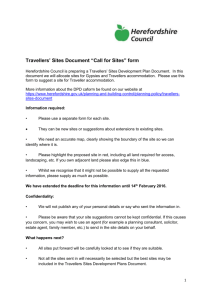
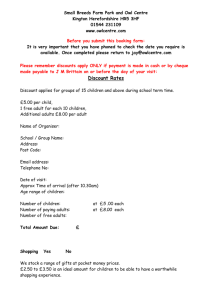
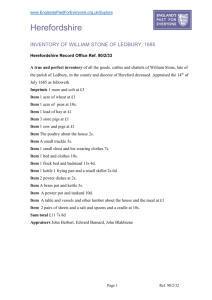
Quality Account Herefordshire PCT: Provider Services
advertisement

Quality Account Herefordshire PCT: Provider Services 2009 - 2010 Our Mission ‘To deliver high quality, safe and sustainable health and well being services tailored to meet the needs of our local community.’ Headquarters: Vaughan Building, Ruckhall Lane, Belmont, HEREFORD HR2 9RP PART 1 Content PART 1 MANAGING DIRECTOR’S STATEMENT STATEMENT OF ACCURACY PART 2 1 LOOKING FORWARD - The Next 12 Months in Herefordshire Page 5 1.1 Our Quality And Safety Priorities For 2010/2011 5 1.1.1 Patients/ Service Users as Partners 5 1.1.2 Improving Quality Through Local Service Partnership 6 1.1.3 Continuing to Improve the Recording of Incidents in All Services and the Sharing of Lessons Learned 7 1.1.4 New Patient Information System 8 1.2 2010 – 2011 CQUINs 8 1.2.1 Community Service Goals 8 1.2.2 Mental Health Service Goals 9 2 Statutory Statements of Compliance 10 2.1 Records 10 2.2 Audit 10 2.3 CQUIN Payments 10 2.4 Information Governance Tool Kit 10 2.5 Payment by Results 11 2.6 Statutory Visits 11 2.7 Research 11 2.8 CQC Registration 11 PART 3 3 LOOKING BACK – Our Services and their Achievements 2009 - 2010 12 3.1 Demographic Context 12 3.2 Organisational Context 13 4. PATIENT SAFETY 14 4.1 Key Safety Indicators 14 4.2 Reducing Serious Untoward Incidents 15 4.3 Compliance with MRSA Screening Process 16 4.4 MRSA Rates 16 4.5 Clostridium Difficile (Cdiff) Rates 17 2 5. CLINICAL EFFECTIVENESS/ QUALITY MEASURES 17 5.1 Essence of Care 18 5.2 Reducing Mixed Sex Accommodation 18 5.3 PEAT (Patient environment action team) 18 5.4 Compliance with NICE Guidance 5.5 Comply with National Target for 18 Weeks from Referral to Treatment in Consultant Lead Services 5.6 Compliance with CQUIN Requirements 5.7 Service Specifications Written and Quality and Performance Indicators/Activity Indicator Metrics Agreed 5.8 Improve Data Quality 19 20 20 20 21 6. PATIENT EXPERIENCE 21 6.1 Mental Health Services 21 6.2 Sexual Health Services 21 6.3 MacMillan Nurses 21 6.4 Recruiting Student Health Visitors and School Nurses 22 6.5 Physiotherapy – Patient Reported Outcomes Measures 22 6.6 Parkinson’s Nurses 22 7. SERVICES REVIEW 22 7.1 Service Review by Care Quality Commission 22 7.2 Delays in Discharges from Inpatient Care 23 7.3 Management of Complaints 23 8. SERVICE IMPROVEMENT 24 8.1 Podiatric Surgery 24 8.2 Community Hospitals and Intermediate Care 25 8.3 MacMillan Nurses 25 8.4 Community Intermediate Care 26 8.5 Physiotherapy 26 8.6 Occupational Therapy Service 26 8.7 Intermediate Diabetes Service 26 8.8 Acute Mental Health Services 27 8.9 Apprenticeships 27 8.10 Change Champions 27 8.11 What Others Say About Us 8.12 Herefordshire Council: Health Scrutiny Committee - Commentary on Herefordshire PCT provider Services Quality Accounts 28 29 3 PART 1 Managing Director’s Statement April 2009 saw the introduction of NHS Herefordshire Provider Services as an arms length provider organisation from Herefordshire Primary Care Trust. Through the year 2009/2010, Provider Services Board, Senior Managers and front line staff have been working to deliver safe, quality care for the people of Herefordshire, and this is reflected in our first Quality Account. We are proud of the progress we have made against our core objectives, whilst acknowledging that we have a challenging agenda and there is no room for complacency. We know that there is a lot of work to do and we shall need to continue to push ahead in the next year to bring these to fruition. We trust that this report helps demonstrate that we are listening to what patients and carers are telling us; we have continued to deliver the excellent infection control performance we inherited from our parent organisation; and we are committed to monitoring and improving patient safety. We are also committed to making patients, their families and the wider public, partners in the delivery of health and social care in Herefordshire. Our Quality Account 2009/10 establishes a baseline against which we will monitor our progress in 2010/11 against our safety and quality targets and sets out our vision for the future. Richard Carroll Interim Managing Director of Provider Services Statement of Accuracy: All Services (see section 4.2) delivered by NHS Herefordshire Provider Services have been included in the scrutiny and assurance process. To the best of my knowledge the information contained within this Quality Account is accurate. Lynda Steele MPhil, DCR(R), SRR, MHSC (cert) Associate Director of Quality and Clinical Effectiveness 4 PART 2 1 Looking Forward – The Next 12 Months in Herefordshire The next 12 months promise to be no less challenging and interesting than the last. We and our partners in local health and social care delivery are currently consulting with the people of Herefordshire on the way services shall be provided in the future as part of the Shaping Health and Wellbeing in Herefordshire programme. Whatever the outcome, the closer working relationships which have been developed during the last 12 months to improve patient care will become even stronger. Safe, quality cost-effective services can only be delivered in a co-ordinated and co-operative way and this is well recognised by the organisation and our partners. In an economic climate which dictates even closer scrutiny of every penny spent, it is vital that the patient remains at the centre of the care package, and remains our focus. We intend to do this whilst continuing to focus our attention on the services around that person, and to reduce duplication and unnecessary steps which can lead to poorer care and increased cost. As part of this drive for efficiencies, in 2010 Podiatric Surgery are starting to use a Productive Operating Theatre Programme, (which is similar to the Releasing More Time to Care programme – see section 8.2) using LEAN methods to work out how they could work in a more efficient way. 1.1 Our Quality and Safety Priorities 2010/2011 The organisational form which evolves from the consultation and the economic climate will create a need to more clearly define the key priorities for the next 12 months. For this reason the priorities which are outlined in this report are broad and will continue to be shaped by the formation of new organisational boundaries. There are three areas where we will be focussing attention: 1. Patients/ Service Users as Partners 2. Improving Quality through local service partnerships. 