Intermediate and Long-Term Outcomes of Total Ankle Arthroplasty and Ankle Arthrodesis 1899
advertisement

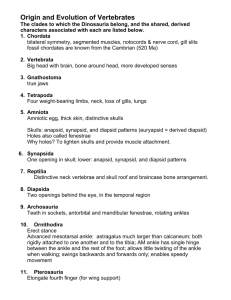
Haddad.fm Page 1899 Thursday, August 16, 2007 12:00 PM 1899 COPYRIGHT © 2007 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED Intermediate and Long-Term Outcomes of Total Ankle Arthroplasty and Ankle Arthrodesis A Systematic Review of the Literature By S.L. Haddad, MD, J.C. Coetzee, MD, R. Estok, RN, BSN, K. Fahrbach, PhD, D. Banel, BA, and L. Nalysnyk, MD, MPH Investigation performed at Illinois Bone and Joint Institute, Glenview, Illinois, and United BioSource Corporation, Medford, Massachusetts Background: The efficacy of total ankle replacement compared with that of ankle fusion continues to be one of the most debated topics in foot and ankle surgery. The purpose of this study was to determine whether there are sufficient objective cumulative data in the literature to compare the two procedures. A systematic review of the literature addressing the intermediate and long-term outcomes of interest in total ankle arthroplasty and ankle arthrodesis was performed. Methods: A comprehensive search of MEDLINE for all relevant articles published in English from January 1, 1990, to March 2005 was conducted. Additionally, relevant abstracts from the 2003 and 2004 annual proceedings of major orthopaedic meetings were eligible. Two reviewers evaluated each study to determine whether it was eligible for inclusion and collected the data of interest. Meta-analytic pooling of group results across studies was performed for the two procedures. The analysis of the outcomes focused on second-generation ankle implants. Results: The systematic review identified forty-nine primary studies, ten of which evaluated total ankle arthroplasty in a total of 852 patients and thirty-nine of which evaluated ankle arthrodesis in a total of 1262 patients. The mean AOFAS (American Orthopaedic Foot and Ankle Society) Ankle-Hindfoot Scale score was 78.2 points (95% confidence interval, 71.9 to 84.5) for the patients treated with total ankle arthroplasty and 75.6 points (95% confidence interval, 71.6 to 79.6) for those treated with arthrodesis. Meta-analytic mean results showed 38% of the patients treated with total ankle arthroplasty had an excellent result, 30.5% had a good result, 5.5% had a fair result, and 24% had a poor result. In the arthrodesis group, the corresponding values were 31%, 37%, 13%, and 13%. The five-year implant survival rate was 78% (95% confidence interval, 69.0% to 87.6%) and the ten-year survival rate was 77% (95% confidence interval, 63.3% to 90.8%). The revision rate following total ankle arthroplasty was 7% (95% confidence interval, 3.5% to 10.9%) with the primary reason for the revisions being loosening and/or subsidence (28%). The revision rate following ankle arthrodesis was 9% (95% confidence interval, 5.5% to 11.6%), with the main reason for the revisions being nonunion (65%). One percent of the patients who had undergone total ankle arthroplasty required a below-the-knee amputation compared with 5% in the ankle arthrodesis group. Conclusions: On the basis of these findings, the intermediate outcome of total ankle arthroplasty appears to be similar to that of ankle arthrodesis; however, data were sparse. Comparative studies are needed to strengthen this conclusion. Level of Evidence: Therapeutic Level IV. See Instructions to Authors for a complete description of levels of evidence. Disclosure: In support of their research for or preparation of this work, one or more of the authors received, in any one year, outside funding or grants in excess of $10,000 from DePuy Orthopaedics, a Johnson and Johnson Company. In addition, one or more of the authors or a member of his or her immediate family received, in any one year, payments or other benefits in excess of $10,000 or a commitment or agreement to provide such benefits from a commercial entity (DePuy Orthopaedics). No commercial entity paid or directed, or agreed to pay or direct, any