff. “I just wanted to thank all the women and staff that I met during my recent visit to Garrow House - for your hospitality, time and information sharing. It was a very informative visit for me, the service you provide at Garrow stands as a real example for how I hope our service will develop. 3.4Clinical Effectiveness Between April 2011 and the end of March 2012 Garrow House assessed 18 and admitted 8.The service achieved an average occupancy rate of 91.6% (11 Beds). 13 The following graph indicates the occupancy trend over the past 24 months. . Occupancy Occupancy 2010-2012 12 11.5 11.0 11 10.3 10 10.0 9 8 7 6 10-11 11-12 12-13 Target Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar • Although occupancy dipped in December and January, there were 2 prompt admissions and the service was full again by the end of the year • • • Average Occupancy for 2011-12 = 91.66%. (11 beds) This is just below the target of 93% (11.6 beds) The service has had at least 10 beds full for the past 24 months The service is currently full (May 2012) and the occupancy has not dropped below 10 in the past 24 months. There are currently 4 women who are informal patients, three women regularly attend college and three who undertake voluntary work. .We are actively developing pathways into less secure care for example by working with Leeds personality disorder pathway service and increasing our social work provision. The development of pathways is also a major CQUIN objective. To this end we have set up a Recovery and Outcomes Group In order to ensure staff competency to deliver clinical effectiveness the following has been developed: • An annually-reviewed service specific competent worker programme is in place. This ensures that all new staff have a comprehensive induction and complete all relevant learning and development within their six-month probationary period. Completion in recorded centrally and reviewed regularly. 14 Learning & Development Training Modules Completed (excludes Casual workers) Face to Face NP staff 33 % Jun %Aug % Sep % Dec % Apr % Change NHS E-Learning Modules E Learning Mental Capacity Safeguarding Food Key EmerHygiene Act and Info Vulnerable Working gency Intro to DepDementia Security Adults & Young Level 2 Skills First Aid at IG rivation of People (Front E Guidelines Day 1 Work line Workers) Learning Liberty Awareness 30 25 27 8 27 28 85% 85 82 82 80 74% 74 71 76 63 85% 85 82 82 87 18% 21 24 24 27 3 -20 -13 5 3 n/a 3 85% 85 82 82 77 88% 88 85 85 80 n/a -5 -5 Only 8 Competent Worker modules are less than 90% complete All other modules are 80% complete or higher; • Face to Face- 15 modules • E-learning – 11 modules In addition, the staff team at Garrow House has developed competencies to meet the needs of the complex client group. Staff have participated in specialist training in the following areas: • • • • • . Cognitive Analytical Therapy training Relational Skills training Equality and Diversity training The Knowledge and Understanding Framework for Personality Disorder Four support workers are being supported on the foundation degree nursing programme. 15 Health & Wellbeing The staff team is an essential part of the success of Garrow House. It has continued to be a relatively stable element of the service as the graph below shows. Workforce Performance - Turnover Leavers & Joiners 2011-12 4 Leavers Joiners 3 2 1 0 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr Vacancy Staff Staff and Vacancy Numbers 2011-12 36 30 24 18 32.5 33.4 32.4 32.4 33.2 33.4 33.5 33.5 33.5 32.5 31.5 30.5 31.5 Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar 12 6 0 During the past year there have been 6 leavers and 4 new joiners, although 2 of the leavers have since rejoined the service. Exit interviews are routinely completed. This stable, highly trained and highly motivated staff team has impressively low levels of sickness. Over the past year, sickness levels have been both below the target the service set for itself, and against the benchmark of the CIPD average for the sector of 0.8 Lost Working days per employee per month. There has been no long-term sickness since July 2011. 16 HR - Employee Welfare Lost Working Days 2011-12 45 LT ST 30 15 17 Mar 1.5 9 1 0 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Garrow Target 1.0 CIPD 0.8 Average Lost Working Days per Employee 1.0 0.5 New policy 0.0 Mar • Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Sickness continues to be low, with no long-term sickness since July. After the seasonal increase in Dec & Jan, sickness levels have dropped The Garrow House therapeutic model aims to enhance psychologically informed care through relational understandings. Within the model, staff support and supervision is viewed as essential. It is acknowledged that the work can be emotionally demanding and that the staff team need to be well functioning in order to provide high quality care. Supervision and support for staff is therefore seen as integral to the model, and a reflection culture is encouraged. Staff protected time each day allows for this. Staff have weekly group supervision facilitated by an external therapist. There is also a weekly risk supervision group in which the risk assessments, formulations and management plans are discussed. Shared formulation meetings are also held. More informal opportunities for reflective practice are also encouraged, including the introduction of weekly shared learning seminars. In addition, all staff have identified clinical supervisors and are expected to access a minimum of one hour of individual clinical supervision each month. 3.1.3 Patient Safety Through the Quarterly Governance Committee patient safety has been assessed. An analysis of all incidents is undertaken monthly through the service governance and this group reports to the Quarterly Governance Committee. To date the service has been a high incident reporting service and the committee wished to analyse the type of incidents and trends to determine any improvements to service delivery. 17 Incident analysis for 2011/12. The most frequently reported incident type across the period was self harm. Hence a priority for 2012-2013 is the establishment of a shared protocol on self harm agreed with the women who use our services. Incidents are reported to Turning Point’s Risk and Assurance team through an electronic reporting system (DATIX).They are also reviewed internally by the leadership team who cascade learning from incidents to the wider team .As of June 2012 all incidents will undergo review by the newly formed Risk Management Group. 18 Under contractual arrangements serious incidents are also submitted for review to Yorkshire and Humber Secure and Specialist Mental Health Commissioning Team. Reports are submitted within 24 hours and at 5 day and 12 week intervals. Garrow House participates in the Adult Secure Providers Security and Operational Group Meeting. This meeting brings together commissioners and providers from the region enabling the sharing of good practice and quality initiatives. Statements from Local Involvement Networks, Overview and Scrutiny Committees and PCT’s Service User experience at Garrow House is second to none. The underlying ethos of women being involved in all aspects of their care has been maintained and has led to the provision of a service that is an exemplar of good practice. The biggest challenge for the service continues to be maintenance of the partnership between the two 3rd sector providers and the NHS – ‘sub contracting’ for the medical and psychological input continues to exacerbate this. The formation of LYPFT allows this relationship to be developed beyond a contractual level and I would encourage this. Mick Burns Senior Commissioning Manager Secure and Specialist Mental Health Commissioning North of England Specialised Commissioning Group-Yorkshire and the Humber Office 19 York LINk Holgate Villa 22 Holgate Road York YO24 4AB Mr Chris Dawson Service Manager Garrow House 115 Heslington Road York YO10 5BS 15th June 2012 Dear Mr Dawson Garrow House Quality Account 2011 - 2012 Thank you for giving York LINk the opportunity to comment on your Quality Account for 2011-2012. Most of the account was very easy to read and understand although there was a little difficulty with the Learning and Development Table. We were particularly impressed with the Introduction to the Account which provided clear details about the services offered at Garrow House. We would, however have liked to see a glossary of terms plus an explanation of the abbreviations used to make the account more accessible. We are pleased that you have involved the residents in setting up new systems to improve your services. During the coming year, if there is any way you feel that the LINk could be of assistance to you in improving or enhancing your residents’ experience, please do not hesitate to get in touch. Yours sincerely Mrs Lesley Pratt Chair, York LINk 20 3.2 Feedback on Garrow Houses Quality account. For more information on Garrow House or to give feedback on this account please visit our website on http://www.northernpathways.co.uk/ and complete a contact form.