3. Continuing to improve the recording of incidents in all services and the sharing of lessons leaned. There are a further two areas where we will also be looking to improve: 4. Improving Clinical engagement with our key priorities. 5. Continuing to improve patient information systems. 1.1.1 Patients/ Service Users as Partners One of our targets is to improve the collection, analysis and use of patient experience. A programme manager has Success Story A 14 year old young person with Cerebral Palsy, having limited mobility, had an operation resulting in the person not being able to stand or walk. Surgeons thought it would take up to 2 years for maximum function to return. Daily support from specialist Children’s Physiotherapists meant that in 6 weeks the young person was walking independently. 5 PART 2 recently been appointed and started work in Herefordshire in April 2010 and is focussing on the best way to improve the consistency and collection of patient experience information and comments. She will also set in place processes to improve the sharing and use of that information across the organisation, to enable services to improve in response to patient experience. We will be taking patient experience forward in line with the Darzi Next Stage review 2008, and will seek to populate the report required in 2011 with data we are starting to capture now. We will take a two strand approach to the generation of the report, looking at both the measures from metrics (generated from the service and user and carer questionnaire) and the narratives from patient voice information, across both health and social care. We will be working closely with as many groups as we can, to ensure that their voice is heard, and that we use this to develop meaningful improvements in patient focused care. We will also be working towards the CQUIN target, which is a method for Commissioners to reward Providers of services, based on good patient experiences and we hope our service users will feel confident in telling us when we have met their needs. We also aim to expand in the year the use of NHS choices as part of our patient experience work. 1.1.2 Improving Quality through Local Service Partnerships This year we will implement the care pathway work undertaken in 2009/10. During the last 6 months Provider Services has been working with local partners to deliver care in a more co-ordinated manner which more closely considers the delivery of care closer to home. Clinical staff from all organisations have come together to consider national guidance and local needs and they have taken all information available to determine how the best most effective care can be provided for the people of Herefordshire. The following areas have developed new care pathways which will transform care delivery: • Low Back Pain • Stroke • Frail Elderly • Diabetes • Respiratory Conditions Mental Health Services are currently exploring working as partners with another provider service, and this new way of working should allow for a broader service to be delivered to people who require support. Subject to the outcome of local consultation a new provider organisation will potentially be in place by 1st April 2011, and services may begin to change towards that new organisational structure in the autumn of 2010. 6 PART 2 Our Training Team will be supporting the development of our current and future workforce. Apprenticeships will continue to be supported by our organisation as we recognise the future stability of the local services depend on recruiting people locally. To further enhance our connections with local young people and to help develop skills amongst the local workforce, money has been successfully obtained to develop a facility to help young people understand the work of the NHS. This consists of a training environment including a “mock up” of someone’s home with working equipment to show them what really happens if you are caring for someone at home and how to react in a medical emergency situation. This facility will also be used to support training and development for our own and hospital staff. This will be the first time such advance training facilities have been available locally, and this means we will not have to send people away for training, cutting travel costs, CO2 emissions and can train and develop more people for the same cost. 1.1.3 Continuing to Improve the Recording of Incidents in all Services and the Sharing of Lessons Leaned The Corporate Risk and Quality Teams are supporting the development of the team leaders in the organisation to enable them to better support all staff in the reporting and management of incidents. They will also be improving the way that information is made available to teams so that teams are able to see trends that need to be addressed. They will also be training staff and supporting the investigation of incidents and complaints using the Root Cause Analysis methods, which help to clearly identify system failures and support the development of the improvement of these systems. Three training sessions will be delivered to staff Team Leaders and ad hoc support will be offered when required. One report will be delivered to each of our service directorates every three months, trends and issues will be identified and actions identified. We will Success Story also be producing information sheets to highlight areas of good practice and 4 out of the last 5 clinical lessons learned, to share with other assistants in community services. All such lessons will also be Psychology have gained shared through governance meetings places on Doctoral Courses across the organisation. due to the support and example of local team and In liaison with the Infection Control Team mentorship of local Clinical and our service partners we will ensure Psychologists. we learn lessons from incidents which occur and use our learning to further The most recent assistant won improve the safety of patients, their a place with only 20 on offer families, the general public and our own and in competition against 200 staff. others. 7 PART 2 1.1.4. New Patient Information Systems Herefordshire is in the early group of Trusts introducing new patient information systems in the next few years. In 2010 – 11 the Podiatric Surgery and Children’s Safeguarding teams will be pioneering the use of a new national IT system called Lorenzo, which will connect teams together and link to the general health information held within existing national confidentiality and Information Governance requirements. Clinical leaders and Information programme planners are working very closely to make this a successful transition. 