fill out the Medical History form
advertisement

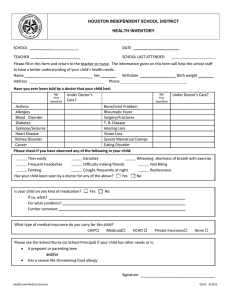
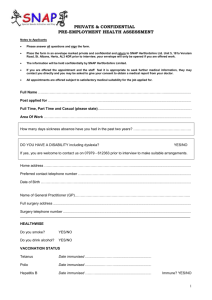
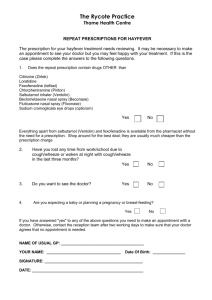
MEDICAL HISTORY Name: Click here to enter text. Address: Click here to enter text. Phone Cell Phone Click here to enter text. Click here to enter text. Date of Birth: Click here to enter a date. General Health History: Check all items that apply to past or present medical history. Explain yes answers in space below, and conditions that may limit participation in outdoor activities. ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ Ever been hospitalized? Ever had surgery? Recurrent/chronic illness? Recent infectious disease? Recent injury? Asthma/wheezing/shortness of breath? Diabetes? Seizures, Epilepsy? Headaches, Migraines? Wear glasses, contacts, protective eyewear? Hearing Impairment? Click here to enter text. List all medication you are presently taking. Click here to enter text. ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ Fainting or dizziness? Passed out/had chest pain during exercise? Heart condition? High or Low blood pressure? Back/joint disorders or problems? Muscle disorders? Bone disorders? Pregnancy? Allergies, Hayfever? Skin problems, conditions? Problems with falling asleep/sleepwalking? MEDICAL HISTORY If known, what is your blood type? ☐ A ☐ B ☐ + positive ☐ AB ☐ - negative ☐ O Have you had diphtheria/tetanus booster in the past 10 years? If no, we encourage you to get one. ☐ Yes ☐ No Please list any other information you feel we should know regarding your medical history. Click here to enter text. Name of primary doctor(s). Click here to enter text. Contact info of primary doctor(s). Click here to enter text. Please list three people to contact in case of an emergency. Name Relationship Address Telephone No. Click here to enter text. Click here to enter text. Click here to enter text. Phone Click here to enter text. Click here to enter text. Click here to enter text. Click here to enter text. Click here to enter text. Click here to enter text. Click here to enter text. Click here to enter text. Participation in this course is physically demanding. You should be free of any medical or physical condition that might create undue risk to yourself or others. If there is any doubt whatsoever about your ability to participate, it is your responsibility to consult with a medical doctor. Click here to enter text. Signature (may be digital) Click here to enter a date. Date