Training Mobility Tasks after Stroke with RESEARCH ARTICLE
advertisement

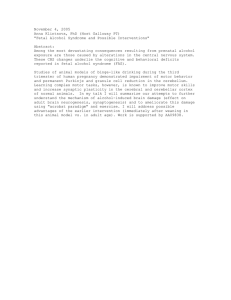
RESEARCH ARTICLE Training Mobility Tasks after Stroke with Combined Mental and Physical Practice: A Feasibility Study Francine Malouin, Carol L. Richards, Julien Doyon, Johanne Desrosiers, and Sylvie Belleville This study examines the potential of using mental practice (MP) to promote the learning of 2 mobility tasks in persons with stroke. Twelve patients were trained with MP to increase the loading of the affected limb while standing up from a chair and sitting down. Vertical forces were recorded using force plates under each foot and the chair. Changes in the loading of the affected limb and in task duration, immediately after 1 training session and 24 h later, served as outcomes. After training, the loading of the affected limb had increased (P < 0.001) during standing up (16.2%) and sitting down (17.9%), and the improvement remained significant 24 h later, indicating a learning effect. In contrast, the duration of the performance did not change with training. The results indicate that, in the early stage of learning with MP, changes in limb-loading strategies are a more sensitive measure of performance than is speed. Key Words: Standing up—Sitting down—Hemiparesis— Postural asymmetry—Motor imagery—Vertical ground reaction force T he use of mental practice in sports, through motor imagery, has gained much attention over the past decades as a means of promoting the learning of motor skills and to maintain performance when physical practice is not possible.1-3 Mental practice is defined as the act of From the Department of Rehabilitation, Laval University and Center for Interdisciplinary Research in Rehabilitation and Social Integration, Quebec City, PQ, Canada (FM, CLR); Department of Psychology, University of Montreal, PQ, Canada (JD, SB); and the Research Centre on Aging, Université de Sherbrooke, PQ, Canada (JD). Address correspondence and reprint requests to Dr. Francine Malouin, CIRRIS (Rehabilitation Research Center), IRDPQ, 525, Boul Hamel est, Quebec City, PQ, Canada G1M 2S8. E-mail: francine.malouin@rea.ulaval.ca. Malouin F, Richards CL, Doyon J, Desrosiers J, Belleville S. Training mobility tasks after stroke with combined mental and physical practice: a feasibility study. Neurorehabil Neural Repair 2004;18:66–75. DOI: 10.1177/0888439004266304 66 repeating, through motor imagery, an imagined movement several times with the intention of improving motor performance, whereas motor imagery corresponds to a dynamic state during which the representation of a specific action is internally reactivated within working memory without any overt motor output.4 Sport psychology literature has previously demonstrated that mental practice can improve the performance of motor skill behaviors.1-3 These studies have generally shown that subjects who practice only mentally a specific task usually display less improvement than those who practice physically, although mental practice leads to a superior increase in performance when compared to a no-practice condition.1 Different combinations of physical and mental practice, however, have been shown to be more efficient than either form of practice alone,5-7 with the effect of mental practice being greater when physical practice is added, even in small amounts.8 There is also some evidence that motor imagery performed using a 1st-person perspective (i.e., internally) yields better improvement than when performed in the 3rd-person perspective.9-11 Recent advances in the neurosciences have provided evidence that motor imagery activates brain regions similar to the areas activated during the physical execution of the same action.12-14 Using transcranial magnetic stimulation (TMS), PascualLeone and colleagues15 found that mental practice produced representational changes in the brain comparable to those yielded by physical practice. In addition, subjects who had been practicing mentally for 5 sessions reached the same level of performance as those who practiced physically for 5 sessions, after adding only 1 session of physical practice. This suggests that part of the behavioral improvement seen with mental practice may be latent, waiting to be expressed after minimal physical practice, hence supporting the combination of Copyright © 2004 The American Society of Neurorehabilitation Mental Practice and Mobility after Stroke mental and physical practice.15 Several investigators have proposed the use of mental practice in physical rehabilitation as a cost-efficient means of promoting motor recovery after damage to the central nervous system.16-20 However, the few studies21-24 that have investigated the use of mental practice in neurorehabilitation have focused on the training of the upper extremity, using mostly case study design.21,23,24 Results from these studies, however, are generally encouraging and suggest that mental practice can be used with good results for training the