1.2 2010 – 2011 CQUINs In the next 12 months there are a number of targets (Goals) which have been added to the requirements for reporting on new services and improved effectiveness. These are listed in the CQUIN for the next year: 1.2.1 Community Services Goals 1 Patient Experience - Improving the experience of Patients receiving Community Hospital services and patients receiving community based health services. 2 Percentage of smokers/tobacco users attending outpatient clinic appointments receiving a brief intervention to reduce tobacco use including being given written advice. 3 To implement best practice care in hospitals in the West Midlands for the care of inpatients with a secondary diagnosis of diabetes and as a consequence reduce associated healthcare costs. 4a All patients on admission (and within a minimum of 24 hours) should be assessed by a suitable competent and experienced Registered Nurse for their risk of developing a pressure ulceration using a recognised evidence based tool. (Exclusions would be paediatrics, day cases, maternity (if any). 4b Inpatients assessed to be at risk of ulceration or who currently have a pressure ulcer will have preventative actions taken and documented in their care plan. 4c Percentage decrease on numbers of hospital acquired grade 2, 3 and 4 ulcerations demonstrated by Q4 against baseline level established in Q1. 4d All hospital acquired ulcerations of grade 2, 3 or 4 will be recorded on the appropriate system and a Root Cause Analysis commenced within 5 working days. 4e All ulcerations which show deterioration from grade 2 to 3 or 3 to 4 will be recorded as a serious untoward incident on the appropriate system. 5 Patients will have a falls risk assessment completed on admission to Community Hospital (within a maximum of 24 hours) or initial contact with community team. For those identified at risk, an individualised falls care plan will be implemented. 8 PART 2 6 Patients will have a nutrition assessment completed on admission (within a maximum of 24 hours) to Community Hospital or initial contact with community team, using a nationally recognised tool. 7 The number of patients who have died whilst on a GSF register, have a supportive care plan and have been managed on a supportive care pathway. 8 To promote effective Discharge Planning. Development and completion of a standardised discharge care plan. 9 To improve patient safety management in relation to medication administration. 1.2.2 Mental Health Service Goals 1 Productivity and Pathways Improvement Programme. 2 Patient Experience - Improving the experience of Patients receiving Community Mental Health services and patients receiving hospital based Mental Health Services. 3 Percentage of smokers/tobacco users attending outpatient clinic appointments receiving a brief intervention to reduce tobacco use including being given written advice. 4 Supporting Social Inclusion Opportunities by assessing accommodation and employment status and security. patients’ 5 All Patients have the opportunity to be treated in their own home. 6 Failure to administer prescribed medicines as a result of non-availability of the medicine. 7 Dementia Pathway Development. Development of a Dementia Pathway for the mental health trust elements of the pathway in partnership with all key stakeholders. Ensuring people are following the Dementia Care pathway. 8 Ensuring that use of leave from hospital admission is a clinically managed part of all patients’ in-patient length of stay. 9 Reducing the incidents of broken engagement with service users of Assertive Outreach Teams. 9 PART 2 2 Statutory Statements of Compliance 2.1 Records “Herefordshire PCT Provider Services did not submit records during April 2009 – March 2010 to the Secondary Uses service for inclusion in the Hospital Episode Statistics which are included in the latest published data.” 2.2 Audit During the period April 2009 to April 2010 Herefordshire PCT Provider Services participated in one national clinical audit and one national confidential enquiry of the national clinical audits and national confidential enquiries in which it was eligible to participate. The national clinical audits and national enquiries that Herefordshire PCT Provider Services participated in, and for which data collection was completed during October 2009 was for the National Clinical Recordkeeping Audit. All teams in the organisation scrutinised 10 sets of patient records and information was analysed and provided as part of the Information Governance Tool Kit. There were three national confidential enquiries which occurred in 2009/10: • National Confidential Enquiry into Patient Outcome and Death (NCEPOD); • Centre for Maternal and Child Enquiries (CMACE); and • National Confidential Inquiry (NCI) into Suicide and Homicide by People with Mental Illness (NCI/NCISH). 2.3 CQUIN Payments A proportion of NHS Herefordshire Provider Services income in April 2009 – March 2010 was conditional on achieving quality improvement and innovation goals agreed between NHS Herefordshire Provider Services and NHS Herefordshire Commissioners and any person or body they entered into a contract, agreement or arrangement with for the provision of NHS services through the Commissioning for Quality and Innovation payment framework.” “Further details of the agreed goals for April 2009 – March 2010 and for the following 12 month period are available on request from the Clinical Governance lead for NHS Herefordshire Provider Services. 2.4 Information Governance Toolkit NHS Herefordshire Provider Services score for April 2009 – March 2010 for Information Quality and Records Management, assessed using the Information Governance Toolkit was 93%. 10 PART 2 2.5 Payment by Results “Herefordshire PCT Provider Services was not subject to the Payment by Results clinical coding audit during year April 2009 to March 2010 by the Audit Commission.” 