benefits to any research fund, foundation, division, center, clinical practice, or other charitable or nonprofit organization with which the authors, or a member of their immediate families, are affiliated or associated. A video supplement related to the subject of this article has been developed by the American Academy of Orthopaedic Surgeons and JBJS and is available for viewing in the video library of the JBJS website, www.jbjs.org. To obtain a copy of the video, contact the AAOS at 800626-6726 or go to their website, www.aaos.org and click on Educational Resources Catalog. J Bone Joint Surg Am. 2007;89:1899-905 • doi:10.2106/JBJS.F.01149 Haddad.fm Page 1900 Thursday, August 16, 2007 12:00 PM 1900 THE JOURNAL OF BONE & JOINT SURGER Y · JBJS.ORG VO L U M E 89-A · N U M B E R 9 · S E P T E M B E R 2007 T he development of total ankle implants began in the 1970s as an alternative to ankle arthrodesis. Firstgeneration cemented total ankle implants, constrained and unconstrained, often failed, primarily as a result of poor implant design, loosening, and instability1,2. Despite these results, the search for a successful ankle prosthesis continued, leading to the development of a second generation of total ankle implants with numerous modifications, including a semiconstrained cementless design, and mobile and fixedbearing designs1,3,4. The relative benefits of total ankle arthroplasty and ankle fusion continue to be one of the most debated topics in foot and ankle surgery. Proponents for each procedure advocate their point of view very strongly, but most of the information is anecdotal and based on personal experience. The purpose of this study was to determine whether there are sufficient objective cumulative data in the literature to compare the two procedures. We performed a systematic review of the literature addressing the intermediate and long-term outcomes of total ankle arthroplasty and ankle arthrodesis in terms of ankle function, pain, revision, conversion to arthrodesis, implant survival, and quality of life. Materials and Methods tandard systematic review methods were used5,6. Initially, a prospective protocol was written to describe the objectives, search criteria, study selection criteria, data elements of interest, and plans for analysis. According to the protocol, a broad search of the English-language literature spanning fifteen years, from January 1, 1990, to March 24, 2005, was conducted. MEDLINE was searched through PubMed with use of the following search strategies: (1) “ankle replacement” OR “ankle prosthesis” or “ankle fusion”; (2) (arthroplasty, replacement [MeSH] AND “ankle”) OR (Arthrodesis [MeSH] AND “ankle”); (3) 1 OR 2. A manual reference check of all accepted papers and recent reviews was performed to supplement the electronic searches and to identify any additional potentially relevant studies. In addition to the published literature, abstracts from the 2003 and 2004 annual proceedings of the American Academy of Orthopaedic Surgeons (AAOS) and American Orthopaedic Foot and Ankle Society (AOFAS) meetings were searched for eligible studies. Eligibility requirements were the same for abstracts and full publications. For a study to satisfy the criteria for inclusion, the authors had to have reported on (1) total ankle arthroplasty or tibiotalar ankle arthrodesis surgery, (2) outcomes of interest at two years or more after the operation, and (3) at least ten patients in the treatment group. Studies in which all patients had been treated with only revision total ankle arthroplasty or revision arthrodesis were excluded. There were two reviewers, who had to agree on all accepted and rejected studies. All study designs were eligible, including randomized controlled trials, prospective and retrospective nonrandomized controlled trials, and uncontrolled case series. Multiple publica- S I N T E R M E D I A T E A N D L O N G -TE R M O U T C O M E S O F TO T A L A N K L E A R T H R O P L A S T Y A N D A N K L E A R T H R O D E S I S tions on the same patient population