upper extremity after stroke. To our knowledge, the effects of mental practice to promote the learning of motor skills involving the lower extremities have not been studied in persons with stroke. Moreover, it is questionable if results obtained for unilateral manual tasks are applicable to locomotor-related tasks of the lower extremity, such as standing up and sitting down, that require coordinated actions of the trunk and both lower extremities. When compared to healthy subjects rising from a chair, persons with stroke take 25% to 61% longer, put much more load on the unaffected leg, and decrease the loading on the affected leg by 20% to 25%.25-27 Similar impairments of loading have been observed with sitting down.25,26 The relearning of motor strategies to obtain a more symmetrical loading on the lower limbs during these 2 mobility tasks early after stroke is critical to prevent compensations.28 The amount of physical practice a person early after stroke can manage, however, is reduced because of weakness, lack of endurance, and poor balance, hence limiting the practice time. Given the difficulty that each of these mobility tasks presents for persons after stroke, the addition of mental practice is a means of increasing the practice time without the physical constraints and fatigue associated with physical training. The main purpose of the present study was to examine the feasibility of using mental practice in combination with a small amount of physical practice to improve the motor strategy of persons with impaired loading of the affected leg while standing up from a chair and sitting down. The specific objectives were to (1) describe the deficits specific to partial loading (PL) and full loading (FL) phases of each task, (2) examine the response of a biomechanical limb-loading measure to change in motor strategies immediately after 1 training session, and (3) assess whether the changes in motor strategies were retained 1 day later (learning). Neurorehabilitation and Neural Repair 18(2); 2004 Table 1. Subject Characteristics Patients (n = 12)Healthy (n = 6) Gender (male/female) 10/2 Age (years) 56.1 (9.1) Mass (kg) 86.9 (12.8) Height (cm) 174 (6.0) Kinesthetic and Visual Imagery Questionnaire (max score = 50) Visual 38.1 (7.8) Kinesthetic 30.8 (8.9) Onseta (mo)a 20.3 (17.5) Sideb (left/right)b 6/6 ChedokeSASc (1-7)c Leg 6 Foot 5 Timed Up and Go (s) 16.5 (11.2) 5/1 50.2 (14.1) 71.4 (12.6) 170 (9) 36.9 (9.3) 35.0 (8.4) Values are presented as Mean (SD) unless otherwise indicated. a. Stroke onset to study entry. b. Side of the hemiparesis. c. Median score of the Chedoke-McMaster Stroke Assessment Scale. METHODS Subjects and Design Twelve persons with residual motor impairment on 1 side of the body (hemiparesis) resulting from a 1st cerebral vascular accident (patients) and a group of 6 age-matched healthy subjects participated in the study (Table 1). The patients included in the study were between 30 and 75 years old, had a unilateral locomotor disability consecutive to a stroke (ischemic or hemorrhagic origin), demonstrated motor imagery ability, and were able to stand up and sit down from a chair without using their arms. The exclusion criteria were cerebellar or brain stem lesions, receptive aphasia, moderate to severe body hemineglect, or other problems apt to interfere with the rehabilitation process or the motor tasks being trained (e.g., hip replacement, ankle sprain). The loading of the affected leg during standing up and sitting down was assessed at 3 time points: before training (baseline), after 1 training session (post-training), and 1 day later (followup). The motor imagery ability was also assessed at baseline. Motor imagery ability and limb loading were also assessed in the group of healthy subjects for comparison purposes. Since the healthy subjects demonstrated almost a 50% body weight distribution, they were not trained, but the values of 67 F. Malouin et al. selves perform the movements from within. The subjects rated their capacity to elicit mental images of the action on two 5-point scales (5 = high imagery, 1 = low imagery). One scale rates the clarity of the image (visual score), and the other rates the intensity at which they can feel themselves executing the movement (kinesthetic score). The Timed Up and Go32 (TUG) and the Chedoke-McMaster Stroke Assessment Scale33 were used respectively as measures of motor disability and motor impairment. The TUG is a mobility test that includes a series of tasks: standing up from a chair, walking 3 m, turning around and walking back to the chair, and turning around and sitting down. The Chedoke-McMaster Stroke Assessment Scale assesses the level of motor recovery on a 7stage scale ranging from 1 to 7 (stage 1 = lowest level). More specifically, it assesses the ability to perform dissociated movements and was used to assess motor impairment of the foot and the leg. Evaluation of Standing up and Sitting Down Tasks Figure 1. Experimental setup illustrating the position