2.6 Statutory Visits The Mental Health Service has participated in a special review by the Care Quality Commission during 2009/10. The special review was conducted by the Mental Health Act Commissioner on Jenny Lind Ward, Stonebow Unit, on 23rd January 2010. The Mental Health Service intends to take the following action to address the conclusions or requirements reported by the CQC: • Development of Patient Information Pack. • Ensure Care Co-ordinators attend ward reviews regularly. • Develop formal system of supervision. • Ensure corridor toilets are gender specific. • Day rooms are identified for gender specific use. The Mental Health Service has made the following progress by 31st March 2010 in taking such action; • Patient Information Packs have been completed and are in all patient rooms. • Action plan for the development of formal supervision is being developed. • Corridor toilets are gender specific. • Day rooms are identified for gender specific use. 2.7 Research The number of patients receiving NHS services provided or sub-contracted by Herefordshire PCT Provider Services from April 2009 to March 2010 that were recruited during that period to participate in research approved by a Research Ethics Committee was nil. 2.8 CQC Registration Herefordshire PCT is required to register with the Quality Commission and its current registration status is: ‘Registered without conditions’. The Care Quality Commission has not taken enforcement action against Herefordshire PCT during the period between April 2009 and March 2010. 11 PART 3 3 LOOKING BACK - Our Services and Achievements 2009 - 2010 NHS Herefordshire Provider Services was established in 2009 as an arms length provider organisation. At the outset it set as its vision ‘to be recognised by the local and wider communities as the health and well-being services provider of choice.’ With a mission ‘to deliver high quality, safe and sustainable health and well being services tailored to meet the needs of our local community.’ 3.1 Demographic Context Herefordshire is a predominantly rural county with six centres of population: With a population density which is the 4th lowest in England this means that many key services are further away from residents compared to other parts of the country so only about half of residents are within 4km of a GP (48%) and one Success Story third (34%) within 4km of a supermarket. The Falls Prevention Team Coupled with limited public transport it is particularly important therefore that we started Staying Steady Groups work hard at ensuring that local services in Ledbury, Leominster and are delivered as close to residents as Hereford. In January they possible. started more groups in Ross The Black and Minority Ethnic (BME) population is steadily rising; however, it and Bromyard. This has lead represents 4% of the Herefordshire to improved independence for population compared to 16% nationally. many people across the county 12 PART 3 3.2 Organisational Context Provider Services delivers care across the county. The organisation is led by a Managing Director and operationally has five Directorates: • • • • • Adult and Older People Services Mental Health Services Specialist Services Children’s Services Social Care. Adult and Older People Services Children’s Services Specialist Services Mental Services 3 Community Hospitals Safeguarding Children Podiatric Surgery Acute Mental Health Services Intermediate Care Beds Intermediate Care in Community Respite Care Dental Care Substance Misuse Health Visitors Lymph oedema. Occupational Therapy School Nurses Diabetes care. Physiotherapy Audiology District Nursing Paediatric Occupational Therapy MacMillan/Palliative Care Sexual Health Children & Adolescent Mental Health Services Older People’s Mental Health Services (DMHOP) Recovery Services Community Stroke Team Falls Service Paediatric Physiotherapy Looked After Children Nurses Paediatricians Health Psychology Children’s Centre Continence Service Adult Health Visitor Adult Social Care Learning Disabilities Services Adult Social Care Health Community & Primary Care Mental Health Services Parkinson’s Podiatry Acquired Brain Injury Service Musculo-skeletal Service Multiple Sclerosis Service These services are supported by central functions including Training, Finance, Human Resources, Risk Management and Quality. 13 4 Patient Safety For 2009/10 the Provider Board agreed that there would be a certain number of indicators which would support their knowledge of the services and their performance. In respect of safety the following indicators were identified: 4.1 Key Safety Indicators Indicator Reduce Serious Untoward Incidents MRSA screening compliance MRSA bacteraemia rates Clostridium Difficile rates Source Local HCAI reduction plan HCAI reduction plan HCAI reduction plan Glossary: MRSA: Methicillin-resistant Staphylococcus aureus; a bacterium responsible for several difficult-to-treat infections in humans. HCAI: Healthcare acquired Infections. 4.2 Reducing Serious Untoward Incidents The National Patient Safety Agency (NPSA) report that: ‘Every day more than a million people are treated safely and successfully in the NHS. However, the advances in technology and knowledge in recent decades have created an immensely complex healthcare system. This complexity brings risks, and evidence shows that things will and do go wrong in the NHS; that patients are sometimes harmed no matter how dedicated and professional the staff.’ The Seven Steps are core to patient safety in healthcare organisations. The NPSA provide guide documents which provide a checklist to help staff to plan their activities and measure patient safety performance. The Steps are: 1 Build a safety culture 2 Lead and support your staff 3 Integrate your risk management activity 4 Promote reporting in primary care 5 Involve and communicate with patients and the public 6 Learn and share safety lessons 7 Implement solutions to prevent harm In Herefordshire PCT Provider Services we have set out to build a Safety Culture by encouraging reporting of incidents and supporting the recognition of lessons that can be learned from incidents and ensuring that lessons are shared and implemented to improve safety for all patients. Success Story Dental Therapist, Gilly Hunt, based at the Dental Access Centre at Gaol Street in Hereford has been named the British Association of Dental Therapist; Therapist of the year 2010. Gilly has been a hard working member of staff for many years and is an inspiration to the team. 14 PART 3 Chart to compare of the number of serious incidents reported over the last 2 years 8 7 6 5 2008-2009 4 2009-2010 3 2 1 m ar ch ja nu ar y fe br ua ry oc to be r no ve m be r de ce m be r au gu st se pt em be r ju ly ju ne m ay ap ril 0 Herefordshire PCT is below average in its level of reported incidents as recorded by the NPSA. During the last 12 months the total number of incident reports has remained similar (slightly more than 2000 incidents) across all directorates. The number of Serious Untoward Incidents was small 12 months ago but there has been a decrease in the number of these reported during the year (2008/09 = 34 2009/10 = 21). 