were pooled as one study (kinship) to the extent possible to avoid double-counting of patients. Protocol-defined data elements from each eligible study were extracted by one researcher onto a data-extraction form and were confirmed by a second researcher, who checked all extracted data against the original report. Differences were resolved prior to data entry. Statistical Methods Outcomes of interest included patient-reported outcome scores, mobility, function, pain, revision or conversion to an arthrodesis, implant survival, and prosthetic loosening. In addition, the overall postoperative outcome, based on the patient’s assessment, was recorded. Study, patient, and treatment characteristics were summarized with use of basic descriptive statistics. The number of patients enrolled (or randomized) was used as a denominator in the analysis of baseline patient characteristics in the assessment of patient-reported efficacy outcomes. The number of ankles evaluated was used as the denominator in the analyses of all other efficacy outcomes. Follow-up scores on the AOFAS Ankle-Hindfoot Scale and on other scales evaluating ankle pain, function, alignment, and range of motion were summarized for both total ankle arthroplasty and ankle arthrodesis. Similarly, overall patient outcomes were summarized with use of four categories: excellent, good, fair, and poor. The definitions of these four categories were for the most part uniform across studies. The AOFAS Scale (with excellent defined as 90 to 100 points; good, as 75 to 89 points; fair, as 50 to 74 points; and poor, as <50 points) was the most commonly used rating system in the studies of total ankle arthroplasties. The Mazur Score (with excellent defined as 80 to 90 points; good, as 70 to 79 points; fair, as 60 to 69 points; and poor, as <60 points) was most commonly used in the studies of arthrodeses. In order to include all available data, overall outcomes were also categorized as good (including excellent and good results) and poor (including fair and poor results). Data were summarized in two ways. First, raw means and counts were weighted by sample size and calculated for all outcomes. Second, selected efficacy outcomes were synthesized with random-effects meta-analytic pooling of group results across studies7,8. In random-effects meta-analyses, study results are weighted by a combination of study size and between-study variation. When there was no variation across study results that would not be expected due to random chance, the weighted results were equivalent to those found by weighting by study sample size. The presence of variation across study results suggests that important study-level factors were impacting results, causing large studies to be given somewhat less weight and, concomitantly, smaller studies to be given somewhat more weight. We report the efficacy results associated with second-generation implants, including the Agility and New Jersey LCS (DePuy, Warsaw Indiana), Buechel-Pappas (Endotec, South Orange, New Jersey), TNK (Kyocera, Kyoto, Japan), STAR (Waldemar Link, Hamburg, Germany), and Salto (Tornier, Montbonnot, France) prosthe- Haddad.fm Page 1901 Thursday, August 16, 2007 12:00 PM 1901 THE JOURNAL OF BONE & JOINT SURGER Y · JBJS.ORG VO L U M E 89-A · N U M B E R 9 · S E P T E M B E R 2007 ses. Similar efficacy outcomes were analyzed, with use of the same meta-analytic techniques, in the review of the ankle arthrodesis studies. No formal comparison of efficacy or safety outcomes between total ankle arthroplasty and ankle arthrodesis was performed. All calculations were performed with use of SAS software (version 8.1; Cary, North Carolina) and SPSS software (version 14.0; Chicago, Illinois). Results Studies he initial search yielded 460 citations, of which 167 were retrieved for further review. Sixty-two full publications and five meeting abstracts met all eligibility criteria for inclusion into the database (see Appendix). Eighteen of these were identified as kinship studies. The final database included forty-nine