of the subject during testing. The chair and each foot were placed on 3 force plates (A, B, C). the leg with less loading were used to calculate the loading deficits of the affected leg of the patients. Clinical Evaluations A prerequisite for mental practice is the ability to engage in motor imagery. Therefore, at baseline, the Kinesthetic and Visual Imagery Questionnaire (KVIQ), which includes a series of 10 gestures scored on a 5-level ordinal scale,29 was used to evaluate motor imagery ability. This questionnaire, a modified version of the Movement Imagery Questionnaire (MIQ),30 has been validated (Cronbach’s α = 0.92), and its concurrent validity (with the MIQ: r = 0.61) in a group of healthy subjects has been reported.31 In this test, the participants were required to execute each movement physically and to immediately imagine the same movement as if they were seeing and feeling them- 68 Subjects were seated on a chair with a seat height standardized to 100% of lower leg length (Figure 1), and the chair and each foot were placed on 3 force plates.29 On hearing an auditory cue, the subjects were required to stand without using their hands and to sit down on a 2nd auditory cue. They were instructed to hold their paretic hand with their sound hand and to keep their elbows flexed in front of them. Five trials were recorded at baseline, immediately after the training session, and 24 h later. Signals from the force plates were collected synchronously at a sampling rate of 1000 Hz and recorded for further analysis. Training Procedures Prior to training, patients followed a familiarization procedure. In the familiarization period, the subjects were provided with visual feedback of their motor performance. This feedback, displayed on a monitor located in front of them, was the net vertical force trace indicating overloading on the affected (green trace) or the unaffected (red trace) leg when standing up and sitting down. Patients were instructed to modify their motor strategies to increase the loading of the affected leg (green Neurorehabilitation and Neural Repair 18(2); 2004 Mental Practice and Mobility after Stroke trace). Most important, they were asked to relate their movements to the outcome viewed on the screen and to remember the feeling and the movement sequences associated with success or error, to develop an inner representation of their performance. They were also instructed to verbally describe (explicit knowledge) what they did to improve their performance (e.g., “shift my body to the right and then move forward and up”) so that they could reactivate these pointers later during mental practice.20,29 The visual display was then removed, and the patients had to rely on their memory to repeat and rehearse mentally the proper motor strategies. The familiarization period ended after about 10 min, when the patients were able to provide a good autoestimation of their performance (whether they were able to increase the loading on the affected leg) as judged by the physical therapist who continued to monitor the limb loading on the visual display. The visual display was then taken away and not used any further for training. The familiarization period was followed by the training period, which consisted of a series of 7 blocks, each including 1 physical repetition (PP) and 5 mental repetitions (1PP:5MP training ratio). The 1PP:5MP ratio was based on preliminary findings in patients with stroke. It was found that 1 physical repetition after 5 mental repetitions provided the necessary feedback to go on with mental practice and be successful in imagining the task. During physical practice, the patients were instructed to stand up and sit down to an auditory cue as they had done during the baseline testing. Then they were instructed to close their eyes and to imagine they were standing up and sitting down and to verbally signal the beginning and end of each repetition. To control for mental practice, the therapist recorded the duration of the physical and the mental repetitions that are expected to have a similar duration.20 The training period required 25 to 30 min. DATA REDUCTION AND STATISTICAL ANALYSES The total scores from each scale of the motor imagery questionnaire (KVIQ) were averaged for each group. Each task was divided into a PL phase and an FL phase (see Figure 2) using the signals from the force plate under the chair. The PL phase is defined as the period when body weight is supported by the chair and both feet, whereas the FL phase represents the period without contact with Neurorehabilitation and Neural Repair 18(2); 2004 Figure 2. (A) Top graphs illustrate the mean vertical force exerted with each lower limb (right and left) when standing up and sitting down in the group of healthy subjects. The vertical forces are normalized in percentage of total body weight, and tasks are normalized in percentage of total duration. The vertical broken lines on the xaxis indicate the time of seat-off and separate the PL phase