Center for Global Health & Diplomacy
University of North Florida
Jacksonville, Florid
September 12, 2012
A Global Perspective
Cecil B. Wilson, MD, MACP, President-Elect
World Medical Association
Caring, Ethics, Science
Global Situation
• All systems are on the move
• All systems are deeply rooted in cultural
ideas about society and values
• There is no evidence that one model is better
than another, if you do not define what you
want to achieve and whom you are willing to
trust
Global situation (2)
• Total inequality
• Some countries have systems for care for the population
others do not
• Currently the rich countries in this world satisfy their
need for health professionals by brain drain from poor
countries
• Health disparities may be a driving force for general
migration
• Is there a blue print to copy?
Strengthening the
health workforce A
country action Guide
In health care
thereis a
human
resource crisis
•Source: WHO World Health Report 2006
•Source: WHO World Health Report 2006
Global Migration of Physicians
Healthcare Financing
1.
2.
3.
4.
5.
6.
7.
General taxation
Social health insurance
Voluntary or private health insurance
Out-of-pocket payments
Donations to charities
Public-private partnerships
Market-based financial transaction taxes
Four Basic Systems Worldwide
•
•
•
•
The Beveridge Model
The Bismarck Model
The National Health Insurance Model
The Out-of Pocket Model
Beveridge (gov’t system)
• Health care provided and financed by gov’t
through tax payments
• Hospitals and clinics owned by gov’t
• Doctors are gov’t employees – GPs
capitation, specialists salary
• Co-payments none for most services
• Countries – Great Britain, Cuba, Spain, most
of Scandinavia and New Zealand
Bismarck (private insurance)
• Social insurance financed by employers and
employees through payroll deduction
• Plans cover everyone and are not for profit
• Single payment system negotiated by insurers
(240)
• Doctors and hospitals private
• Countries – Germany, France, Belgium, the
Netherlands, Japan, Switzerland
National Health Insurance
•
•
•
•
Gov’t run insurance into which everyone pays
Single payer
Private sector providers
Controls costs by limiting medical services
they will pay for and making patients wait
• Countries – Canada, Taiwan and South Korea
Out-of-pocket
• Underdeveloped countries with no health
care system
• The rich get medical care, the poor stay sick
or die
• Millions of people go their whole lives
without seeing a doctor
• Access – a village healer, home remedies
• Regions – Rural Africa, India, China and Latin
America
If you are in America
• Veterans and native Americans – Britain,
Cuba
• Employer provided insurance – Germany,
France, Japan, Switzerland *
• Medicare – Canada, Taiwan, South Korea
• Uninsured – Cambodia, rural India
* Insurance mandated and not for profit
Observations
• All systems are on the move
• All systems are deeply rooted in cultural
ideas about society and values
• More important than one or the other
feature is a national consensus
• It is a question of what values are most
important: freedom, choice, social
protection, profits
21
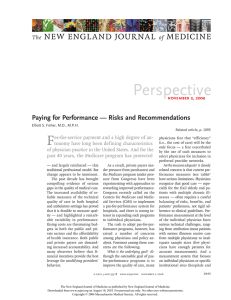
Average Health Care Spending per Capita, 1980–2009
Adjusted for differences in cost of living
Dollars
US
8000
NOR
7000
SWIZ
NETH
6000
CAN
DEN
5000
GER
FR
4000
SWE
3000
UK
AUS
2000
NZ
JPN
1000
0
1980
1984
1988
1992
1996
2000
2004
2008
THE
COMMONWEALTH
FUND
Source: OECD Health Data 2011 (June 2011).
22
Health Care Spending as a Percentage of GDP, 1980–2009
Percent
18
US
NETH
16
FR
14
GER
DEN
12
CAN
SWIZ
10
NZ
8
SWE
UK
6
NOR
AUS
4
JPN
2
0
1980
1984
1988
GDP refers to gross domestic product.
Source: OECD Health Data 2011 (June 2011).
1992
1996
2000
2004
2008
THE
COMMONWEALTH
FUND
2011 Economic Impact Survey
Office based physicians, Florida *
•
•
•
•
•
•
Total office based physicians – 39,432
Total jobs – 230,000
Jobs, average per physician – 5.9
Output - $64.5 billion – 8.6% of FL’s GDP
Wages & Benefits - $40 billion
Taxes - $2.3 billion state and local
* nationally $1.4 trillion economic activity and 4
million jobs
The Future
1. Scientific advances will continue to
astound, with innovative and creative ways
to care for the sick
2. An aging population and an accompanying
epidemic of chronic disease
3. Healthcare system changes that emphasize
continuity and coordination of care –
investments in quality, prevention and
wellness
1. Scientific Advances
Scientific advances will continue to
astound, with innovative and
creative ways to care for the sick
James Watson
Economic Impact Human Genone Project
1988 to 2010
•
•
•
•
$5.6 b – Federal Gov’t investment *
$796 b – research and industry activity
$244 b – personal income
3.8 m – job years of employment
In 2010 genomics-based industry generated
• $3.7 b – federal taxes
• $2.3 b – US state and local taxes
Future of Medicine
2. Demographics
An aging population and an
accompanying epidemic of chronic
disease
Workforce solutions
• National Health Services Corp scholarship
and loan repayment programs
• Title VII health professions program
payment programs
• Primary care training
• National Commission on Workforce
• Grants to adopt patient-Centered Medical
Homes, and residency programs at teaching
health centers
Workforce solutions (2)
• 10 percent bonus payments for primary care
• Medicaid payments equal to Medicare
• Center for Medicare and Medicaid Innovation
• Redistribution of unfilled residency positions
to primary care and general surgery
• States option to enroll patients in primary
care medical homes
3. Health System Changes
Healthcare system changes that
emphasize continuity and
coordination of care – investments
in quality, prevention and wellness
AMA Physician Innovators
Physicians Innovator Committee
– Formed among doctors active in new
models
– Members from across medicine
– Goals:
• Offer physicians resources and
information
• Improve patient care
• Maximize financial stability
AMA Guidelines on ACOs
Accountable care organizations must:
• Be physician-led
• Be voluntary for patients and physicians
• Include flexible organizational criteria
• Offer support for independent and smallpractice physicians
• Include antitrust and fraud and abuse reform
• Use quality measures driven by physicians
Medicare ACOs: A Win
• Participating physicians now share in every
dollar of cost savings without a threshold
• Less burdensome “meaningful use” criteria for
electronic health records
• Number of required measures cut in half
• New application process allows time to prepare
• $170 million in advance payments to physicianowned ACOs for start-up costs
• Improved antitrust process eliminates
burdensome mandatory review
The Future
1. Science
2. Demographics
3. Structure
Caring, Ethics, Science
 0
0