4.3 Compliance with MRSA Screening Process Published in 2006 Essential Steps to safe, clean care1 translated existing guidance on infection control into a format that could be easily measured and applied. This process of self assessment has been used in Herefordshire across the Community Hospitals and inpatient intermediate care units to support the delivery of safe care for all patients. Assurance has been provided to the board through a monthly surveillance report. In order to contain infection and reduce the risk of cross infection of all patients it is necessary to screen certain categories of people for MRSA when they arrive at the Success Story Community Hospital or Intermediate Care Unit. Work of the Diabetes Nursing team has reduced Across the year there has been a noted hospital admissions for their improvement on the understanding of the patients by 50% usage of the tool and the application of it, and we have seen a steady and marked improvement in screening. When we have seen lower numbers we have investigated the 1 Essential steps to safe, clean care: reducing healthcare-associated infections 15 reasons in detail and put actions in place to improve compliance. MRSA Screening Compliance Sep-09 Ross CH - Merlin 100% Ross CH Peregrine 100% Leominster CH 43% Bromyard CH 64% Hillside Centre 86% Cantilupe ward 100% Jenny Lind Ward 100% Mortimer Ward 64% Podiatric Surgery 100% 4.4 Oct-09 100% Nov-09 100% Dec-09 100% Jan-10 100% Feb-10 100% Mar-10 100% 100% 74% 93% 89% 100% 100% 58% 100% 100% 73% 90% 96% 100% 100% 100% 100% 100% 40% 93% 100% 100% 100% 85% 100% 100% 94% 91% 96% 100% 100% 100% 100% 100% 96% 97% 96% 100% 100% 92% 63% 100% 100% 100% 100% 100% 100% 100% 90% MRSA Rates The MRSA data captures new diagnosis of MRSA infection and colonisation within the Trusts inpatient areas March 2010 compared against the previous 12 months figures. Over a number of years the Community Hospitals have been working with the Infection Control Team to reduce the levels of infection and to fully explore the origin of infections. Root Cause Analysis investigation is undertaken for every occurrence. The lessons learned from such investigation is shared with colleagues and new processes initiated if necessary. 2009/10 has seen the lowest number of MRSA incidents for the last 5 years. 16 PART 3 4.5 Clostridium Difficile (Cdiff) Rates The data below captures new diagnosis of Clostridium difficile infection within the Trusts inpatient areas March 2010 compared with the previous 12 months figures. C.Diff incidents are treated in the same way as for MRSA; all incidents are investigated and lessons learned shared. 2009/10 has seen the lowest number of incidents in the last five years. 5 Clinical Effectiveness/ Quality Measures Essence of Care undertaken for each National clinical Area Reduce Mixed Sex Accommodation Mixed Sex Accommodation reduction plan Compliance with NICE guidelines National Comply with CQUIN requirements Regional Service specifications written and Local quality and performance indicators / activity performance indicators metric agreed Improve data quality Data quality improvement plan Glossary: NICE National Institute for Clinical Excellence CQUIN: Commissioning for Quality and Innovation PIP: Productivity Improvement Programme 17 5.1 Essence of Care During the past 12 months nursing teams have been reviewing the Essence of Care2 benchmarks to determine if they have improved or changed the way they are working. Teams who have not previously taken part in the exercise have started to measure their service delivery using the benchmarks. In the first instance teams have looked at the benchmarks for ‘Privacy and Dignity’. All teams have now benchmarked their service against ‘Privacy and Dignity’. This has lead to changes being made to the way we do things to take account of the personal privacy and dignity of patients/ service users. 5.2 Success Story 105 Apprentice placements were offered in services around Herefordshire (60 more than last year). 65 have been offered advance placements for further training and learning next year 80% of Apprentices take up work in the care sector. Reducing Mixed Sex Accommodation Herefordshire Provider Services were able to declare their virtual compliance with the national target for single sex accommodation. During the past 12 months work has been undertaken to address the concerns about mixed sex accommodation. In the Mental Health inpatient area structural work has been undertaken, to provide single sex bathrooms and toilets. In Intermediate Care Facilities and Community Hospitals work has been undertaken related to the planned use of facilities to reduce the occasions where different genders have to share the same facilities. Where it has not been possible to ensure that people of one gender will not be walking through an area occupied by people of the opposite gender this has been limited to areas such as corridors. Toilets and bathrooms are clearly designated as being for one gender only. 5.3 PEAT (Patient Environment Action Team) PEAT is an annual assessment of inpatient healthcare sites in England with more than ten beds. The assessment was established in 2000 (managed by the NPSA since 2006) and is a benchmarking tool to ensure improvements are made in the non-clinical aspects of a patient’s healthcare experience. PEAT highlights areas for improvement and shares best practice across the NHS. The annual assessment took place in February. Amongst the assessors is a patient representative. All scores are supplied to the National Patient Safety Agency. 2 Essence of Care: Patient-focused benchmarks for clinical governance 18 PART 3 Site Leominster Bromyard Ross Hillside Stonebow Cleanliness/Envi ronment Good Good Good Good Good Food Good Excellent Good Excellent Good Privacy Dignity Good Good Good Good Good & All in patient facilities assessed early in 2010 in Herefordshire Provider Services were scored as ‘Good’ or ‘Excellent’. This included Community Hospitals and Inpatient Mental Health Services, and shows NHS Herefordshire’s commitment to improving its Estates and premises to improve cleanliness, environment, food and privacy and dignity. 