from the FL phase. Each task starts at time 0. (B) The middle graph represents corresponding patterns of vertical forces exerted by the affected and unaffected legs in the group of subjects with stroke. Note the large interlimb difference, with greater force exerted by the unaffected leg. Each task starts at time 0. (C) The lower graphs represent the changes in vertical force loading patterns after the training (open squares) and at followup (filled circles). Each task starts at time 0. the chair. Standing up started with the PL phase and sitting down with the FL phase (Figure 2). The onset of the standing-up task was determined by a change (10 N or more) in the vertical force signal 69 F. Malouin et al. Table 2. Mean (SD) Limb Loading (%) and Deficit (%) of the Affected Leg Standing Up Phase Patients with stroke (n = 12) Baseline Limb loading Deficit Post-training Limb loading Deficit Follow-up Limb loading Deficit Healthy subjects (n = 6) Limb loading PL FL Sitting Down Total PL FL Total 43.6 (4.8) 12.1 (9.7) 40.5 (7.9) 16.3 (16.4) — 14.2 (12.0) 45.1 (4.2) 7.8a (8.5) 41.3 (7.2) 15.3 (14.8) — 11.6 (10.4) 47.0b (5.5) 5.2 (11.2) 46.1b (5.2) 4.7 (10.8) — 4.9 (10.5) 48.8b (3.8) 0.2 (7.8) 46.9b (5.6) 3.4 (11.4) — 2.0 (8.7) 46.5b (6.8) 6.3 (13.6) 44.8b (6.7) 7.5 (13.8) — 6.9 (13.0) 48.1b (4.5) 1.7 (9.3) 45.1b (5.3) 7.5 (10.8) — 4.6 (9.5) 49.6 (1.0) 48.4 (2.3) — 49 (2.9) 48.8 (2.6) — PL, partial loading phase; FL, full loading phase; total, mean of PL and FL. a. Baseline deficits: deficit in PL phase was smaller (P < 0.03) than in FL for the sitting-down task, smaller than in PL phase of the standing-up task (P < 0.01). b. Training effects: significant increase post-training (P < 0.01) and at follow-up (P < 0.01). Table 3. Mean (SD) Duration (s) and Deficit (%) Standing Up Phase Patients with stroke (n = 12) Baseline Time Deficit Post-training Time Deficit Follow-up Time Deficit Healthy subjects (n = 6) Time PL FL Sitting Down Total PL FL Total 0.54 (0.32)a 60.9 (97.1) 1.41 (0.53) 1.95 (0.76) 59.5 (59.9) 59.9 (62.5) 0.81 (0.27) 47.7 (49.9) 1.52 (0.65) 60.1 (68.8) 2.33 (0.78) 55.5 (52) 0.62 (0.33) — 1.34 (0.43) 1.96 (0.71) — 60.7 (58.5) 0.72 (0.17) — 2.02 (0.18) — 2.74 (0.18) 82.7 (120) 0.56 (0.32) — 1.27 (0.39) 1.83 (0.61) — 50.4 (49.7) 0.79 (0.14) — 1.72 (0.10) — 2.49 (0.11) 66.1 (71) 0.33 (0.27) 0.89 (0.07) 0.55 (0.11) 0.95 (0.11) 1.5 (0.16) 1.2 (0.07) PL, partial loading phase; FL, full loading phase; total, mean of PL and FL. a. All duration values were significantly larger (Mann-Whitney U test; P < 0.001) than values from the comparison group. recorded from the force plate under the chair and the end of the task to full body elevation as determined visually by an observer29,34 who interrupted the recording. The sitting-down task started with the auditory cue and ended when the signals from the force plate under the chair were stable. The duration of each task was normalized to 100%, and the vertical ground reaction force (vertical impulse) from each leg was converted into percentage of body weight. For each task, a mean vertical force value (area under the curve) was calculated from 5 trials. The effects of training on limb loading and task duration were statistically examined using a 3factor ANOVA with repeated measures (time = 3 levels, tasks; 2 levels and phases 2 levels), followed by the post hoc Tukey procedure. The deficit levels of limb loading in the patients were calculated using mean loading values from the healthy sub- 70 jects. For each phase of each task, the percentage change from baseline values in loading of the affected leg and task duration were computed after training and at follow-up and expressed as a measure of improvement. Pearson correlation coefficients were used to determine whether the amount of improvement of limb loading was associated with the initial limb-loading deficit. Last, betweenand within-group comparisons (KVIQ, loading deficits and gains) were made using, respectively, the Mann-Whitney U test and the Wilcoxon rank sum test. RESULTS The subject characteristics are reported in Table 1. The mean age of the subjects in the 2 groups Neurorehabilitation and Neural Repair 18(2); 2004 Mental Practice and Mobility after Stroke Standing up 60 Partial loading phase Table 4. Relationships between Limb Loading Deficits at Baseline Full loading phase Sitting Down (FL) Limb loading gains (%) 50 Condition 40 Standing up (FL) Standing up (PL) Sitting down (FL) 30 20 10 r P Sitting Down (PL) r Standing Up (PL) P r 0.92 <0.0001 0.60 <0.04 P 0.68 <0.01 0.64 <0.03 0.90 <0.0001 1 1 0.58 <0.05 0.64 <0.03 PL, partial loading phase; FL, full loading phase. 0 Post-T F-Up Post-T F-Up Table 5. Between-Task Relationships of Limb Loading Improvement after Training and at Follow-up Sitting down 60 Partial loading phase Post Training Full loading phase Limb loading gains (%) Condition r P Follow-up r P 50 Full loading phase 0.96 Partial loading phase 0.45 40 <0.0001 NS 0.91 0.64 <0.0001 <0.03 NS, not significant. 