journeys recovery Quality accounts for 2010/11
advertisement

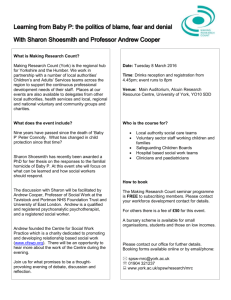
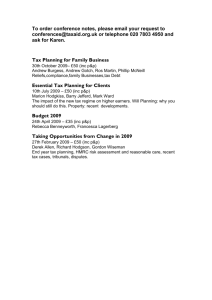
recovery journeys Quality accounts for 2010/11 2 | Quality accounts for 2010/11 contents Part one - tracking progress 3 Part two - regulatory information 8 Part three - on track with patient safety, clinical effectiveness and patient experience 12 Tracking progress The past year has seen major changes in the healthcare landscape. We’ve seen a new government take control; significant changes starting to affect sector funding; and the launch of a series of health bills proposing greater local accountability, support and choice for service users. It’s clear that the world is changing and that means both challenges and opportunities for healthcare providers. The key challenges organisations like St Andrew’s must face are: n Proving that we offer the best quality services for a reasonable price n Showing that value can be achieved through shorter recovery times as well as keener pricing n Setting new standards to attract, develop and keep the highest calibre staff. On the other hand, there are opportunities for the charity: n Investing any surpluses we make into specialist therapies, services and environments that help service users recover more quickly n Spending more time and effort on service user engagement, making sure that we actively respond to their ideas and concerns n Developing new tools and techniques - testing their effectiveness and then sharing the results across the sector n 1 Working with partners to develop new services, in response to specialist needs. Our direction of travel is clear. St Andrew’s vision is to be a world-class mental healthcare provider, whose services across the UK set the benchmark for excellence. We’re totally dedicated to making that vision real - putting quality healthcare on the map, and our service users in the driving seat. This strength of vision explains why we’ve remained ahead for more than 170 years; why we’ve tirelessly supported the NHS since its inception in 1948; and why we’re still growing in difficult times. We firmly believe that with the right people, partners and attitude, we can look forward to the future together with optimism. I hope that you enjoy reading this account of our work. Professor Philip Sugarman Chief Executive Officer and Medical Director 1. Professor Philip Sugarman, Chief Executive Officer and Medical Director Quality accounts for 2010/11 | 3 PART ONE TO THE ACCOUNTS “We aim to provide the highest quality clinical training through specialist services, engaging and supervising people, supporting studies and providing our own continuing professional development programme.” Tracking progress 1 This is the official quality accounts report for St Andrew’s Healthcare, covering the period 1 April 2010 to 31 March 2011. It outlines how the charity is performing, and our plans to improve. well. More than 3,500 people work in our Northampton, Birmingham, Essex and Nottinghamshire hospitals; employing and keeping the best staff is fundamental to our success. Since last year’s report was published, St Andrew’s has opened two new regional hospitals and a specialist national facility. We’ve won national awards for innovation and healthcare outcomes. We achieved 80 per cent service user satisfaction with food quality, and were described as excellent practice in the Soil Association’s First Aid for Hospital Food report. We were also the only independent healthcare provider chosen for the Implementing Recovery, Organisational Change (ImROC) national recovery programme pilot. We aim to provide the highest quality clinical training through specialist services, engaging and supervising people, supporting studies and providing our own continuing professional development programme. Our academic partnership with the Institute of Psychiatry, King’s College London, also develops research opportunities. But we must keep moving and improving, if we’re going to be the best in the sector. We’re currently trialling our first length of stay ‘price promise’ in Nottinghamshire, and aim to develop this further across other services. We need to improve the quality of reporting information, which will free up more clinical time for patient care. And we must ensure that service users remain centred at the heart of our work helping us to make the right decisions. During 2010/11 we launched two new specialist qualifications in partnership with the University of Northampton: a BSc (Hons) degree in Mental Healthcare, and the Certificate in Higher Education in Mental Health. These courses will create training opportunities for our own staff, and support NHS professionals with formal study options - helping to develop and grow the healthcare leaders of the future. On behalf of St Andrew’s, I confirm that to the best of my knowledge, the information contained in this document is accurate. These accounts were also approved by the charity’s Board of Directors on 27 May 2011. We have identified clear priorities for improving patient safety, clinical effectiveness and people’s experiences of our services. Page 5 lists these priorities, what we plan to do and how we’ll track progress. To achieve great results, we must ensure that everyone is equipped to do their job Caroline Rose Director of Nursing and Quality 1. Caroline Rose, Director of Nursing and Quality 4 | Quality accounts for 2010/11 1 1. We use various performance measures to assess patient satisfaction with food 2 2. St Andrew’s is determined to provide great value for partners through strong performance management Quality routes St Andrew’s wants to set the quality standards for service users across the mental healthcare sector. The quality of care we provide is vital to helping people on their journey to recovery; it often changes their lives. So of course we aim to give the very best support and make sure that everyone achieves their maximum potential whilst staying with us. In this report, you’ll find some real-life patient stories and see how people have overcome difficult and traumatic situations to live the most positive life they can. The people we work with inspire us and we hope their stories inspire you too. Of course, it’s easy to focus on the highlights, compliments and awards. But we don’t look at these things in isolation. We use a range of performance measures to gauge how good our services are. These include: n Listening to views from service users on the care they receive from us n Assessing patient satisfaction on their experiences of dignity, food, living spaces and the way we communicate with them n Monitoring the ‘outcomes’ (results) that our clinical treatments deliver - such as people moving into less secure settings, and returning to community life n Checking the length of time that our service users stay with us n Comparing our work to other healthcare providers, by sharing performance data and service information n Taking part in local and national service audits and listening to feedback from regulators and commissioners n Being accountable to our board of trustees, who provide independent feedback and input. Taken together, this information gives us a ‘dashboard’ of statistics and feedback that helps us to keep track of the charity’s performance, and make sure we’re spending money wisely. That’s important because the Government’s Quality, Innovation, Productivity and Prevention programme wants to make sure that health spending achieves maximum benefit and quality of care. And we want the same thing - great value for the services we provide to our NHS partners. Quality accounts for 2010/11 | 5 Improvement planner In preparing these accounts, St Andrew’s discussed quality priorities with service users, staff and trustees. The results of these conversations have led to us agreeing the following improvement priorities for 2011/12. Quality priorities Patient safety Essen Climate Evaluation Scale (EssenCES) Why this is important Objectives for 2011/12 This scale explores how much service users feel safe and supported, by both their peers and care staff. Evidence suggests that patients respond better, engage more and recover more quickly where they feel safe and comfortable. This indicator is part of the Commissioning for Quality and Innovation (CQUIN) payment framework and a Care Quality Commission requirement. n n n Identify a service development or improvement based on the 2010/11 surveys (patient perceptions of the risk status system) Produce an implementation plan to achieve the improvement within 2011/12 Monitor progress throughout the year Patient safety Design manual We need to make sure that our hospitals provide safe and secure environments for patients and staff. Having