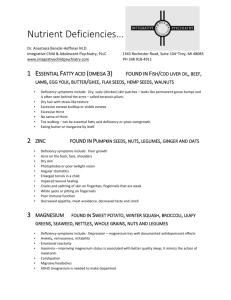
Water-soluble vitamins
advertisement

Vitamins
Definitions:
Vitamins are organic compounds required by the body in trace amounts to
perform specific function, and can not be synthesized by humans, or can not be
synthesized in adequate (sufficient) quantities to meet needs.
When present in inadequate quantities, deficiency states results leading to
disease.
Modern views suggest that more quantities than RDIS might be needed to
prevent some chronic diseases.
Provitamins are precursors of vitamins that could be converted into
vitamins inside the body e.g. Carotenes are provitamin A.
Vitamers: These are different forms of one vitamin e.g. Vitamin D has
2 vitamers; D2 &D3.
Water-soluble vitamins
Water-soluble vitamins
They include the B-group vitamins and
vitamin C. These are:
Not stored extensively.
Required regularly in the diet.
Generally non-toxic in excess (within
reason).
All B vitamins are coenzymes in metabolic
pathways.
Thiamin (B1)
Co-factor or active form and Function
Co-factor active form:
Thiamine pyrophosphate ( TPP).
TPP acts as cofactor in the following enzyme systems:
- Pyruvate dehydrogenase (pyruvate
acetyl CoA)
-α-Ketoglutarate dehydrogenase
(α-Ketoglutarate
succinyl CoA)
-Oxidative decarboxylation of α–keto acids derived from leucine, isoleucine,
valine, threonine and serine.
-Trans ketolase reaction in pentose phosphate pathway
TPP also supports normal appetite.
And ,
Is needed for normal brain and CNS function.
Deficiency
Decreased activity of the dehydrogenases ,
leading to
-accumulation of pyruvate and lactate.
-Decreased acetyl CoA and ATP formation ,
thus decreased acetylcholine and CNS
activity.
Decreased HMP shunt results in low levels
of NADPH , Hence decrease fatty acid
synthesis necessary for myelin formation
and causing peripheral neuropathy.
Deficiency:
Severe Deficiency
leads to beri beri
Diagnosing deficiency
This is done by measuring the transketolase activity in RBCs , before
and after the addition of TPP . A greater than 30% increase in activity
indicates deficiency.
Requirement , sources and toxicity
RNI:
1.0mg/day for men; 0.8mg/day for women.
Increased requirement in case of high carbohydrates diet.
Sources:
Wholegrain cereals, liver, pork, yeast, dairy produce and legumes.
Toxicity:
Rare but an excess causes headaches , insomnia and dermatitis.
Riboflavin ( B2)
Co-factor or active form and Function:
Co-factor or active form :
Flavin mononucleotide (FMN) and flavin-adenine
dinucleotide (FAD).
Function of active forms:
FAD and FMN act as electron carriers in oxidoreduction
reactions (usually tightly bound to the apoenzyme).
Deficiency
Diagnosis of deficiency
Erythrocyte glutathione reductase level is a good measurement of
deficiency.
HPLC measurement of B2 in blood is used also for diagnosis of deficiency.
Requirement and sources
RNI:
1.3mg/day for men; 1.1mg/day for women.
Sources:
Milk, eggs, liver.
Riboflavin is readily destroyed by ultraviolet light.
Niacin ( B3)
Co-factor
or active form
Co-factor or active form :
NAD+ and NADP+
Nicotinamide-adenine dinucleotide and its phosphate.
A certain amount of NAD and NADP can be
synthesized in the body from the amino acid
tryptophan, in reactions requiring pyridoxal P
Functions and Deficiency
Requirement and sources
RNI:
17mg/day for men; 13mg/day for women.
Sources:
Wholegrain cereals, meat, fish .
It can be synthesized in the body from the amino
acid tryptophan, but requires other B vitamins as
co-factors ( Vit.B1, B2 &B6) ,and is not very
efficient ( 60mg Tryp. To make 1mg of niacin)
Assessment of nutritional status
Measurement of urinary Nmethylnicotiamide and 2-pyridone
reflect nutritional status.
Pantothenic acid ( B5)
Co-factor or active form and function
Co-factor:
Coenzyme A , ACP
Examples of enzyme systems needing CoA:
- Pyruvate dehydrogenase
- α-Ketoglutarate dehydrogenase
- Oxidative decarboxylation of α-keto acids
- Fatty acid activation
- Generally, a carrier of acyl groups.