30 20 10 0 Post-T F-Up Post-T F-Up Figure 3. Bar graphs representing mean (±1 SD) percentage improvement in the loading of the affected leg when standing up (top) and sitting down (bottom), posttraining (Post-T) and at follow-up (F-Up). was not different (Mann-Whitney U test; P > 0.05). Similar mean KVIQ scores were found for both groups (Mann-Whitney U test; P > 0.05), indicating that the patients had a motor imagery ability that compared to control subjects. Further comparisons, however, indicated that the patients had higher visual than kinesthetic scores (Wilcoxon rank sum test: P < 0.05). Impaired Performance: Limb Loading and Task Duration The patterns of limb loading illustrated in Figures 2A and 2B indicate that the difference in loading between legs was greater in the patients (Figure 2A, 2B). The mean loading, expressed as a percentage of body weight, is reported for each phase of both tasks for the 2 groups in Table 2. Data from the control group were used to calculate Neurorehabilitation and Neural Repair 18(2); 2004 the deficits reported in Table 2. For the standing-up task, there was no difference in the amount of loading deficit between phases, but for the sittingdown task, the loading deficit was smaller in the PL phase compared to the FL phase (Wilcoxon rank sum test: P < 0.03). Although there was no difference between tasks in the loading deficit in the FL phase, a smaller deficit was found in the PL phase of the sitting-down task (Wilcoxon rank sum test: P < 0.01). At baseline, the duration of both tasks was longer in the patients who took on average 60% and 55.5% more time than healthy subjects to stand up and sit down, respectively (Table 3). All duration values were significantly larger (Mann-Whitney U test; P < 0.001) than values from the comparison group. The duration of the PL phase represented 27% of the standing-up task compared to 35% for the sitting-down task, and these proportions were similar for the 2 groups of subjects. Effects of Training on Limb Loading and Task Duration After the training session, the patients increased the loading on the affected leg (Figure 2C) for both tasks, resulting in a smaller difference in the amount of loading exerted by each leg as compared to baseline (Figure 2B). As reported in Table 2, the loading deficits dropped markedly post-train71 F. Malouin et al. ing and at follow-up. Comparisons of loading values over time for both tasks (ANOVA) revealed an effect for time (F = 15.6, P < 0.001) and phase (F = 5.9, P < 0.03) but not for task and no interaction, indicating a similar improvement for both tasks and phases. A post hoc Tukey test carried out to determine whether the improvement was maintained over time indicated significant increases in loading (P < 0.01) post-training and at follow-up. The percentage gains in the loading of the affected leg are illustrated in Figure 3. Gains in the FL phase ranged from 11.3% to 18% and from 6.3% to 8.5% in the PL phase; there was no difference between tasks or phases (Wilcoxon rank sum test: P > 0.05). The task duration at baseline, post-training, and followup are reported in Table 3. Comparisons of task duration over time for both tasks (ANOVA) did not reveal a main effect for time and no interaction between time, task, or phase, indicating no significant change of duration with training. Relationship between Tasks in the Loading Deficit and Training Effect At baseline, high correlation coefficients were found (Pearson coefficient: r > 0.90) in loading deficits between similar phases of the mobility tasks but not between phases of the same task (Table 4). High Pearson correlation coefficients were also found in the magnitude of the loading improvement post training and at follow-up between tasks for the FL phase but not for the PL phase (Table 5). DISCUSSION A single training session of mental practice combined with physical practice resulted in an improvement of the motor strategies as determined by the loading patterns when standing up and sitting down. In addition, the improvement was retained 1 day later, indicating a learning effect. In contrast, training did not improve the speed of the performance. Effects of Training on Limb Loading and Task Duration The gains in loading obtained after a single 30min training period that included 7 physical repeti- 72 tions and 35 mental repetitions in the present study were similar to the magnitude of changes reported by Engardt and colleagues26 in patients after 3 weeks of regular training in a physiotherapy program. Thus, even if our patients physically executed the tasks 5 to 8 times during the familiarization period, the learning took place with a relatively small amount of physical practice. The reason for improvement with such little physical practice is possibly the combination with mental practice that required rehearsing mentally and explicitly the sequence of movements associated with each task. Such rehearsal made them focus each time on the preparation and planning of