primary studies spanning the years 1990 to 2005. The studies included fifty-six treatment arms and 2114 patients. Study attrition is shown in Figure 1. The characteristics of the accepted studies are further detailed in Table I. T I N T E R M E D I A T E A N D L O N G -TE R M O U T C O M E S O F TO T A L A N K L E A R T H R O P L A S T Y A N D A N K L E A R T H R O D E S I S Of the forty-nine studies, ten (20%) focused on total ankle arthroplasty and thirty-nine (80%) described ankle arthrodesis; 852 patients underwent total ankle arthroplasty and 1262 underwent arthrodesis. The majority of the arthrodesis studies (56%) were published between 1990 and 1997, whereas all ten of the total ankle arthroplasty studies were published more recently, between 1998 and 2005. The vast majority of studies were from single centers in the United States and Europe. Other geographic locations included Japan and Taiwan. There were no studies directly comparing total ankle arthroplasty and arthrodesis. Three non-randomized controlled trials of ankle arthrodesis compared different surgical techniques for arthrodesis. The duration of follow-up ranged from two to nine years in the studies of total ankle arthroplasty and from two to twenty-three years in the studies of arthrodesis. The average follow-up time following the total ankle arthroplasties and the arthrodeses was approximately five years. All ten studies of total ankle arthroplasty (including a Fig. 1 Study attrition diagram. This algorithm outlines the filtration of studies from inception to conclusion of the project. Note the substantial number of studies that were rejected on the basis of rigid exclusion criteria. Haddad.fm Page 1902 Thursday, August 16, 2007 12:00 PM 1902 THE JOURNAL OF BONE & JOINT SURGER Y · JBJS.ORG VO L U M E 89-A · N U M B E R 9 · S E P T E M B E R 2007 I N T E R M E D I A T E A N D L O N G -TE R M O U T C O M E S O F TO T A L A N K L E A R T H R O P L A S T Y A N D A N K L E A R T H R O D E S I S TABLE I Study Characteristics Total Total Total Ankle Arthroplasty No. of Studies No. of Treatment Groups No. of Patients 49 56 2114 Ankle Arthrodesis No. of Studies No. of Treatment Groups No. of Patients No. of Studies No. of Treatment Groups No. of Patients 10 12 852 39 44 1262 Publication year 1990-1997 22 26 644 — — — 22 26 644 1998-2005 27 30 1470 10 12 852 17 18 618 Publication type Abstract Full paper 2 2 123 2 2 123 — — — 47 54 1991 8 10 729 39 44 1262 Geographic location North America 22 27 854 3 4 236 19 23 618 Europe 22 23 1073 6 7 590 16 16 483 Other* 5 6 187 1 1 26 4 5 161 44 50 1771 7 8 569 37 42 1202 5 6 343 3 4 283 2 2 60 42 48 1607 5 6 377 37 42 1230 7 8 507 5 6 475 2 2 32 3 6 121 — — — 3 6 121 46 50 1993 10 12 852 36 38 1141 5.32 (1.90-23.00)‡ 41 1192 Setting Single center Multicenter Study type Retrospective Prospective Study design Non-randomized controlled trial Uncontrolled study Implant manufacturer† DePuy Agility 1 1 126 DePuy LCS 1 1 38 Endotec Buechel-Pappas 2 2 72 Kyocera TNK 1 1 26 Waldemar Link STAR 4 5 394 Tornier Salto 1 1 96 Mixed (Wright/ Waldemar Link) 1 1 100 Cemented 1 1 26 Uncemented 6 7 654 4.70 (2.30-9.00)‡ 7 636 Implant fixation Follow-up time 5.10 (1.90-23.00)‡ 48 1828 *Other includes Japan and Taiwan. †Two implant types were reported in one study (Buechel et al., 2002). ‡The values are given as the mean and range in years. total of 852 patients) focused on second-generation total ankle implants. Information on the implants and the methods of fixation used in the total ankle arthroplasties is also displayed in Table I. Patients Patient characteristics were minimally described in the studies. In those in which the age of the patient population was reported, the mean overall age was fifty-three years (mean Haddad.fm Page 1903 Thursday, August 16, 2007 12:00 PM 1903 THE JOURNAL OF BONE & JOINT SURGER Y · JBJS.ORG VO L U M E 89-A · N U M B E R 9 · S E P T E M B E R 2007 I N T E R M E D I A T E A N D L O N G -TE R M O U T C O M E S O F TO T A L A N K L E A R T H R O P L A S T Y A N D A N K L