Functions and Deficiency
Sources:
Most foods but eggs, liver and yeast are very good sources.
Biotin
Structure:
Functions and Deficiency
Sources
-Most foods, especially egg yolk, offal, yeast
and nuts.
-A significant amount is synthesized by
bacteria in the intestine.
Pyridoxine
Structure:
Active form
All
three forms can be converted to the active coenzyme
pyridoxal phosphate
Functions and Deficiency
Causes of Deficiency:
Deficiency is rare but can be seen in :
- Newborn babies fed formula milk deficient in the vitamin.
- Elderly people and alcoholics.
- Women taking oral contraceptives.
- Patients on isoniazid therapy for treatment of tuberculosis.
Requirement and sources:
RNI:
1.4mg/day for men; 1.2mg/day for women.
Increased requirement in case of high protein diet.
Sources:
Whole grains (wheat or corn), meat, fish and poultry.
Toxicity
This is rare.
In fact vit.B6 is actually used in the
treatment of PMT. However ,
neurological symptoms have been
observed at intake >2g/day.
Improvement , but not complete
recovery occurs when the vitamin is
discontinued.
Folic acid
Active form and action:
Active form is 5,6,7,8-THF .
The function of THF derivatives is to carry and transfer
various forms of one carbon units during biosynthetic
reactions. The one carbon units are either methyl, methylene,
methenyl, formyl or formimino groups.
Absorption and storage:
When stored in the liver or ingested folic acid exists in a polyglutamate form.
Intestinal mucosal cells remove some of the glutamate residues through the
action of the lysosomal enzyme, conjugase.
The removal of glutamate residues makes folate less negatively charged (from
the polyglutamic acids) and therefore more capable of passing through the
basal lamenal membrane of the epithelial cells of the intestine and into the
bloodstream.
Folic acid is reduced within cells to dihydrofolate and then tetrahydrofolate
(principally in the liver where it is stored) through the action of dihydrofolate
reductase enzyme (DHFR), an NADPH requiring enzyme.
Malabsorption syndromes such as tropical sprue, celiac disease, and
Crohn disease greatly affect the absorption of folate, also some drugs
such as sulfasalazine may interfere with folate absorption. The most
common circulating form of the vitamin is 5-methyltetrahydrofolate.
Functions and Deficiency
Causes of deficiency
Decreased intake :Poor dietary habits as those of chronic alcoholics can lead to
folate deficiency (for adult about 1 mg/day folate is considered enough for
treatment of deficiency if there is no malabsorption).
The predominant causes of folate deficiency in non-alcoholics are impaired
absorption or metabolism or an increased demand for the vitamin.
Increased demand :The most common condition requiring an increase in the
daily intake of folate is pregnancy (it is recommended to give pregnant ladies
400 ug/day folate).
Drugs :Certain drugs such as anticonvulsants and oral contraceptives can
impair the absorption of folate.
Others may interfere with its metabolism , e.g. dihydrofolate inhibitors.
Secondary to vitamin B12 deficiency.
Folate deficiency in pregnancy
The development of the neural tube in
the fetus is dependant on the
presence of folic acid.
Therefore , it is advisable for women
planning a pregnancy to take
prophylactic folate supplements to
reduce the risk of neural tube defects
such as spina bifida or anencephaly.
Requirement and sources
RNI:
200mg/day.
Sources:
Green vegetables, liver and wholegrain
cereals.
Vitamin B (cobalamin)
Absorption:
The vitamin must be hydrolyzed from protein in food in
order to be absorbed.
Hydrolysis occurs in the stomach by gastric acid following
consumption of animal meat.
The vitamin is then bound by intrinsic factor ( IF), a
glycoprotein secreted by parietal cells of the stomach, and
carried to the ileum where the complex is bound to
receptors on the mucosal cells ,and vit.B12 is absorbed, the
absorption is enhanced by calcium ions and pH >6.
Transport and Storage
Following absorption the vitamin is transported to the liver in the
blood bound to carrier globulins; transcobalamin II.
About 2-3 g of the vitamin are stored in the liver ( enough for about
2 years requirement )
Active Form:
Two active forms:
- deoxyadenosyl cobalamin
and
- methyl cobalamin
Function
Till now there are only two known reactions in the body that require
vitamin B12 as a cofactor:
The first one, during the catabolism of fatty acids with an odd number
of carbon atoms ,and during the catabolism of amino acids valine,
isoleucine and threonine .