the proper strategy, hence increasing their awareness of the required movements. Present findings are in line with the results of Pascual-Leone and colleagues15 who demonstrated with TMS that mental practice had preparatory effects and increased the efficiency of subsequent physical training. Likewise, using positron emission tomography, Jackson and colleagues35 found that after 5 days of intensive mental practice, the changes in brain activity were not found in motor-related areas but were restricted to the medial aspect of the orbitofrontal cortex, supporting the idea that mental practice initially improves performance by acting on motor preparation and planning. At variance with previous studies,21-24 patients engaged in mental practice using a 1st-person perspective instead of a 3rd-person perspective. Moreover, rather than using audiotaped instructions that described scripts of functional activities to be imagined with the affected limb, patients were required to generate their own mental representation of the motor tasks. The latter training conditions may have contributed to optimizing the effects of motor imagery since the 1st-person perspective has been reported to be best to elicit kinesthetic components of a movement during imagery.9-11 Moreover, recent findings in the neurosciences have shown that only the 1st-person perspective activates regions that partly overlap with actual execution of motor behavior.36 Likewise, using internal signals for motor imagery eliminates the shortcomings associated with the use of audiotapes, which makes motor imagery a more passive process in which the patient is dependent on an external source to engage in motor imagery.7,20,37 Present results also indicate that initially, the improvement of the motor strategies is not necessarily associated with a faster execution, and our findings suggest a change in the quality of movement (improved loading of the affected leg) to be Neurorehabilitation and Neural Repair 18(2); 2004 Mental Practice and Mobility after Stroke the first indicator of learning. The latter may be related to the fact that in the early stage of learning, the subjects rely more on declarative knowledge of the tasks (conscious level), and such a cognitive process requires more attention and time.20 The other factor that may explain the lack of change in movement speed is likely of peripheral origin as it takes more training over a longer period to increase muscle strength and improve balance associated with faster movements. In fact, changes in both motor strategies and speed of movement have been documented after several weeks of training.26,38,39 Last, a faster performance may not necessarily reflect improvement in the quality of movement. On the contrary, it was found in a follow-up study40 that although gains in loading of the affected leg were lost, movement time in rising and sitting down had further improved. Latter findings suggest caution in the interpretation of changes related to spatiotemporal parameters, as a faster performance could be the result of more use of the unaffected leg or from other compensatory means.40 Finding that initial improvement in quality of movement without concomitant gain in speed in the initial phase of learning is also in keeping with the construct of the Motor Assessment Scale,41 which is based on the premise that improvement of motor performance precedes the increase in speed. Indeed, in this 7-level ordinal scale, the indicators for the lower levels of performance of the sit-tostand task are related to the symmetry of weight bearing, whereas the higher levels correspond to indicators of movement speed. Impaired Motor Performance after Stroke: Limb Loading and Task Duration The deficits measured while patients were bearing full weight were similar for both tasks, suggesting that both require as much training. Our findings concur with those of Engardt and Olsson25 who also observed, in a group of 42 patients with stroke, equivalent deficits in weight-bearing distribution for similar mobility tasks. The dividing up of the tasks into 2 phases, however, allowed us to demonstrate that deficits were present even when patients were not bearing full weight (PL phase) and that patients need to be reminded to sit with weight equally distributed before standing up. Our results also show that the deficits were smaller in the PL phase during sitting down compared to that during the standing-up task (Table 2), which fur- Neurorehabilitation and Neural Repair 18(2); 2004 ther emphasizes the difficulty in the transition from sitting to standing. When examining the nature of the deficits in loading, greater deficits occurred in the FL phases than in the PL phases, suggesting a phase-specific difference in motor strategies. This was confirmed by the correlation analysis (Table 4), which shows a strong intraphase relationship and a weaker interphase relationship. These findings are likely related to the nature of the control of the body momentum within