agreed quality standards and sharing information on product testing means that all of our facilities can learn from past experience. n Less incidents relating to buildings, fixtures and fittings Patient safety Safe access to technology Patients benefit from using technology for work, leisure, education and communication. We want to help help people people access access technology technology safely, whilstsafely, making whilst suremaking sure equipment equipment is used is used appropriately. appropriately. n Organise charity-wide training on managing risks safely Provide regional testing equipment and training Increase resources for forensic screening Investigate potential for music library and patient intranet Explore ways of helping service users connect with relatives (such as video conferencing) n n n n Clinical effectiveness Recovery planning Where service users and care staff work in partnership to achieve a shared understanding of recovery, it’s assumed that length of stay will be shorter and patient experiences of care improved. This indicator is part of the Commissioning for Quality and Innovation (CQUIN) payment framework. n n n n All service users offered the opportunity to complete a recovery plan appropriate to their needs Plans reviewed formally Monitor uptake and report quarterly on performance Progress the Implementing Recovery, Organisational Change pilot, which will in turn impact on all aspects of service user and staff experiences of care 6 | Quality accounts for 2010/11 Quality priorities Clinical effectiveness Care Programme Approach (CPA) Why this is important Through CPA, St Andrew’s supports service users to help them achieve optimal mental health and recovery. The focus is on working in partnership with service users to plan and manage their treatment programmes. This helps them to move out of secure care and back into the community. Objectives for 2011/12 n n n n Clinical effectiveness Enhancing physical healthcare People with mental health difficulties need access to good physical healthcare. Through regular health checks, screening programmes and vaccinations we can spot possible problems and make sure service users get any treatments they need. That’s good for their long-term physical and mental health. n n n This indicator is standard to most of our NHS contracts. Clinical effectiveness 25 hours therapeutic activity Evidence suggests that boredom and reduced motivation results in poorer clinical outcomes for service users in secure care. This indicator promotes a balanced and structured day of meaningful activity, linked to agreed care plans that promote recovery. n This indicator is part of the Commissioning for Quality and Innovation (CQUIN) payment framework. n n n Review the charity’s CPA processes to bring together clinical practice and contractual requirements Make sure that service users contribute to the review Review the charity’s policy, key roles and responsibilities in Spring 2011 Review CPA measures as part of the St Andrew’s ‘balanced scorecard’ for managing performance Introduce the new Patient Environment Action Teams (PEAT) tool to monitor patient satisfaction with the cleanliness of ward environments Achieve the National Institute for Clinical Excellence quality standards for diabetes in adults by year end Exceed the World Health Organisation influenza vaccination targets (75 per cent for both over-65s and under-65s ‘at risk’) Align the charity’s systems and treatment programmes with the agreed national definition of ‘meaningful activity’ Audit services using new agreed national benchmarking tool Develop and implement work plan to address any needs identified in audit Develop new performance framework using timetabling module in patient records system Quality accounts for 2010/11 | 7 Quality priorities Patient experience Dining Why this is important Food quality and menu choices are very important to the daily life of most service users. Objectives for 2011/12 n n By giving people freshly-cooked, tasty produce, we can help improve their quality of life as well as their physical and mental health. n n n n Patient experience Patient experience Dignity Involvement and personalisation strategy Helping vulnerable service users to retain their dignity whilst in secure care is hugely important to St Andrew’s. Supporting people to give them the best quality of life throughout their stay is likely to achieve better service user experiences of care. n Where service users and care staff work in partnership, patients are likely to move through a shared pathway more quickly. This is likely to mean shorter stays and better service user experiences of care. n This indicator is part of the Commissioning for Quality and Innovation (CQUIN) payment framework n n Complete nutritional analysis of charity recipes and share ‘healthiest options’ on intranet Maintain level of sustainable and ethical food produce as proportion of total spend Complete initial nutrition and wellbeing training programme Maintain customer satisfaction levels with the dining experience Develop on-site herb gardens to support the charity’s kitchens Support service users to grow fruit and vegetables and build understanding of food production Comprehensively review the charity’s dignity, choice and care policy by June 2011 and implement practice changes during the year Identify key actions and milestones to make sure our approach to dignity is consistent with the very latest sector practice Implement service user involvement strategy for the charity, linked to the national service user groups Produce joint service user and staff report to show how the charity can achieve the choices made by patients for the year This report is not intended to sit on a shelf gathering dust; we will use it regularly to monitor performance against targets and invite feedback from our partners. St Andrew’s will track progress in the following ways: n Document the targets and key information on our intranet n Report updates against targets to Board meetings n Invite input on key targets and ongoing performance from service users. 8 | Quality accounts for 2010/11 PART TWO TO THE ACCOUNTS This section provides information in the official format required under the National Health Service (Quality Accounts) Regulations 2010. Reporting period: 1 April 2010 to 31 March 2011 Name of provider: St Andrew’s Healthcare Driving improvements 1 Review of services During the reporting period 2010/2011 St Andrew’s Healthcare provided clinical services in the field of mental health to over 700 service users, commissioned by more than 130 different NHS Services and other organisations. 2 St Andrew’s Healthcare has reviewed all the data available to it on the quality of care in respect of all the services for which it provides clinical services. The income generated by the NHS services reviewed in 2010/2011 represents 100% per cent of the total income generated from the provision of NHS services by St Andrew’s Healthcare for 1 April 2010 to 31 March 2011. Participation in clinical audits 1. During the year, St Andrew’s provided clinical services to over 700 service users 2. Hospital cleanliness is a key priority for the charity During 1 April 2010 to 31 March 2011, three national clinical audits and zero national confidential enquiries covered NHS services that St Andrew’s Healthcare provides. During that period St Andrew’s Healthcare participated in 100 per cent of the national clinical audits which it was eligible to participate in. The national clinical audits that St Andrew’s Healthcare was eligible to participate in during the reporting period are as follows: Clinical audits Prescribing Observatory for Mental Health n Prescribing of Antipsychotics for Children and Adolescents n Monitoring of Patients Prescribed Lithium n Medicines Reconciliation. The national clinical audits that St Andrew’s Healthcare participated in during the reporting period are as follows: Prescribing Observatory for Mental Health n Prescribing of Antipsychotics for Children and Adolescents n Monitoring of Patients Prescribed Lithium n Medicines Reconciliation. Quality accounts for 2010/11 | 9 1 The national clinical audits that St Andrew’s Healthcare participated in, and for which data collection was completed during the reporting period, are listed below alongside the number of cases submitted to each audit as a percentage of the number of registered cases required by the terms of that audit. Audit Participation Participant numbers Sample size Prescribing of Antipsychotics for Children and Adolescents Yes 67 service users* 100% Monitoring of Patients Prescribed Lithium Yes 22 service users* 100% Medicines Reconciliation Yes 10 service users* 100% of two admission wards as sample base • Figures based on service users who met the criteria in the auditing period The report of one national clinical audit was reviewed by the provider in the reporting period and St Andrew’s Healthcare intends to take the following actions to improve the quality of healthcare provided: n n Information used as a baseline to improve Medicines Policy and Procedures, particularly in regard to complying with NPSA alerts Presentation at in-house training event - Prescribing Observatory for Mental Health, Audit Process and Lithium Report. These are reports published in 2010 that may relate to data collected in 2009/10 but may also relate to an earlier collection of data, that is, the audit and report of the audit fall in different financial years. St Andrew’s Healthcare has a comprehensive clinical audit programme supported by governance structures. The reports of 77 local clinical audits (applied to all wards) were reviewed by the provider in 2010/11 and St Andrew’s Healthcare intends to take a range of actions to improve the quality of healthcare provided. Further details are available electronically from Caroline Rose, Director of Nursing and Quality; please email crose@standrew.co.uk for this information. Research The number of patients receiving NHS services provided or sub-contracted by St Andrew’s Healthcare in 1 April 2010 to 31 March 2011 that were recruited during that period to participate in research approved by a research ethics committee was 159. Use of the CQUIN payment framework A proportion of St Andrew’s Healthcare’s income in 1 April 2010 to 31 March 2011 was conditional on achieving quality improvement and innovation goals agreed between St Andrew’s Healthcare and any person or body they entered into a contract, agreement or arrangement with for the provision of NHS services, through the Commissioning for Quality and Innovation payment framework. Further details of the agreed goals for the reporting period are available electronically from rjones@standrew.co.uk upon request. 1. St Andrew’s Healthcare has a comprehensive clinical audit programme 10 | Quality accounts for 2010/11 1 2 Statements from the Care Quality Commission St Andrew’s Healthcare is required to register with the Care Quality Commission (CQC) and is currently registered for: 3 The charity ensures that the information we record, hold and use in the treatment and care of our service users: n n n n Treatment of disease, disorder or injury Assessment or medical treatment of persons detained under the Mental Health Act 1983. St Andrew’s Healthcare has the following conditions on registration: n The Registered Provider must not provide services for people under thirteen years of age at the location St Andrew’s Healthcare, Adolescence Services, Northampton. The Care Quality Commission has not taken enforcement action against St Andrew’s Healthcare during 1 April 2010 to 31 March 2011. St Andrew’s Healthcare has not participated in any special reviews or investigations by the CQC during the reporting period. Data quality Statement of relevance of Data Quality and your actions to improve your Data Quality Good quality information underpins the effective delivery of patient care at St Andrew’s. n Is updated and validated in a timely manner Is monitored for accuracy and completeness Complies with the NHS national clinical coding ensuring consistency in reporting information that can be comparable with other organisations. Over the previous 12 months, St Andrew’s has been following a strategy to ensure that data quality is improved. We have achieved an improvement rate of 80 per cent on our baseline data from 2009/10. Our strategy for the year ahead is to continue with our improvement rate and to implement an audit schedule that will monitor and track scheduled information governance audits. These will pay particular attention to: n Clinical record keeping through improved clinical governance procedures n Accuracy of data that relates to Mental Health Minimum Dataset Submissions n Information obtained on admission n Consistent use of the NHS number. 1. Our information is monitored for accuracy and completeness 2. We are registered to assess and treat people detained under the Mental Health Act 3. St Andrew’s complies with NHS national clinical coding Quality accounts for 2010/11 | 11 NHS Number and General Medical Practice Code Validity St Andrew’s Healthcare did not submit records during 1 April 2010 to 31 March 2011 to the Secondary Uses service for inclusion in the Hospital Episode Statistics which are included in the latest published data. Information Governance Toolkit attainment levels St Andrew’s Healthcare Information Governance Assessment Report overall score for 1 April 2010 to 31 March 2011 was graded as: To achieve a ‘satisfactory’ rating, we need to comply with level 2 in all requirements of the toolkit. Following an internal audit review in October 2010, a series of recommendations were made and our management team implemented a change management strategy. All but four of these recommendations have now been either fully resolved, or making good progress. Action plans are now in place to make sure we comply with the remaining requirements by December 2011. Current Score 42% Not Satisfactory Target Score 65% Not Satisfactory Clinical coding error rate St Andrew’s Healthcare was not subject to the Payment by Results clinical coding audit during the reporting period by the Audit Commission. 1 2 1. Our team is currently progressing a change management strategy 2. The charity is making good progress to measure up to level 2 of the toolkit 12 | Quality accounts for 2010/11 PART THREE TO THE ACCOUNTS On track with patient safety Keeping people safe is a top priority for St Andrew’s. We do everything we can to provide a safe and secure environment for service users, staff and visitors. There are five key ways that we do this: n n n Assessing and managing risks Building and maintaining well-designed hospitals (page 15) Recruiting, training and supporting staff (page 3) Assessing and managing risks The charity has grown in recent years and we now treat more service users than ever before. Table 1 shows how many registered beds we have managed over the past six years. We now manage 480 more beds than we did in 2005 - with an increase of 40 per cent in the last two years alone. Table 1: Number of registered beds 1200 1000 800 600 400 200 0 n n Delivering effective care and clinical treatment programmes (page 20) Sharing learning and best practice across the charity and beyond. St Andrew’s was the first mental healthcare provider awarded a full five-star rating by the British Safety Council. We’re determined to maintain this high standard, and during the year ahead, all of our national services will be assessed through an external audit of health and safety management systems. Minimising risks We work hard to minimise risks in our hospitals and use the safest equipment. Retractable needles are a case in point. EU directive 2010/32/EU requires all healthcare providers to use retractables from 11 May 2013, but we’ve used them since June 2009. Whilst they cost a little more, we’ve found using retractables means less injuries and less anxiety. Our needlestick incident reports are consistently low; just 11 incidents were reported last year, with no adverse outcomes. 2005 2006 2007 Number of beds 2008 2009 2010 Year ended 31 December We are also managing risks better. The total number of incidents reported in our hospitals has reduced by 40 per cent since 2007, even though we’re supporting more people. Table 2 shows our year-on-year performance. Table 2: Number of reported Incidents 18000 16000 14000 12000 10000 8000 6000 4000 2000 0 2005 2006 2007 Number of incidents Please note these figures include all incidents involving staff or patients. A lot of those things are quite small, but we report them because it’s the right thing to do. The number of serious problems is much lower, and this figure is also decreasing. 2008 2009 2010 Year ended 31 December Our Serious Untoward Incident reporting system helps us collect information consistently and has clear guidelines for investigating any problems that may occur. Quality accounts for 2010/11 | 13 1 Tackling challenging behaviours In 2010, St Andrew’s was the first secure healthcare provider in the UK to receive the RAID® Centre of Excellence Award from the Association of Psychological Therapies (APT). RAID® - which stands for Reinforce Appropriate, Implode Disruptive – is designed to tackle extremely challenging behaviours in healthcare settings. The system involves setting clear goals to aid individual recovery, such as working towards independence, or developing appropriate social skills. The process involves rewarding positive or ‘green’ behaviours in ways that help patients recognise their achievements; whilst ‘red’ (negative) behaviours are safely played down through the use of strategies such as distraction techniques. Chloe’s journey Chloe, a 28-year-old with Huntington’s disease, was admitted to St Andrew’s after a string of unsuccessful placements elsewhere. 