5.4 Compliance with NICE Guidance The National Institute for Health and Clinical Excellence (NICE) provides guidance, sets quality standards and manages a national database to improve people’s health and prevent and treat ill health. Implementing NICE guidance benefits everyone - patients, carers, the public, the NHS. It helps ensure consistent improvements in people' s health and equal access to healthcare. During the period from April 1st 2009 and 31st March 2010, 65 pieces of guidance have been issued by the National Institute for Clinical Effectiveness. The guidance falls into 5 categories: • • • • • Cancer service guidance Clinical guidelines Interventional procedures Public health guidance Technology appraisals Of the guidance issued in the 12 months 16 documents have been determined as relevant to the services delivered in the organisation. All of these have been circulated to relevant clinical leaders. There are 12 documents where it was determined that we met the standard or for which we have taken steps to meet the standard. There have been matters within the guidance which have caused us to take steps to change what we are doing in order to come into line with the recognised standards. There are 3 documents where we still have steps to take to meet the standard. These are: Guidance name What we are doing Low back pain Vagus nerve stimulation for treatment-resistant depression Venous thromboembolism reducing the risk The guidance is currently being reviewed with the Musculoskeletal Service and the Integrated Commissioning team. All Provider Physiotherapy Services are compliant An action plan has been agreed, and is being implemented Assessments are currently being completed. 19 5.5 Comply with National Target for 18 Weeks from Referral to Treatment in Consultant Lead Services The 2004 NHS Improvement Plan set out the idea for reform: “By 2008, no one will have to wait longer than 18 weeks from GP referral to hospital treatment.” The 18 week referral to treatment (RTT) pathway is about improving patients’ experience of the NHS - ensuring all patients receive high quality elective care without any unnecessary delay. The 18 week maximum wait for an assessment applies to pathways that involve consultant-led care, setting a maximum time of 18 weeks from the point of initial referral up to the start of any treatment necessary for all patients where it is clinically appropriate and where patients want it. Across the year provider services were 100% compliant with this target. 5.6 Comply with CQUIN requirements The commissioners asked us to provide information as part of a regional project called PIP (Productivity Improvement Programme). We set up a plan to provide information and analyse this in line with the project. This has helped us all to understand the current services we provide, how we can improve efficiency and to be clear about what we are doing to support people in Herefordshire. We were able to reach each target at the appointed time. Achievements against targets in the productivity improvement plan: What we need to do/ Quarter 1 Quarter 2 Quarter 3 By when Receipt of recommendations and action plans for 09/10 Submission by provider of input file for benchmarking (BMT) (09/10) Submission by provider of input file for Service Line Economics (SLE) community model Sign-up by all providers to generic quality indicators to measure SLE tool Submission of quality indicators for population of SLE Time to Care diary card exercise completed for selected teams Receipt of evidence based report to identify measurable productivity improvement & service improvement Expected Achieved Expected Achieved Expected Achieved Quarter 4 Expected Achieved YES YES YES YES YES YES YES 5.7 Service Specifications Written and Quality and Performance Indicators / Activity Performance Indicators Metric Agreed All services have produced a document which describes the service which they deliver, who delivers it, where, and when. It also describes the patient/ service user group which it caters for. Targets for activity etc were agreed with the Integrated Commissioning team commissioners (people who pay for the service to be delivered) to decide if we 20 PART 3 were delivering the services to an appropriate standard. These targets have been monitored throughout the year, and we have been able to show we have met their targets. 5.8 Improve Data Quality The type and detail of information we collect has been improved over the past year, and staff training has addressed many of the issues we had. To do this we have had support from Information Technology project managers who have worked with us to tailor the data we collect and the systems we have in place. We have more work to do to be able to have up to date accurate information which is produced in a style which helps us to react more quickly to issues in services and the needs for change, however we have made considerable improvements in 2009/10. 6 Patient Experience During the last 12 months teams have asked patients/service users and carers for their opinions of the services they are receiving. In Community Hospitals there is a monthly survey of patient and carer opinions which is used to inform managers and staff of the ways in which they could improve the services they are delivering. Other services for instance Health Visitors, Podiatry and Podiatric Surgery have undertaken patient satisfaction surveys, and we have used this information to make changes to our services. 6.1 Mental Health Services Mental Health Services have set up the Mental Health Reference Group, a group of users and carers who work in partnership to lead change across services. 6.2 Sexual Health Services Sexual Health Services undertook a Department of Health Survey of local young people. This looked at many aspects of the service. Friendliness, Confidentiality, Listening by staff, advice and treatment all received over 75% of positive answers (service rated as GOOD or EXCELLENT). Areas where improvements can be made were car parking, magazines available in waiting room, embarrassment and waiting times. We have plans in place to Success Story redevelop the waiting room area at Gaol Street to make it more comfortable for patients, and NICE Guidance for Palliative we are reviewing our Sexual Health services to Care was assessed by our see if we create additional appointments. local specialist support team. 6.3 MacMillan Nurses MacMillan Nurses took part in a national survey (MORI poll). The survey showed that the team explained their work well, that people were happy with the support offered, the information provided was informative and Following this, the MacMillan services were extended in January 2010 to provide 24/7 expert advice and care all day every day. 21 helped people and their families and that most people found the team easy to speak to . 