each phase.42,43 For instance, the PL phase corresponds with the control of horizontal body momentum either in the forward direction for standing up or in the backward direction for sitting down.42,43 Likewise, the vertical body momentum has to be controlled in the FL phase by the extensor muscles of the lower limbs either by concentric contractions when standing up or eccentric contractions when sitting down.42 As for the correlation coefficients in Table 5, they revealed a strong relationship for the FL phase and a weaker one for the PL phase, suggesting the response to training across tasks is less consistent for the PL phase. IMPLICATIONS The present study has described a training approach to promote the learning of mobility tasks with mental practice. The 1PP:5MP training ratio method wherein mental practice is combined with a minimal amount of physical practice resulted in an increase of loading on the affected leg that was retained at follow-up. Although the study included a small number of subjects and did not tease out the additive effects of mental practice, this study described an innovative approach in using mental practice to augment physical practice to promote the learning of mobility tasks after stroke. The information relative to training methods and outcome measures gathered in this preliminary study has been applied to the design of the randomized trial that is now underway to evaluate the potential of mental practice for promoting the relearning of mobility tasks in a larger group of patients with stroke. Future studies are needed to compare the effects of different training programs combining physical and mental practice and to determine the optimal timing for the introduction of such training over the rehabilitation period. For example, in a recent case study,44 it was shown that the addition of mental practice in a patient who had reached a plateau after being trained only physically yielded an extra 73 F. Malouin et al. 10.3% improvement, and continuing his training with mental practice alone after discharge induced another small increase of 2.2%. This example illustrates how mental practice can gradually be introduced in a patient’s rehabilitation program. In general, once the patient has a good representation of the movements to be rehearsed, mental practice could be added to regular interventions. Thus, on discharge, the patient, already familiar with the method, should be able to continue training with mental practice on his or her own, hence further optimizing physical performance of the task. ACKNOWLEDGMENTS We thank the subjects who participated in this study. We also extend our gratitude to Lise Dion for her assistance in data collection and Daniel Tardif for preparing the figures. This work was supported by a grant from the Quebec Rehabilitation Research Network (REPAR) from the Fonds de la Recherche en Santé du Québec. C. L. Richards holds a Canada Research Chair in Rehabilitation. REFERENCES 1. Feltz DL, Landers DM. The effects of mental practice on motor skill learning and performance: a meta-analysis. J Sport Psychol 1983;5:25-57. 2. Hinshaw KE. The effects of mental practice on motor skill performance: critical evaluation and meta-analysis. Imagin Cogn Personality 1991;11:3-35. 3. Driskell JE, Copper C, Moran A. Does mental practice enhance performance? J Appl Psychol 1994;79:481-92. 4. Decety J, Grèzes J. Neural mechanisms subserving the perception of human actions. Trends Cogn Sci 1999;3:172-8. 5. McBride ER, Rothstein AL. Mental and physical practice and the learning and retention of open and closed skills. Percept Mot Skills 1979;49:359-65. 6. Richardson A. Mental practice: a review and discussion. Res Q 1967;38:95-107. 7. Hall C, Buckolz E, Fishburne GJ. Imagery and the acquisition of motor skills. Can J Sport Sci 1992;17:19-27. 8. Janssen JJ, Sheikh AA. Enhancing athletic performance through imagery: an overview. In: Sheikh AA, Korn ER, eds. Imagery in sports and physical performance. Amityville, NY: Baywood; 1994. p. 1-22. 9. Mahoney MJ, Avener M. Psychology of the elite athlete: an exploratory study. Cognit Ther Res 1977;1:135-41. 10. Ryan ED, Simons J. Efficacy of mental imagery in enhancing mental rehearsal of motor skills. Int J Sport Psychol 1982;4:41-51. 11. Rotella RJ, Gansneder B, Ojala D, Billing J. Cognitions and coping strategies of elite skiers: an exploratory study of young developing athletes. Int J Sport Psychol 1980;2:3504. 12. Stephan KM, Fink GR, Passingham RE, et al. Functional anatomy of the mental representation of upper extremity movements in healthy subjects. J Neurophysiol 1995;73:37386. 74 13. Deiber MP, Ibanez V, Honda M, Sadato N, Raman R, Hallett M. Cerebral processes related to visuomotor imagery and generation of simple finger movements studied with positron emission tomography. Neuroimage 1998;7:73-85. 14. Lafleur MF, Jackson PL, Richards C, Malouin F, Evans A, Doyon J. Motor learning produces parallel dynamic functional changes during the execution and imagination of sequential foot movements. Neuroimage 2002;16:142-57. 