1. We were the first secure provider to receive the RAID® Centre of Excellence Award from the Association of Psychological Therapies (APT) 2. The process involves reinforcing positive or ‘green’ behaviours in ways that help patients recognise their achievements On her arrival, Chloe ignored staff and refused to conform to ward routines. Due to self-harming risks, we provided enhanced support; she hid under the duvet and tried to avoid activities. She also showed physical and verbal aggression towards herself and other people, slammed doors, threw items of property around and routinely refused meals. 2 Through RAID®, Chloe’s goal was to be calm and motivated to engage in activities. The team did this in many ways, including: n Providing encouragement and incentives to help her get up n Using distraction techniques to tackle disruptive behaviour n Changing the environment to reduce risks to Chloe and others n Creating an activity timetable to promote positive actions n Giving her a designated ‘role’ on the ward. Changes in Chloe’s behaviour were measured through the Overt Aggression Scale - Modified for Neurorehabilitation (OAS-MNR). Over two years, her aggressive behaviours reduced from more than 50 incidents a week to less than 10. She has also progressed to a point where she: n Gets out of bed and eats meals without prompting n Is talkative and takes part in groups n Is highly motivated to try new activities, including bowls, horse-riding and pet therapy n Shows high levels of wellbeing n Consistently shows high levels of positive behaviour. 14 | Quality accounts for 2010/11 1 2 Progress against last year’s priorities Essen Climate Evaluation Scale (EssenCES) St Andrew’s aspires to be a teaching hospital, leading the way in healthcare. Research is important to check that our services are effective, and prove that we deliver high-quality treatment. Lots of research takes place at the charity. In 2010, members of our team were published 34 times, and delivered 39 national and international presentations. We also have a Therapeutic Practice Group that helps us to develop strong therapies with a built-in review process. The Essen Climate Evaluation Scale, or ‘EssenCES’, is a new measure of ward atmosphere and personality. It assesses engagement, patient motivation and perceived safety. Evidence suggests that patients respond better, engage more and recover more quickly where they feel safe and comfortable. St Andrew’s conducted research on EssenCES last year. We used the scale to assess ward atmosphere and identify any patient concerns, then use interventions to test if they made an impact. For example, we found that in some services, misunderstandings between service users were leading to individual friction and apprehension. So we developed an anti-bullying policy, ran some theatre workshops on diversity and bullying and helped service users to produce an anti-bullying leaflet. We then used EssenCES again to test the difference. We’ve found that patients moving through medium secure services who feel supported show fewer needs, fewer risk behaviours and are more likely to progress through the care pathway. the wider research community describes as key therapeutic factors. The work was recently written up by the charity’s Dr Clive Long. Linda has gone from strength to strength, having spoken at national conferences, presented her own content and fielded questions from mental health professionals. The fact that she has done this whilst unwell is impressive. Linda’s journey Linda had a severe and enduring mental illness, and was in medium secure care in St Andrew’s women’s service. She started attending service user group meetings, where a consultant spotted her potential skills articulating and presenting information. She showed an obvious interest in developing her skills further, so we looked for opportunities to do this. Last year, St Andrew’s supported Linda in developing a piece of qualitative research. This explored what patients feel makes a comfortable therapy setting (such as attitudes, staff and physical layout). Linda ran two focus groups, looking at what patients felt were positive factors in their treatment and learning what they value. Her findings were consistent with what 1. EssenCES assesses engagement, patient motivation and perceived safety 2. Patients respond better, engage more and recover more quickly where they feel safe and comfortable Quality accounts for 2010/11 | 15 Priorities for the year ahead EssenCES EssenCES remains an important priority for the year ahead. All healthcare providers must identify a service development or improvement, based on the surveys they did in 2010/11. At St Andrew’s, we intend to focus on patient perceptions of the ‘risk status’ system. 2 We are now producing an implementation plan to make sure that we achieve service improvements over the year ahead. This will be regularly tracked throughout the year, to make sure we meet what is required of us. Building and maintaining well-designed hospitals 3 With three new hospitals recently opened and ward refurbishments in Northampton, Birmingham and Essex, St Andrew’s is determined to provide well-designed healthcare environments. We want to create homely spaces that people feel comfortable living in as they recover. This year, the charity has developed a design guide which sets standards for the quality of our hospital environments. The guide builds on 1 1. A view of St Andrew’s latest development, William Wake House 2. Plans to upgrade one of the wards on the charity’s Northampton campus 3. Our Nottinghamshire facility, which opened in September 2010 the national regulatory standards, and includes information to make sure that any development or refurbishment meets and (where appropriate) exceeds those requirements. It also helps colleagues to learn from the charity’s experience and share information about environments and products for particular service user groups. The guide prevents unnecessary risks and identifies areas that may be susceptible to problems. This includes information on products tested, to minimise risk and encourage shared learning without stopping creativity. For example, if buying a new sofa, we will initially test it in a low-secure environment, against agreed criteria. If something works in that environment, we will consider whether it’s appropriate to test the product in a medium-secure setting. During 2011/12 we will work with service users to develop the guide further, and include specifications for specific room types. We will also be looking at room layouts and designs for seclusion areas; the Institute of Psychiatry has shown an interest in being involved in this work, possibly with a view to developing UK standards for seclusion environments. 16 | Quality accounts for 2010/11 Safe access to technology Education journeys Many secure mental healthcare providers routinely prevent patients from accessing technology. But St Andrew’s makes every effort to help people access technology for work, social, leisure and education use. In St Andrew’s College, we’ve installed eight interactive whiteboards, linked to individual student laptops. We can download thousands of lessons for the national curriculum using ‘SMART’ software. Everyone can access some form of technology, from gaming consoles, laptops and mobile phones through to PCs, Wiis and Playstations on our wards. We focus on managing access, rather than denying it altogether. The technology enhances lesson planning and student learning, and we use it all the time. It’s very visual for example, students can look at the positions of planets in the solar system – and kinaesthetic, as you can move words into sentences or shift body parts for a biology lesson. Teachers use pens to pick out key learning points from a lesson, then click a button to print the information; the equipment ‘understands’ their handwriting. As we support vulnerable people, we must risk assess individuals to ensure they access technology safely. Last year team members met with Nottinghamshire Police for training around access to information and the law, and best practice on disclosing information. St Andrew’s has a forensic IT security expert responsible for screening information and helping to assess machine capabilities. We share a technology ‘safe list’ with our Service User Group. We can also adapt equipment to patient needs, such as disabling Playstation browsers to allow gaming without Internet access. This approach has attracted plenty of interest, including visits from several NHS providers. In 2011/12, we will dedicate more resources and support to service users. This includes risk management training sessions and providing regional testing equipment. We’ve increased screening resources to track emerging technologies, and will evaluate video conferencing options for people whose families live overseas. 