6.4 Recruiting Student Health Visitors and School Nurses This year we invited local school pupils to take part in the selection of people to take up places to train to become school nurses or Health Visitors. This proved very successful. Three people were chosen to be supported to start their studies in September. 6.5 Physiotherapy - Patient Reported Outcome Measures (PROMS) A Physiotherapy lead service for people suffering from back pain problems has introduced sufferers to Pilates as a way to manage their pain. Patients were asked to record their pain levels at the start of the course and also after the 6 week course. The results of this show that people find this type of exercise helpful and feel that it has decreased the level of pain they feel and improved their mobility. 6.6 Parkinson’s Nurses The team have supported the development of a pioneering project which has won accolades for its innovation and patient satisfaction. The project was originally conceived by local Parkinson’s patient Mike Canavan. The work has looked at whether group singing can provide effective voice therapy for people with Parkinson’s. The project has been declared a success by those who took part, as well as being put forward for a national award. 7 Services Review 7.1 Service Review by Care Quality Commission A recent review by the Care Quality Commission of the acute Mental Health Services identified Good Practice observed: The ‘Rights presentation’ was excellent in that it was regularly undertaken and the recording made clear the extent of the patient’s understanding and whether or not he had been provided with a rights information leaflet. The Commission also noted that the leaflet includes information about the Independent Mental Health Advocacy Service. There was evidence of discussion about consent alongside a detailed assessment of capacity at the beginning of the patient’s detention. The statutory consultees involved due to the treatment plan of ECT for a patient lacking mental capacity had provided extremely detailed accounts of their rationale for agreeing with the treatment plan. The patient was prone to falling and the ward had involved a physiotherapist to review his care, a falls diary had been developed as well as a falls risk assessment and risk management plan. 22 PART 3 Success Story The new Herefordshire Intermediate Care Team officially starts work on May 4th 2010 with a single point of access and equitable service for people across the whole County. The service is to be provided 24/7. 7.2 Delays in Discharge from Inpatient Care NHS Herefordshire Provider services have been working with its partners to improve the discharge of patients from Community Hospitals and Mental Health Services. Improvements have been made within the year, and the overall delayed discharges have reduced over 2009/10. However the issue is a challenging one both nationally and locally. Further work is underway to reduce the delays which result in people staying in hospital longer than their medical needs indicate is necessary. The development of a community based intermediate care team and work with our partners in care will help us to continue to reduce delays across Herefordshire. The data provided below provides an overall picture of delays within NHS Herefordshire Provider Services including Community Hospitals, Intermediate care and Mental Health, and those contracts for other In-Patient beds in the community commissioned by NHS Herefordshire (excluding Hereford Hospitals NHS Trust) Number of bed days lost due to delay in discharge: ! 7.3 " #"# $" $ % & & "' $ "' ( Management of Complaints During the year 52 letters of complaint were received by Herefordshire Provider Services, of these 76% were sent an acknowledgement within 3 days. We aim to acknowledge all letters within 3 days; however, complaint letters and phone calls are received at various places in the organisation. The rural nature of the area the organisation serves and therefore the distance between our staff bases sometimes leads to delays in receipt of the letters at a point where an acknowledgement can be sent and an investigation of the complaint can be started. 23 Acknowledgement of complaints following receipt in service 9 8 7 6 5 4 3 2 1 0 Apr-09 May09 Jun-09 Jul-09 Aug-09 Sep-09 Oct-09 Nov-09 Dec-09 Jan-10 Feb-10 Mar-10 Responses within 3 days Over 3 days We are looking at the way we are managing the process as well as ensuring our staff know what to do when they receive a complaint; giving due regard for maintaining the confidentiality of an individual’s information when we pass on the complaint to be dealt with. We are working closely with the NHS Herefordshire and Herefordshire County Council Customer Insight Unit to ensure a coordinated approach to complaints management and response times. 8. Service Improvements 8.1 Podiatric Surgery The department has developed into a sub-regional “Centre of Excellence”. The service undertakes 1000 operations and 5000 outpatient appointments per year. Podiatric Surgery has out of county contracts with neighbouring counties which account for about 50% of the department’s activity. Since the mid - 1990s services have been provided by the Podiatric Surgeons of Herefordshire to surrounding counties: Powys, Gloucestershire, Telford and Wrekin, South Shropshire and Worcestershire. The team accept patients from across the Country. 8.2 Community Hospitals and Intermediate Care Across our community inpatient service (Ross Hospital, Leominster Hospital, Bromyard Hospital and Hillside Intermediate Care) we have implemented the NHS Institute “Releasing More Time to Care”. It is a part of a series of ways in 24 PART 3 which the NHS has been changing services according to the LEAN processing. This is a Community Hospital improvement plan which looks at the way we manage and communicate in our Community Hospitals and looks at way that they can be simplified and streamlined. This programme of work means that nurses have more time to spend with patients and carers and the development of more systematised processes will improve patient care. The programme has already resulted in release of 21% trained nurse direct care time, (based on minute interval observations of an eight hour shift,) and we have seen improvements in patients satisfaction with services (see overleaf), which shows an increase in positive comments from patients about their experiences during their stay with us. 8.3 MacMillan Nurses Since January 2010, MacMillan Nurses are providing a 24/7 service in response to the End of Life Strategy (DOH, 2008) and the Supportive and Palliative Care Guidance for Adults with Cancer (NICE, 2004). Development of the service has ensured that one of the most vulnerable client groups within Herefordshire Health community and the health professional caring for them can now access specialist support at week ends and bank holidays. In the first twelve weeks of operation with one nurse on duty at week ends and bank holidays, the service was accessed on 218 occasions by patients or carers 25 Success Story Physiotherapists have been supported by Practice Based Commissioners to develop a 12 month pilot to provide services at rural surgeries. This will improve access for those who find it difficult to travel to the centres where services are already provided. 