15. Pascual-Leone A, Nguyet D, Cohen LG, Brasil-Neto JP, Cammarota A, Hallett M. Modulation of muscle responses evoked by transcranial magnetic stimulation during the acquisition of new fine motor skills. J Neurophysiol 1995;74:1037-45. 16. Decety J. Should motor imagery be used in physiotherapy? Recent advances in cognitive neurosciences. Physio Theory Pract 1993;9:193-203. 17. Warner L, McNeill ME. Mental imagery and its potential for physical therapy. Phys Ther 1988;68:516-21. 18. Yue G, Cole KJ. Strength increases from the motor program: comparison of training with maximal voluntary and imagined muscle contractions. J Neurophysiol 1992;67:1114-23. 19. Van Leeuwen R, Inglis JT. Mental practice and imagery: a potential role in stroke rehabilitation. Phys Ther Rev 1998;3:47-52. 20. Jackson PL, Lafleur M, Malouin F, Richards CL, Doyon J. Potential role of mental practice using motor imagery in neurological rehabilitation. Arch Phys Med Rehabil 2001;82:1133-41. 21. Page SJ, Levine P, Sisto SA, Johnston MV. Mental practice combined with physical practice for upper-limb motor deficit in sub-acute stroke. Phys Ther 2001;81:1455-62. 22. Page SJ, Levine P, Sisto SA, Johnston MV. A randomized efficacy and feasibility study of imagery in acute stroke. Clin Rehab 2001;15:233-40. 23. Yoo E, Park E, Chung B. Mental practice effect on line-tracing accuracy in persons with hemiparesis stroke: a preliminary study. Arch Phys Med Rehabil 2002;82:1213-18. 24. Stevens JA, Stoykov ME. Using motor imagery in the rehabilitation of hemiparesis. Arch Phys Med Rehabil 2003;84:1090-2. 25. Engardt M, Olsson E. Body weight-bearing while rising and sitting down in patients with stroke. Scand J Rehabil Med 1992;24:67-74. 26. Engardt M, Ribbe T, Olsson E. Vertical ground reaction force feedback to enhance stroke patients’ symmetrical body-weight distribution while rising/sitting down. Scand J Rehabil Med 1993;25:41-48. 27. Hesse S, Schauer M, Malezic M, Jahnke M, Mauritz KH. Quantitative analysis of rising from a chair in healthy and hemiparetic subjects. Scand J Rehabil Med 1994;26:161-6. 28. Carr JH, Shepherd RB. Neurological rehabilitation: optimizing motor performance. Oxford, UK: Butterworth Heinemann; 1998. 29. Malouin F, Belleville S, Richards CL, Desrosiers J, Doyon J. Working memory and mental practice outcomes after stroke. Arch Phys Med Rehabil 2004;84:177-83. 30. Hall CR, Pongrac J. Movement imagery questionnaire. London, Ontario, Canada: Faculty of Physical Education; 1983. 31. Roy M, Gosselin V, Lafleur M, Jackson PL, Doyon J. Évaluation des qualités psychométriques du Questionnaire d’Imagerie Kinesthésique. Science et Comportement 1998;27:S-191. 32. Podsiadlo D, Richardson S. The Timed “Up and Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991;39:142-8. 33. Gowland C, Stratford P, Ward M, et al. Measuring physical impairment and disability with the Chedoke-McMaster Stroke Assessment. Stroke 1993;24:58-63. 34. Dion L, Malouin F, McFadyen B, Richards CL. The rise-towalk task for assessing mobility after stroke. Neurorehabil Neural Repair 2003;17:83-92. Neurorehabilitation and Neural Repair 18(2); 2004 Mental Practice and Mobility after Stroke 35. Jackson PL, Lafleurs M, Malouin F, Richards CL, Evans AC, Doyon J. Practice of a sequential task with motor imagery modulates orbitofrontal functional organization. Neuroimage 2003;20:1171-80. 36. Ruby P, Decety P. Effect of subjective perspective taking during simulation of action: a PET investigation of agency. Nat Neurosci 2001;4:546-550. 37. Hall C, Schmidt D, Durand M-C, Buckolz E. Imagery and motor skills acquisition. In Sheikh AA, Korn ER, eds. Imagery in sports and physical performance. Amityville, NY: Baywood; 1994. p. 121-34. 38. Cheng PT, Wu SH, Liaw MY, Wong AM, Tang FT. Symmetrical body-weight distribution training in stroke patients and its effect on fall prevention. Arch Phys Med Rehabil 2001;8:1650-54. 39. Monger C, Carr JH, Fowler V. Evaluation of a home-based exercise and training programme to improve sit-to-stand in patients with chronic stroke. Clin Rehabil 2002;16:361-7. Neurorehabilitation and Neural Repair 18(2); 2004 40. Engardt M. Long-term effects of auditory feedback training on relearned symmetrical body weight distribution in stroke patients: a follow-up study. Scand J Rehabil Med 1994;26:65-9. 41. Carr JH, Shepherd RB, Nordholm L, Lynne D. Investigation of a new motor assessment scale for stroke patients. Phys Ther 1985;65:175-80. 42. Pai Y, Rodgers MW. Control of body mass transfer as a function of speed of ascent in sit-to-stand. Med Sci Sports Exer 1990;22:378-84. 43. Kralj A, Jaeger RJ, Munih M. Analysis of standing up and sitting down in humans. J Biomech 1990;23:1123-38. 44. Jackson, PL, Doyon J, Richards CL, Malouin F. The efficacy of combined physical and mental practice in the learning of a foot-sequence task after stroke: a case report. Neurorehabil Neural Repair 2004;18:106-11. 75