1 2 3 For some service users, such as young people with autistic spectrum conditions, it’s a very effective way of helping them focus into learning sessions. They can see things happening, and find this calming. Wiis are also linked to each machine. We use these to teach physical education GCSE, provide warm-ups to get the body and mind thinking and as ‘rewards’. There is scope to link in DVDs, music and sound; students can even write their own programs. 1. St Andrew’s College uses ‘SMART’ software to make lessons more engaging 2. The charity makes every effort to help people access technology, including accessing Wiis on wards 3. To maximise safety, a forensic expert is responsible for screening information Quality accounts for 2010/11 | 17 On track with clinical effectiveness Physical healthcare checks St Andrew’s supports patients to help them achieve optimal mental health and recovery. Our focus is on helping people to move into less secure settings, and back into the community wherever possible. Some people admitted into our care are very unwell, so it’s important to support and empower them in planning and managing treatment programmes. Their carers or families may need our help too. 1 1. St Andrew’s routinely assesses new patients for physical healthcare conditions and possible infections The Department of Health publication No mental health without physical health recognises that people with mental illness need good physical healthcare. People with mental illness often don’t access medical support; some patients admitted to us haven’t seen a GP for a long time. St Andrew’s routinely assesses everyone admitted to our hospitals for physical health conditions and possible infections. We also provide annual physical healthcare checks, including monitoring blood pressure, screening for chronic diseases and obesity and providing regular vaccinations. Our vaccination programme is already set to exceed the World Health Organisation influenza targets for the year ahead. The results are logged on our patient records system and trigger follow-up treatment where needed, so relevant staff can access key information immediately. For example, people with diabetes, asthma or heart disease are referred to clinicians for reassessment, and development of an illness-specific care plan. Alongside our physical health checks, we monitor service users’ diets and analyse the nutritional value of the food they eat. We screen their nutrition on admission and then every month; weight data is recorded on the patient records system, and Body Mass Index (BMI) figures are monitored on a graph. If someone is underweight, overweight or has had a major change in weight, the charity monitors their progress. High BMI patients usually enter the weight management care pathway. This involves a referral to therapists and access to a ward-based healthy lifestyle group, with information on food and activity choices. Interactive resources, factsheets and presentations are also available on our intranet. Healthcare providers need to promote healthy lifestyle choices. We encourage people to make informed decisions by coding menus and posting ‘traffic light’ nutritional content on food. In late 2011, we’re set to launch some service user workshops on tackling obesity. These sessions will use pictures and key words (such as ‘takeaways’ and ‘portion control’) to prompt debate. 18 | Quality accounts for 2010/11 Progress against last year’s priorities Recovery planning St Andrew’s uses a range of recovery tools to help people recognise where they are on their treatment pathway based on how they feel now, and where they want to be. The tools we use include Recovery Star, Teen Star, Dementia Care Mapping and Functional Independence Measure and Functional Assessment Measure (known as FIM-FAM). We know that different tools suit different people, and individual experience is also very important; after all, our service users are expert in understanding their life they have lived so far. One of our key targets for 2010/11 was to implement a recognised tool for recovery planning. We promised that every service user would be offered the chance to complete a recovery plan during 2010/11. Our progress towards this goal is shown in table 3 below. 1 Table 3: Compliance with recovery targets 2010/11 100 90 80 70 60 50 40 30 20 10 0 End of quarter 2 End of quarter 3 This information shows that we have made steady progress towards our target for the year. Some people have declined to take part in a plan; we will offer them the chance again End of quarter 4 every so often, in case they change their minds. Others haven’t completed a plan yet, that’s usually because they have been admitted in the last 12 weeks. 1. The charity uses a range of tools and information to track performance Quality accounts for 2010/11 | 19 1 2 Risk management Secure mental healthcare providers need clear guidelines in preventing and managing aggression. St Andrew’s is determined to provide the most sensitive support. We train staff in the prevention and management of aggression and violence; this helps us to prevent situations occurring, and reduce risks of injury to service users and staff. The charity has also trained nearly 400 staff to Level One Health and Safety. St Andrew’s uses a risk management tool called HCR-20 to assess service users and the people around them. This tool looks at patient history, clinical symptoms and risk situations. By being sensitive to risks that may affect people in our care and carefully managing potentially difficult situations, we can keep people safe without imposing unnecessary restrictions. Commissioners expect us to conduct HCR-20 with certain service users when they’re admitted to hospital, and then every six months. In 2010/11 we monitored 97 per cent of these ‘relevant patients’. Last year, Professor Chris Webster – one of the people who developed HCR-20 – ran an in-depth ‘train the trainers’ session and risk assessment workshop with clinicians. We produced a user guide in December 2010, showing staff how to log information on our patient records system. And over the year, we trained 83 staff to use the tool across our adult services. For 2011/12, St Andrew’s has developed an action plan to make sure we fully implement HCR-20; we have also set minimum standards to make sure that all elements of the tool are completed. During 2011 we will integrate the tool into individual care plans for relevant service users. We will also audit our standards next year, to check the quality of this work. 1. By being sensitive to risks and managing potentially difficult situations, we keep people safe 2. Training and auditing are key to managing risk successfully 20 | Quality accounts for 2010/11 Effective care and treatment Anna’s journey Delivering effective care and treatment programmes is very important to St Andrew’s. We’re constantly looking for ways to develop new ideas and improve services where this will benefit our service users. A healthcare professional who had experienced mental illness for many years, Anna’s pregnancy increased her paranoia and she tried to smother her child, leading to admission. She repeatedly attempted self-harming, including setting herself alight and suffering severe burns. In 2010, St Andrew’s women’s service developed a psychosocial treatment programme to support women with complex mental health needs. Many of these patients have experienced trauma such as physical, mental and sexual abuse; they typically have a history of high levels of risk to themselves or others, with challenging behaviours needing careful management. The charity has developed individual and group-based treatments, including problem solving, emotional regulation and interpersonal skills. Sometimes service users attend more than one group, to maximise treatment impact and speed recovery. The team has also developed creative solutions to help women assume personal responsibility and make informed choices. Achievements include training service users and staff together to use the Recovery Star, and piloting a self-assessment process where patients assess their own state and decide whether they should be given leave. 