One of the enzymes in this pathway, methylmalonyl-CoA mutase,
requires vitamin B12 as a cofactor in the conversion of methylmalonylCoA to succinyl-CoA.
The 5'-deoxyadenosylcobalamin derivative of cobalamin is required
for this reaction.
The second reaction requiring vitamin B12 (methylcobalmin) catalyzes
the conversion of homocysteine to methionine and is catalyzed by
homocysteine methyl-transferase.
It requires methyl-tetrahydrofolate as cofactor ( as a carrier of the
methyl group).
Therefore , in case of vit.B12 deficiency the THF is trapped as methylTHF.
Requirement and sources
RNI:
1.5mg/day.
Sources:
Only animal sources: liver, meat, dairy
foods; therefore vegans are at risk of
deficiency.
Vitamin B12 deficiency:
The liver can store up to 2-3 years of vitamin B12, hence
deficiencies of this vitamin are rare.
Reduced intake , as in total vegetarians , could cause deficiency.
There are many causes that may affect the absorption of
vitamin B12 such as:
- achlorhydria,
- total gastrectomy
- gastric atrophy (as in aging and pernicious anemia), ,
- impaired pancreatic function , and
- production of antibody against the intrinsic factor (pernicious
anemia) .The commonest cause of deficiency.
- Some drugs (anticonvulsant, neomycin, paraaminosalicylic
acid, Cholestyramine and alcohol) also cause vitamin B12
deficiency.
- Diseases of terminal ileum , e.g. Crohn’s disease or
tuberculosis.
- Blind – loop syndrome: parasites compete for B12.
Vitamin B12
deficiency(continue)
Deficiency can cause two main problems:
-Pernicious anemia which is a megaloblastic
anemia The anemia resulting from impaired DNA
synthesis due to a block in purine and thymidine
biosynthesis.
The block in nucleotide biosynthesis is a
consequence of the effect of vitamin B12 on
folate metabolism. When vitamin B12 is deficient
essentially all of the folate becomes trapped as
the N5-methyltetrahydrofolate derivative and
cannot participate in nucleotide biosynthesis.
Vitamin B12
deficiency(continue)
Neurological
complications
(subacute
combined degeneration of the spinal cord of
lateral {motor} and posterior {sensory}
columns and peripheral neuritis leads to
numbness
tingling
and
weakness
of
extremities) also are associated with
vitamin B12 deficiency and result from a
progressive demyelination of nerve cells.
The demyelination is thought to result from
the increase in methylmalonyl-CoA that
result from vitamin B12 deficiency.
Deficiency
Ascorbate (Vitamin C)
Active form and function:
Active form is ascorbate
Functions :
1-Important antioxidant, inactivates free oxygen radicals , and protects
other antioxidant vitamins A and E.
2- Essential for iron absorption , reducing F3+ to F2+.
3 - It has mild anti-histamine effect.
4- important for the immune system (antibodies and white blood cells),
strengthening resistance to infection.
5- Coenzyme in hydroxylation reactions :
- Collagen formation (essential for formation of hydroxylysine and
hydroxyproline.
- Formation of corticosteroid hormones in the adrenal gland.
-It is important for formation of adrenaline and noradrenaline.
Requirement and sources
RNI:
40mg/day.
Sources:
Citrus fruit, tomatoes, berries and green
vegetables.
Deficiency
Defective collagen synthesis causes scurvy
which is characterized by bleeding gum,
bruises.
Hypochromic microcytic anemia may take
place due to decreased iron absorption.
Low levels of this important antioxidant
may increase risk of minor infections and
heart disease.
Diagnosis of deficiency is by measuring
vitamin C level in blood.
Effect of mega dose and toxicity
It is thought that large doses of 1-4
g/day can :
- decrease the severity of symptoms of
cold (but not decrease the incidence )
- decrease the incidence of CHD and
certain cancers by scavenging free
radicals.
Chronic intake of large doses may lead
to formation of kidney stones (
ascorbate is metabolized to oxalate in
the body – uric acid excretion is also
increased)
Assessment of nutritional status
•
•
•
Vitamin C (ascorbate ) can be measured in
serum.
Normal Level is .4 – 1.2 mg/dl
.1-.2 mg/dl indicate moderate deficiency
<0.1 mg/dl indicate severe deficiency (high
risk of scurvy)
Vitamin C load test:
Mega dose of Vitamin C is given orally, and
urinary excretion is measured.
Most of the dose is excreted within hours if
status is adequate
No or little ascorbate appear in urine in case
of deficiency (tissue de-saturation)