E A R T H R O D E S I S TABLE II Efficacy Outcomes: Scores and Range of Motion Total Ankle Arthroplasty Outcome Measure No. of Treatment Groups No. of Patients Reporting Outcome Mean 5 243 80.6 points Ankle Arthrodesis Mean Meta-Analysis Mean (95% Confidence Interval) 136 75.15 points 75.6 (71.679.6) points No. of Treatment Groups No. of Patients Reporting Outcome 78.2 (71.984.5) points* 3 Meta-Analysis Mean (95% Confidence Interval) AOFAS Ankle-Hindfoot Scale score Total Pain 4 354 34.5 points — — — — — Function 4 354 37.4 points — — — — — Alignment 2 85 9.4 points — — — — — Kofoed score Pain 2 21 50.0 points — 1 28 32.5 points — Function 2 21 21.0 points — 1 28 15.7 points — Mazur score — — — — 4 86 73.0 points — Overall 5 296 26.75° — — — — — Plantar flexion 2 115 15.23° 12.8° (5.1°-20.5°)* 2 74 16.5° 16.8° (10.9°-22.7°)† Dorsiflexion 2 115 11.25° 9.9° (5.6°-14.2°)* 2 74 0.8° 0.1° (−7.9°-8.2°)* Range of motion *Significant heterogeneity (p < 0.01). †Significant heterogeneity (p < 0.10). range, eighteen to sixty-four years) (see Appendix). The patients treated with total ankle arthroplasty were older (mean age, fifty-eight years; mean range, forty-six to sixty-four years) than those treated with ankle arthrodesis (mean age, fifty years; mean range, eighteen to sixty-three years) and were predominately female (59%). The majority of the patients in the arthrodesis studies were male (52%). Rheumatoid arthritis was the primary indication for the total ankle arthroplasties (39%), whereas posttraumatic arthritis was the primary indication for the arthrodeses (57%). Efficacy Outcomes The reporting of efficacy outcomes was highly variable in both the total ankle arthroplasty and the ankle arthrodesis studies; therefore, the analyses performed in the present study were limited. The AOFAS Ankle-Hindfoot Scale total score and pain, function, and alignment subscores; the Kofoed scores for pain and function; and the range of motion (overall and plantar flexion-dorsiflexion) were among the most frequently reported evaluation methodologies. Table II presents both the raw means for these outcomes and the pooled meta-analytic results for the AOFAS total score and the range-of-motion outcomes for both total ankle arthroplasty and ankle arthrodesis. The meta-analysis mean AOFAS score was 78.2 points (95% confidence interval, 71.9 to 84.5) for the group treated with total ankle arthroplasty and 75.6 points (95% confidence interval, 71.6 to 79.6) for the group treated with ankle arthrodesis. The raw mean scores on the individual AOFAS subscales for pain, function, and alignment were 34.5, 37.4, and 9.4 points, respectively, in the group treated with total ankle arthroplasty. In the arthrodesis group, the raw mean Kofoed scores for pain and function were 32.5 and 15.7 points, respectively. Because of the lack of reporting of variances, meta-analysis of the subscale scores was not possible. In the studies of total ankle arthroplasty in which excellent, good, fair, and poor categories were used as overall outcome measures, the result was excellent in 38% of the patients (95% confidence interval, 0% to 96.8%), good in 30.5% (95% confidence interval, 21.0% to 39.9%), fair in 5.5% (95% confidence interval, 0% to 16.9%), and poor in 24% (95% confidence interval, 0% to 72.9%). In the arthrodesis group, the pooled outcomes were excellent in 31% (95% confidence interval, 19.8% to 41.5%), good in 37% (95% confidence interval, 26.4% to 47.3%), fair in 13% (95% confidence interval, 6.2% to 20.3%), and poor in 13% (95% confidence interval, 7.6% to 18.7%). The authors of several studies used different categorizations of overall patient outcomes (e.g., good-to-excellent results); therefore, in order to include these studies in the analysis, outcomes were combined into two wider categories: good (including both excellent and good results) and poor (including both fair and poor results). The meta-analysis of this binary outcome (Table III) showed that, in the studies of total ankle arthroplasty, 78% (95% confidence