1 2 Anna joined St Andrew’s intensive programme, where the team helped her understand her illness and take responsibility for her own actions and safety. Initially suspicious, she was afraid to disclose some symptoms. Intense psychotherapeutic input (both through psychosocial groups and individual support) helped to change her ways of thinking, manage anxiety and challenge reality. A self-monitoring mood checklist helped Anna check her anxiety levels and perceptions of safety. Initially completed several times a day, Anna’s reliance reduced as her condition and confidence improved. Complementary vocational work boosted Anna’s self-esteem and she engaged much more effectively with the ward team, becoming open about her feelings. She gained sufficient independence to progress to a Community Treatment Order. Discharged in 2010, Anna now lives in the community and is engaged to be married. She and her family have written to the women’s service, thanking them for their support. 1. Nottinghamshire service users developed this Recovery Star diagram 2. Anna’s recovery journey has had a happy ending, with the announcement of her engagement Quality accounts for 2010/11 | 21 Priorities for the year ahead Care Programme Approach St Andrew’s follows the Care Programme Approach (CPA), a national clinical framework for supporting people with complex mental health needs. Every service user has an individual care plan, and an appointed care co-ordinator. Some service users have several plans that are rolled into one. (For example, if someone has a chronic physical illness, they may also have a detailed nursing plan or weight management plan.) The charity’s appointed care co-ordinators meet individual service users at least weekly to discuss their care plan and how things are going. In 2011/12 we will review St Andrew’s CPA processes, to bring together clinical practice and contractual requirements. This work will include refreshing our policy and agreeing key roles and 1 responsibilities. It will also involve reviewing our measures in line with the charity’s performance management framework. Service users’ views will be an important part of the process too. Recovery planning Recovery remains a strong focus for St Andrew’s. In a 2009 policy paper, the Centre for Mental Health listed 10 key organisational challenges facing mental healthcare providers. To address these challenges and help healthcare providers improve the way they work with service users, the Centre worked with the NHS Confederation and National Mental Health Development Unit to launch the Implementing Recovery, Organisational Change project (known as ImROC). ImROC involves changing service user treatment from a mainly clinical focus to one that puts recovery in the spotlight. Recovery puts service users at the centre of their care; it helps them to explore what’s right for them and live the best life they can, in the context of their mental illness. By working in partnership, the person’s life experiences and understanding of their own illness is recognised and valued. St Andrew’s has been selected as one of six national ImROC pilots, and the only independent sector provider. As a pilot site, we expect to review and challenge our existing services and find ways to build on existing good practice. We will have access to a two-year support package to help us. This includes input from expert consultants and trainers at the Centre for Mental Health, provision of training tools and guidance and attendance at ‘learning sets’ to share good practice. 2 1. Service users directly influence our work, as shown on this achievement wall 2. Dr Shawn Mitchell is the charity’s lead on the ImROC project 22 | Quality accounts for 2010/11 3 1 2 25 hours of activity Since 2007, medium secure healthcare providers have been required to provide 25 hours of therapeutic activity to each service user weekly. The scope of this time includes: n Directed psychological therapies n Occupational therapy, including life skills training and physiotherapy n Creative therapies, such as drama, art, music and animation n Complementary therapies, aimed at improving self-image n Educational and vocational training - including both life skills and practical skills (such as bricklaying) n Voluntary placements and academic development n Weight management, exercise and diet n Self-directed activity, including hobbies and leisure. St Andrew’s follows the 2007 Offender Partnerships Best Practice Guidance for Mental Health Services. Activity and engagement are often closely linked, so we aim to get service users fully engaged in focusing on their recovery. That way, they understand what is happening and can sign up to the benefits of getting involved. For example, if someone has been in and out of a psychiatric setting for years and on medication for a long time, it may be hard for them to acknowledge an obesity problem. But until they do, the success of weight management activities may be limited; so we encourage them to think about where they are now, and what they need to do to move on. St Andrew’s routinely sets challenging targets to exceed the basic 25 hour figure. For example, our new men’s service at William Wake House has set a target of at least 30 hours of activity in 2011/12. This unit achieved a ‘top five’ position in the country in a peer review, less than three months after opening. Although we’ve worked hard on the practical side of things, our current systems don’t produce clear and concise information. So in 2011/12, we will develop a new performance framework. We’re adapting the ‘community diary’ on our patient records system to develop a timetable module, and help us to record and report activity hours. The software developer is helping us to make these changes ready to launch in late 2011. Another key action for the year ahead involves aligning our systems and treatment programmes with the new, agreed national definition of ‘meaningful activity’. St Andrew’s intends to achieve the targets set nationally. This includes auditing services using the new sector benchmarking tool and implementing a work plan to address any needs arising from the audit. 1. Learning woodwork helps patients to build confidence and practical skills 2. Animation techniques can tell a strong story, as this example shows 3. Figures developed by service users in our Northampton creative studio Quality accounts for 2010/11 | 23 Enhancing physical healthcare Physical health is still a key priority for St Andrew’s. In the year ahead, we want to help service users with diabetes manage the condition themselves. A high proportion of people referred to us have diabetes; around 10 per cent of service users are diabetics, compared to a national average of four per cent (source: Diabetes UK, 2009). In December 2010, we piloted a structured six-week programme to help diabetic patients look after themselves. This included: n n n Pre- and post-programme blood pressure, lipids and blood glucose checks to test the impact on participating service users Conversation maps, developed with Lilly’s diabetes education section, to train 25 staff in guiding discussions around topics such as food, lifestyle and feelings A ‘takeaway’ resource covering issues such as blood glucose levels and self-monitoring. The pilot is now being evaluated before we extend it charity-wide later this year. We will also share its resources online, to help staff support service users. We aim to achieve the National Institute for Clinical Excellence quality standards for diabetes in adults by year end. Bob’s journey Bob was admitted with paranoid schizophrenia. On admission, our routine checks showed that he had Type 2 diabetes, with an average blood sugar level of 11.9 per cent using the ‘HbA1c’ test (which measures sugar levels over three-months). Bob had been diabetic for many years, but he’d never done anything to monitor or regulate the diabetes. This meant he faced other health risks, such as blindness, heart attack or stroke. An important change involved getting Bob to understand his relationship with food, and how it affected his physical and mental health. We helped him review his diet, change his eating habits, start a regular exercise programme and adjust his diabetic medication. He started making healthier food choices, and changed his attitude to snacking between meals. Within a month, Bob’s average blood sugar level reduced to 10.9 per cent. He now manages his diabetes well. He keeps a food diary and blood sugar diary, to monitor what he’s eating and how it affects his sugar levels. His glucose level is now an average of 10.0 per cent, which is a big improvement. 1 Bob joined our weight management care pathway as part of his treatment programme. He worked with a practice nurse, dietician and ward nursing staff to get the diabetes under control. 