8.4 and 129 occasions by healthcare professionals. This new pattern of working by the Macmillan Community Palliative Care Service ensures support to health care professionals in providing care, and ensures that all patients in the palliative care phase of an illness receive valuable support and information at a time when they may be feeling very vulnerable. Community Intermediate Care Since June last year work has been underway to amalgamate the existing Community Intermediate Care teams from both Social Care and PCT into one new countywide service. This will provide a more comprehensive and coordinated team, whose remit is to support people to remain in their own homes via short term input from a multi-disciplinary team of staff. They work to both try and avoid people being admitted into hospital/residential care unnecessarily and to support a more timely discharge from inpatient facilities should someone be admitted. 8.5 Physiotherapy This year has seen the successful start of a new contract with the Rural GP Practices to provide surgery based physiotherapy giving much improved access to physiotherapy in rural areas. Patients are now able to Self-refer to surgery based Physiotherapists, giving better /quicker access to assessment and treatment plus a reduced need to take up GP appointment time. Choose and Book is now being offered for Physiotherapy services, enabling better access to the service, across the county. 8.6 Occupational Therapy Services The service has developed a new staff role of assistant therapist to support the increased demand for services (18% more people asking for support over the last 3 years). The Falls Support Service is providing ‘Stay Steady’ Groups across the county supporting improved independence for older people. 8.7 Intermediate Diabetes Service The Diabetes Specialist Nurses is part of a shift of focus from hospital to community care. In two years the service has improved access to specialist services for patients, carers and staff working in the community and provided a bridge between primary and secondary care providers, facilitating effective 26 PART 3 patient pathways and proven to be highly cost effective. In the first year referrals to hospital specialist services were reduced by 50%. 8.8 Acute Mental Health Services Refurbishment of Mortimer Ward, Jenny Lind Ward and ground floor public access areas has been completed this year at the Stonebow Unit. Service Users were consulted on aspects of the refurbishment and the work has made the environment much more welcoming for patients, carers, visitors and staff. Thanks go to NHS Herefordshire, the Strategic Health Authority and Charitable Trust funds who have all contributed to the costs of the redevelopment. 8.9 Apprenticeships Our services continue to support placements for local young people to gain experience of working whilst gaining nationally recognised qualifications and being paid an allowance for their studies. For many young people this offers a realist way into work, and helps young people into work, and boosts the local economy as well as providing well trained staff for local services. 8.10 Change Champions Last year, 100 colleagues in Herefordshire PCT and Council took the challenge through the Change Champions Transformation Programme 2009. Teams of Change Champions were each tasked with helping services to drive improvement in a key performance area. One area where the champions have been working is on the ‘flow’ of patients across services, helping to reduce the blockages in the system. They have looked across the services from patients arriving at the local acute hospital, through Success Story local Community Hospitals etc to the point where they are in their own homes being Podiatric Surgery Service supported by community services either recognised as a national health or social care. ‘Centre of Excellence’ by the Faculty of Surgery of The College of Podiatrists (the organisation which sets the standards for training and clinical practice for Podiatric Surgery in the United Kingdom) 27 8.11 What Others Say About Us: NHS Herefordshire’s (Commissioning Arm) Commentary on Herefordshire PCT Provider Services Quality Accounts High Quality Care for All, published in June 2008 set out the requirement for all providers of NHS services to publish Quality Accounts annual reports to the public on the quality of health care services they deliver. NHS Herefordshire is pleased to endorse Herefordshire PCT provider services first Quality account which provides information with regard to the quality of the services it provides to the public. Based on the knowledge NHS Herefordshire commissioners has of Herefordshire PCT provider services, we believe that this report is a fair reflection of the healthcare services provided. The report celebrates the successes and improvements in quality but is balanced in that it recognises those areas which require further development. NHS Herefordshire commissioners monitor the quality performance of PCT Provider services monthly through the Clinical Quality Review Forums. Performance data in relation to quality is presented and verified, and action plans supported to address areas of less than optimum performance. NHS Herefordshire supports the overall broad priority areas for quality improvements identified by PCT providers in these quality accounts and looks forward to the detailed action plans, which will identify the desired outcomes for patients, following these improvements in systems and processes Nicky Willett Associate Director of Nursing, Quality and Clinical Leadership NHS Herefordshire May 2010 28 PART 3 8.12 Herefordshire Council: Health Scrutiny Committee Commentary on Herefordshire PCT provider Services Quality Accounts 29