interval, 61.9% to 95.0%) of the patients had a good result and 22% (95% Haddad.fm Page 1904 Thursday, August 16, 2007 12:00 PM 1904 THE JOURNAL OF BONE & JOINT SURGER Y · JBJS.ORG VO L U M E 89-A · N U M B E R 9 · S E P T E M B E R 2007 I N T E R M E D I A T E A N D L O N G -TE R M O U T C O M E S O F TO T A L A N K L E A R T H R O P L A S T Y A N D A N K L E A R T H R O D E S I S TABLE III Efficacy Outcomes: Overall Postoperative Outcome Based on Patient Assessment Total Ankle Arthroplasty No. of Treatment Groups No. of Patients with Outcome/Total No. of Patients Reporting Outcome % of Patients Ankle Arthrodesis Meta-Analysis Mean (95% Confidence Interval) (%) No. of Treatment Groups No. of Patients with Outcome/Total No. of Patients Reporting Outcome % of Patients Meta-Analysis Mean (95% Confidence Interval) (%) Overall outcome Excellent 2 48/92 52.2 38.0 (0.0-96.8)* 17 177/508 34.8 30.7 (19.8-41.5)* Good 2 28/92 30.4 30.5 (21.0-39.9) 17 187/508 36.8 36.9 (26.4-47.3)* Fair 2 4/92 4.3 5.5 (0.0-16.9)† 17 72/508 14.2 13.3 (6.2-20.3)* Poor 2 12/92 13.0 24.0 (0.0-72.9)* 17 72/508 14.2 13.2 (7.6-18.7)* Overall outcome—binary Good (excellent and good) 6 388/482 80.5 78.4 (61.9-95.0)* 19 427/576 74.1 72.6 (61.2-84.1)* Poor (fair and poor) 6 94/482 19.5 21.8 (4.9-38.6)* 19 149/576 25.9 27.4 (16.0-38.8)* *Significant heterogeneity (p < 0.01). †Significant heterogeneity (p < 0.10). confidence interval, 4.9% to 38.6%) had a poor result. In the arthrodesis studies, 73% (95% confidence interval, 61.2% to 84.1%) had a good result and 27% (95% confidence interval, 16.0% to 38.8%) had a poor result. Data on implant survival, revisions, conversions to arthrodesis, and other clinical outcomes after the total ankle arthroplasties and ankle arthrodeses are presented in the Appendix. The five-year and ten-year implant survival rates following total ankle arthroplasty were 78% (95% confidence interval, 69.0% to 87.6%) and 77% (95% confidence interval, 63.3% to 90.8%), respectively. A revision during the follow-up period was required in 7% (95% confidence interval, 3.5% to 10.9%) of the patients who had undergone a total ankle arthroplasty. The most common reason for revision was loosening and/or subsidence (28%). Five percent (95% confidence interval, 2.0% to 7.8%) of the total ankle arthroplasties were converted to arthrodeses, with the main reason for conversion being loosening and/or subsidence (50% of all conversions). Below-the-knee amputation was performed in 1% of the patients treated with total ankle arthroplasty. Nonunion was observed in 10% (95% confidence interval, 7.4% to 12.1%) of the patients treated with ankle arthrodesis. Nine percent (95% confidence interval, 5.5% to 11.6%) of the arthrodesis group underwent revision, primarily because of nonunion (the indication for 65% of all revisions of arthrodeses). Five percent of the patients treated with ankle arthrodesis underwent a below-the-knee amputation. Significant heterogeneity was detected in almost all of these meta-analyses; therefore, the results must be interpreted with caution. Discussion o our knowledge, this is the first systematic review of the intermediate and long-term outcomes of total ankle arthroplasty and ankle arthrodesis. Baseline differences in the patient populations and the small number of studies contributing to each analysis do not permit formal comparison between the two surgical procedures. However, the intermediate and long-term outcomes analyzed in this review do suggest that total ankle arthroplasty is comparable with ankle arthrodesis. The strengths of this review include the clear definition of the research question to eliminate bias in the selection of the studies, adherence to an explicit research protocol that was developed prior to the analysis, the comprehensive nature of the literature search (with use of both electronic databases and manual bibliography searches), consensus between the two reviewers with regard to all data elements prior to entry into the database, and a quality-control review of all