2 1. Conversation maps guide discussions around food-related topics 2. Healthy eating education helps people like Bob to make more informed choices 24 | Quality accounts for 2010/11 On track with patient experience The way that patients experience our services is critical to any quality assessment of St Andrew’s. Almost every service user at St Andrew’s gets involved in giving the charity feedback or ideas. We involve people in their care and treatment and as many areas of hospital life as possible because: n They know best what is right for them n It helps us to target services better and understand which outcome measures are most helpful n It’s more efficient to listen to them - and get services right first time n It helps them to feel valued, important, know their opinion counts and that the charity cares about what they have to say. Our engaged service users are at all stages of the recovery journey. Some can be very unwell, having chronic or multiple disorders. But anyone can be involved if they want to and there are many ways of taking part: from ward discussions, satisfaction surveys and minor projects through to work placements, training, governors’ events, parties and formal groups such as the service user contributor scheme. We even involve patients in recruitment, including interviewing clinicians, ward and administration staff. 1. Helping people to build their confidence and achieve their potential is core to what we do Some highlights from our service user involvement programme are explained throughout this section. There are not enough pages to explain everything we do in detail, such as involving patients in service improvements, induction training and developing a user handbook. But we can emphasise that helping people to build their confidence and achieve their potential is a core part of what we do. Last year we supported service users to become befrienders, train our team on ‘what it’s like to be a service user’ and speak about mental health issues at national conferences. Where people show an interest and it’s good for their development, we work hard to help them grow. 1 Tom’s journey Tom was admitted to a medium secure ward at St Andrew’s following a history of profound drug misuse and numerous arrests. During his stay, Tom showed an interest in learning; we found out that he had formerly been interested in studying higher education. With support and encouragement, he started to study for a university degree. As he recovered, Tom’s motivation remained strong. When he returned to community life, he continued the qualification, and successfully completed a degree in business studies. Quality accounts for 2010/11 | 25 Progress against last year’s priorities Diversity Everyone is unique, with their own special strengths and qualities. In a secure mental healthcare setting, this can be challenging as some people may not always understand or tolerate each other’s behaviours and needs. In 2010, St Andrew’s developed a diversity questionnaire for staff. Service users helped to develop questions for this. The questionnaire was sent to heads of departments, asking them to review local practice. We also helped service users to construct a patient survey. This asked questions such as: n Do you feel respected? n Are your cultural needs being met? n Does our dining experience meet your needs? n Would you benefit from diversity awareness training? From a population of 667 patients, 227 gave us their views – a 34 per cent response rate. Most people said their cultural needs are met; where people did have unmet needs, these concerned religion, food, decisionmaking, music or acceptance by other people. Some 69 per cent of service users who replied said they can be 1 themselves at St Andrew’s. However, 29 per cent of patients said they had been bullied and 73 per cent of patients told us they would benefit from awareness sessions, to encourage greater respect for differences among service users and staff. So we took urgent action to change this (see page 14). Since the survey, St Andrew’s has taken several steps to help people respect individual differences. For example, we developed interactive training to help people recognise and celebrate different ideas and cultures – including elements delivered by service users to their peers. One tool, a visual training wheel with ‘true’ and ‘false’ cards, uses statements based on patient experiences to challenge why people think in a certain way. The charity also developed a spirituality needs assessment tool last year. We went to great lengths to identify spiritual leaders across many faiths; service users can request support and input from a leader of their chosen faith and we will provide access. We are also considering creating a series of groups in response to the survey. These include a lesbian, gay, bisexual and transgender group, as well as activity-based groups around music, film and sport. 2 1. This questionnaire helped us to explore service users’ views on diversity 2. The anti-bullying leaflet was developed following our diversity audit 26 | Quality accounts for 2010/11 1 2 On track with patient experience Service user contributor scheme St Andrew’s provides a huge range of voluntary opportunities for service users to contribute to the charity’s work. Examples include clerical support, gardening, helping in our shop and hairdressing salon, attending meetings and befriending other patients.Taking part makes people feel valued and important, helps build self-esteem and prepares them for life back in the community. Voluntary placements can also turn negative perceptions of mental disorder into positive experiences, as service users contribute their life experience to improve things. Some service users have severe mental illness, learning disabilities or acquired brain injuries but can still benefit from learning new skills and connecting with other people. 1. Gardening is one way in which service users can contribute to St Andrew’s work 2. This hairdressing salon is a focal point in the hospital community When a patient is admitted to St Andrew’s, we offer them access to befrienders and explain what opportunities are available to them. When someone contributes their time, they accrue service hours. As they build up these hours, service users are rewarded with a range of benefits - such as certificates, cards, presents and invitations to social events with other charity supporters. St Andrew’s also has ‘Oscars’ for people who complete 100 hours of service, and gifts for people completing 200 and 300 hours. By contributing time and energy, individuals can build up a portfolio of evidence ready for their future discharge and potential employment. So there are many positive reasons for people to get involved. John’s journey John was originally admitted to a medium secure ward, where he found it hard not being able to go shopping and get the things he wanted. When he progressed to low secure care and was able to get out and about more, John mentioned his former frustrations and showed an interest in helping other service users going through similar experiences. So John’s occupational therapist helped him develop a plan to help him become an unofficial ‘personal shopper’ for medium secure service users. There were lots of things to consider in making this happen, including risk assessments, training and support. But St Andrew’s has helped John to overcome those barriers. He now enjoys fetching errands for people, bringing back their receipts and so on. It’s also good for his peers, who feel that a friend is doing them a favour rather than feeling dependent upon our staff to shop on their behalf. Quality accounts for 2010/11 | 27 1 2 Priorities for the year ahead “I like it when I’m covered up.” “Feels good inside, treatment becomes easier, being looked after well.” “Being looked after properly.” “To feel like I’m important when staff care for me.” “Showing me what I feel and think matters.” “Feels like I’m treated well. Respected. Dignity means private.” Dignity Helping vulnerable service users to retain their dignity is hugely important to St Andrew’s. We want to make each patient’s experience of our care as positive as possible, recognising individual talents and needs and supporting people whilst they’re with us. Some service users are very unwell and it’s important to do as much as possible, so people can take pleasure in the little details of everyday life. St Andrew’s follows the Department of Health’s 10-point dignity challenge. This aims to help people understand what providers are doing to improve quality of life for their patients. Last year the charity conducted a dignity audit. We asked 122 service users what they thought being treated with dignity feels like, and 67 people responded. Some of their feedback is shown above. During 2010/11 St Andrew’s has introduced several service improvements to enhance dignity, including: n Introducing a ‘clean face’ policy, to make sure more vulnerable residents maintain their dignity after mealtimes n Providing training (using the Royal College of Nursing’s dignity pack) to remind staff of the importance of dignity - this involved staff feeding each other with blindfolds on, and being pushed around in a wheelchair, to show how service users may feel in certain situations n Installing frosted windows on a ward where people walking past could previously look in, to improve service user privacy n Developing life story books to help ward staff and befrienders connect with patients (for example, they can see that the service user used to have a particular car, or support a sporting team) n Launching a ‘hospital passport’ system, which records factors that are important to service users and will make them feel comfortable – such as having a bedside light, or wearing bright colours. St Andrew’s is set to review its dignity, choice and care policy by June 2011. Through this work, we will identify actions and key milestones required to ensure our approach to dignity still meets the very latest industry practice. 