* Mark all that apply MYSELF In My
advertisement

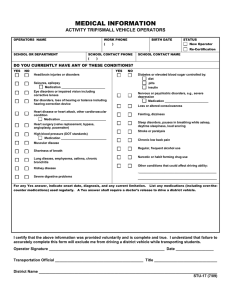
Medical History Return by July 1, 2013 H E A LT H C E N T E R PERSONAL & FAMILY HEALTH HISTORY * Mark all that apply Last name First name Date of Birth Current Past Treatment Student # Student’s cell phone # Student’s Home Street Address Home City Home State □ I am a Freshman □ Female 1. 2. 3. 4. 5. 6. □ I am a Transfer Student □ Male Primary Care Provider • Name: • Phone #: 8. Medical Specialist – (if applicable) • Name: • Phone #: • Specialty: • • Zip Height Weight Medication and/or Food Allergies Name Reaction ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ Medications taken regularly _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ Hospitalizations/Surgeries Please list ________________________________________________________________ ________________________________________________________________ ________________________________________________________________ I am taking medication or have a medical condition which lowers my immune system. No Yes (name) I have had Chickenpox disease No Yes (age or year) I have had a positive test for Mononucleosis No Yes (month/year) 7. • MYSELF MI In My Family ( Who)? AutoImmune Disorders Multiple Sclerosis Systemic Lupus Other: Blood Disorders Anemia Clotting Disorder Sickle Cell trait/disease Other: Cancer Specify: Cardio/Pulmonary Disorders Asthma Blood Clots Heart Disease High Blood Pressure High Cholesterol Other: Digestive Disorders Crohn's Disease GERD Peptic Ulcer Irritable Bowel Syndrome Other: Eating Disorders Anorexia Nervosa Binge Eating Bulimia Other: Endocrine Disorders Diabetes Thyroid condition Other Mental/Emotional Disorders Anxiety Bipolar Disorder Depression Schizophrenia Suicide Attempt Other: Neurological Disorders ADD/ADHD Cerebral Palsy Concussion(s) Migraine Headaches Seizures Other: Reproductive Health Amenorrhea Dysmenorrhea Ovarian cysts Other: STATEMENT OF AUTHORIZATION The information contained on this form is complete and I have not withheld any medical or mental health information. If any aspect of my health profile changes after submitting this form, I will notify the Hope Health Center of this/these changes in writing. I authorize the Student Health Center of Hope College to administer medical and surgical services, including immunizations and to perform routine and emergency diagnostic and therapeutic procedures as deemed necessary by duly licensed medical personnel. I understand that the Medical Director, or designee, serves as primary physician for medical care provided by the Hope Health Center. I understand that I will be required to undergo medical treatment for any current or future diagnosis of Latent Tuberculosis Infection (LTBI). Failure to do so will result in withdrawal from current coursework and living arrangements at Hope College. Signature of Student Date