results. However, despite the strengths of the review process, they cannot overcome the inherent weaknesses in the literature. The primary limitation of this review is that a direct comparative meta-analysis of total ankle arthroplasty and arthrodesis was not possible because there were no head-to-head trials. We were only able to perform a pooled meta-analysis across all studies, with many studies being devoid of key data elements, including methodology reporting and baseline patient information. In addition, the variability of the reporting of outcomes of interest limited the number of studies for each meta-analysis. In fact, differences in patient populations, variability of surgical procedures, and differences in outcome T Haddad.fm Page 1905 Thursday, August 16, 2007 12:00 PM 1905 THE JOURNAL OF BONE & JOINT SURGER Y · JBJS.ORG VO L U M E 89-A · N U M B E R 9 · S E P T E M B E R 2007 evaluation tools and study follow-up times may all be partially responsible for heterogeneity among these studies. In future studies, it will be important to use uniform evaluation tools to make comparisons easier. This study exposed the major lack of objective, prospective, and controlled data on either procedure. The findings of this review demonstrate that the available data on the results of these procedures are based predominantly on retrospective uncontrolled case series from single institutions. The sample sizes in many of the studies were small. Therefore, prospective studies are needed to compare the two procedures in similar patient groups. Despite these limitations, this study provides evidence that both procedures yield satisfactory results, and the data suggest equivalence between the procedures, negating the poor connotations associated with ankle arthroplasty due to failures associated with first-generation implants. In fact, while all patients may not be candidates for ankle arthroplasty, it should be considered as a treatment option for those with ankle arthritis, with the clinician being allowed the latitude to determine appropriate indications. I N T E R M E D I A T E A N D L O N G -TE R M O U T C O M E S O F TO T A L A N K L E A R T H R O P L A S T Y A N D A N K L E A R T H R O D E S I S Appendix Tables presenting the patient characteristics and the clinical outcomes from the combined studies as well as a list of the studies that were evaluated are available with the electronic versions of this article, on our web site at jbjs.org (go to the article citation and click on “Supplementary Material”) and on our quarterly CD-ROM (call our subscription department, at 781-449-9780, to order the CD-ROM). S.L. Haddad, MD Illinois Bone and Joint Institute, Glenview Medical Arts Building, 2401 Ravine Way, 2nd Floor, Glenview, IL 60025. E-mail address: slhaddad@earthlink.net J.C. Coetzee, MD Orthopaedic Clinic, Riverside Campus, 1st Floor, R102, 2512 South 7th Street, Minneapolis, MN 55454 R. Estok, RN, BSN K. Fahrbach, PhD D. Banel, BA L. Nalysnyk, MD, MPH United BioSource Corporation, 101 Station Landing, Medford, MA 02155 References 1. Easley ME, Vertullo CJ, Urban WC, Nunley JA. Total ankle arthroplasty. J Am Acad Orthop Surg. 2002;10:157-67. 5. Cook DJ, Mulrow CD, Haynes RB. Systematic reviews: synthesis of best evidence for clinical decisions. Ann Intern Med. 1997;126:376-80. 2. Neufeld SK, Lee TH. Total ankle arthroplasty: indications, results, and biomechanical rationale. Am J Orthop. 2000;29:593-602. 6. Alderson P, Green S, Higgins JPT, editors. Cochrane Reviewers’ Handbook 4.2.1 [updated December 2003]. In: The Cochrane Library, Issue 1. Chichester, UK: John Wiley and Sons; 2004. 3. Cook RA, O’Malley MJ. Total ankle arthroplasty. Orthop Nurs. 2001; 20:30-7. 4. Pyevich MT, Saltzman CL, Callaghan JJ, Alvine FG. Total ankle arthroplasty: a unique design. Two to twelve-year follow-up. J Bone Joint Surg Am. 1998;80: 1410-20. 7. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177-88. 8. Hedges LV, Olkin I. Statistical methods for meta-analysis. Orlando, FL: Academic Press; 1985. p 230-57.