1. We work hard to help people take pleasure in the little details of everyday life 2. Service directors make sure that our approach to dignity meets the latest industry practice 28 | Quality accounts for 2010/11 “Service user satisfaction with our food is consistently around 80 per cent. We collect feedback at service times, in meetings between chefs and service users and through quarterly surveys.” Dining experience Dining at St Andrew’s is very important. It affects our service users’ quality of life, and is a topic they like to discuss. And of course, diet is an important factor in improving mental and physical health. Since 2009, we have completely overhauled our catering services to focus more on local, organic and ethical produce. A central electronic ordering system controls the products staff can buy, so they can only use healthy options. (For example, sources of ‘trans fats’ have been removed from our purchasing list.) Meals are cooked and served locally to the wards. Service user satisfaction with our food is consistently around 80 per cent. We collect feedback at service times, in meetings between chefs and service users and through quarterly surveys. We’re sensitive to people’s needs and preferences, with eight bespoke menus catering for different groups. Following last year’s diversity survey (page 25), we extended our dining experience to include halal and kosher produce. We also organise themed days linked to religious festivals and serve culturally-relevant food. The charity has analysed and reviewed its menus for some time, taking advice from specialist dieticians. In 2010 we started formally testing the nutritional value of our chefs’ recipes using nutrition analysis software. Each recipe is tested for 14 nutrients (including vitamins, fats and salt) and checked against recommended dietary allowances. A traffic light system highlights the nutritional value of each recipe; this helps us to assess ways of refining ingredients and cooking methods to make options even healthier. The final recipes are priced according to agreed portion controls, and shared on the staff intranet. Our chefs can analyse a week’s menus in advance, knowing they’re achieving a balanced diet. 1 2 The first batch of recipes is online. Our priorities for 2011/12 are to complete the analysis of all recipes and publish the ‘healthiest options’ on the intranet. This will include an online ‘menu builder’ where chefs can pick items from a list. We also aim to maintain high levels of service user satisfaction. One way we plan to achieve this is by building service user awareness of food production. Work is underway to develop herb gardens for the charity’s kitchens. In spring 2011 we will also support service users in planting fruit and vegetables on-site, helping them to see the benefits of growing healthy produce. 1. Meals are cooked and served locally to our wards, with service user satisfaction consistently around 80 per cent 2. Each recipe is tested for 14 nutrients and checked against recommended dietary allowances Quality accounts for 2010/11 | 29 Involvement and personalisation strategy As this section proves, St Andrew’s is dedicated to providing a wide range of opportunities for service users to get involved in shaping the charity’s work. People can contribute formally through work-related tasks, informally through activities and feedback, and of course influence the recovery process. A strong example of how we encourage service user input to develop charity practice and enhance recovery is shown below. Care Pathway Star Service users from all the charity’s sites and services have been involved in delivering a new assessment tool, the Care Pathway Star. This is based on the Recovery Star, but is intended for in-patient settings. There are some key differences between the two tools. For example, the top point of the Recovery Star is self-reliance; on the Care Pathway Star, it’s moving on (which could mean moving from medium to low secure care, or back into the community). 1 1. St Andrew’s is dedicated to providing many opportunities for service users to shape our work St Andrew’s is one of four secure organisations developing the Care Pathway Star, and service users and staff have collaborated together on the work. Service users from Birmingham, Essex and Northampton developed descriptors for all 10 points of the star and we received positive feedback from a Mental Health Providers Forum representative. In spring 2011, service users and staff will join forces to develop the final tool, ready for publication by September. We expect the star will be a huge benefit to service users in future. During 2011/12, we will bring our work into line with the new national framework. By June 2011 we will have developed a new service user involvement strategy for the charity, linked to the national service user groups. Throughout the rest of the year, we will implement the strategy to make sure that we continue to support people in developing their skills, potential and confidence. Working with service users, we will also produce a report showing how the charity can achieve the choices made by patients for the year. 30 | Quality accounts for 2010/11 Mapping feedback In producing this document we have listened to the views of staff, service users, commissioners and other partners who have an interest in our work. Thanks to everyone who has been kind enough to submit ideas and comments; we appreciate your views and know this will help us to keep improving what we do. The list of people formally consulted on these accounts includes: n Strategic commisioning managers n Service user groups n Colleagues at St Andrew's. The feedback received is shown below. We are also grateful to our Board of Trustees for its continued commitment - providing independent input through service visits and challenges, and scrutiny through our committee structure. “In principle it looks fine to me, I wouldn’t suggest any major amendments.” Mick Burns, Senior Commissioning Manager, Yorkshire and Humber region "I have looked through the report and think that once it is complete it will be a very good read and extremely informative." Yvonne Srinivasan, contract lead, East of England Specialised Commissioning Group Quality accounts for 2010/11 | 31 Key connections Partnership working is very important to St Andrew’s. We work with hundreds of people and organisations to support service users, develop and manage services and share best practice. Diagram 1 below outlines some of the key partners we work with, and what we achieve together. Diagram 1: partnership working at St Andrew’s Networks Carers Share best practice and influencing opportunities Share knowledge and understanding to support people Governors Communities Help us to prepare people for life St Andrew’s Provide an independent view of our work Service users Researchers Regulators Discover and share information to improve quality of care Check we’re upholding the law and meet national standards Education specialists Partner us to provide learning opportunities Commissioners Work with us to provide safe and suitable placements Northampton Billing Road Northampton NN1 5DG Birmingham 70 Dogpool Lane Stirchley Birmingham B30 2XR Essex Pound Lane North Benfleet Essex SS12 9JP Nottinghamshire Sherwood Avenue Sherwood Oaks Business Park Mansfield NG18 4GW T: 01604 616000 T: 0121 432 2100 T: 01268 723800 T: 01623 665280 Registered charity number: 1104951