procedure for the use of the syringe pump in palliative and end of life

PROCEDURE FOR THE USE OF THE SYRINGE PUMP IN
PALLIATIVE AND END OF LIFE CARE
(INCLUDING GUIDELINES FOR ADMINISTRATION OF DRUGS)
Version:
Name of originator/author:
Date issued:
Review date:
1.0 (31/01/2013)
Val Revill
31/01/2013
28 th February 2014
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care February 2013
Contents
1 . Scope
2. Glossary of terms
3. Aim
3.1 Client Group
3.2 Staff Group
4. Introduction
5. Indications for using the syringe pump
6. Medication
6.1 Combinations of more than one drug in a syringe pump
7. Drugs
7.1 Diamorphine
7.2 Oxycodone
7.3 Cyclizine
7.4 Metoclopramide
7.5 Haloperidol
7.7 Midazolam
7.6 Levomepromazine
7.8 Hyoscine Butylbromide
7.9 Hyoscine Hydrobromide
7.10 Glycopyrronium
7.11 Dexamethasone
7.12 Octreotide
7.13 Drugs not suitable for use in the syringe driver
8. The T34 McKinley Syringe Pump
8.1 Information for patients
8.2 Labelling of the syringe
8.3 Calibration of a syringe pump
8.4 Decontamination of syringe pump
8.5 Decontamination of holster bag
9. Standard Operating Procedure
10. Skin site selection and skin care
10.1 Sites suitable for subcutaneous infusion
10.2 Sites not suitable for subcutaneous infusion
10.3 Care of the skin site and checks
11. Trouble shooting
12. Specialist Palliative Care Advice
13. References
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
30
31
32
24
28
28
28
29
21
21
21
22
22
4
4
4
2
4
6
6
5
6
15
16
17
18
19
8
8
9
10
11
12
13
14
20
21
1
1. SCOPE
This document is for doctors and registered nurses who have attended organisation approved training sessions on how to use the McKinley T34 Syringe Pump for administration of drugs by subcutaneous infusion (Cooper and Mitten 2000; Danne et al 2000; Dickman et al 2002).
These guidelines have been written with the aim of providing information on the safe administration of medications via the subcutaneous route to relieve distressing symptoms in those patients receiving palliative care. Whilst other syringe driver models are available nationally, the
McKinley T34 Syringe Pump is the only model currently approved for use in the Northern
Lincolnshire locality.
Key Points
All staff using the syringe pump will have been trained in its use and a record of the
training is documented
All staff trained in the use of the syringe pump must be fully conversant with these guidelines and have self-assessed as competent.
All actual and near miss adverse events involving the syringe pump are reported via each organisations incident reporting mechanism.
All syringe pumps must be maintained according to your organisations equipment maintenance policy.
The document will guide the Registered Nurse / Doctor / Pharmacist to
Safely prescribe or dispense medications for a syringe pump
Safely administer medications via a syringe pump
Ensure that the rate setting is correct and that the machine is running to time
Early detection of uncontrolled symptoms
Early detection of functional problems related to the device - trouble-shooting guide
Early detection of occlusion, or discolouring of solutions being administered
The document: -
Explains the indications for choosing the subcutaneous route of administration of medicines e.g. swallowing problems, uncontrolled nausea, uncontrolled vomiting, intestinal obstruction, too weak to take oral medication, terminal agitation, malabsorption.
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
2
Demonstrates the procedure for setting up the McKinley T34 syringe pump and the equipment required.
Explains how to select skin site and which skin sites should not be used.
Explains how to check if the device is running correctly.
Explains how to draw up and prepare solutions.
Illustrates the medications that can be used in a syringe pump and information about the combinations of drugs that can be used.
Clarifies which medications should not be used in a syringe pump.
Provides a list of contact numbers for specialist palliative care advisers
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
3
2.
GLOSSARY OF TERMS
Accountable Responsible for something or to someone
Competent
Possessing the skills and abilities required for lawful, safe and effective professional practice without direct supervision.
DPOWH Diana Princess of Wales Hospital
LLH mg
Lindsey Lodge Hospice
Milligram ml mm
Millilitre
Millimetre
NEL North East Lincolnshire
NELCCG North East Lincolnshire Clinical Commissioning Group
NL
NL&G
NMC
CPG
SAH
SGH
North Lincolnshire
Northern Lincolnshire and Goole Hospitals NHS Foundation Trust
Nursing and Midwifery Council
Care Plus Group
St Andrew’s Hospice
Scunthorpe General Hospital
3. AIM
Safe administration of medications to relieve distressing symptoms in those patients receiving palliative care.
To ensure that the rate setting is correct and the machine is running to time
Early detection of functional problems related to the device
Early detection of occlusion or discolouring of solutions being administered
3.1 CLIENT GROUP
Adults receiving palliative care for whom alternative routes of medication administration are no longer appropriate. e.g. swallowing problems, uncontrolled nausea, uncontrolled vomiting, malabsorption, intestinal obstruction, too weak to take oral medication, terminal agitation and care in the last days of life.
3.2
STAFF GROUP
Registered nurses and doctors who have attended organisation approved training sessions on how to use the McKinley T34 Syringe Pump in NL&G, CPG, NELCCG, Yarborough Clee Care, St Andrew’s
Hospice, NL community, Lindsey Lodge Hospice and Care Homes within the Northern Lincolnshire locality.
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
4
4.
INTRODUCTION
These guidelines are intended for the subcutaneous infusion of drugs only via the McKinley T34
Syringe Pump.
The syringe pump should be used where there are clear indications to do so. It is important to discuss the syringe pump use with the patient/carer/relatives to ensure their full understanding and compliance.
The Nursing & Midwifery Council – The Code 2008
““As a professional, you are personally accountable for actions and omissions in your practice and must always be able to justify your decisions”
“The administration of medicines is an important aspect of the professional practice of persons whose names are on the Council’s register. It is not solely a mechanistic task to be performed in strict compliance with the written prescription of a medical practitioner (now independent/supplementary prescriber). It requires thought and the exercise of professional judgment”
Keep your skills and knowledge up to date
You must have the knowledge and skills for safe and effective practice when working without direct supervision.
You must recognise and work within the limits of your competence.
You must take part in appropriate learning and practice activities that maintain and develop your competence and performance.
The General Medical Council (2006)
“The duties of a doctor registered with the GMC states that as a Doctor you must”
Respect the rights of patients to be fully involved in their care
Keep your professional knowledge and skills up to date
Recognise the limits of your professional competence
Work with colleagues in the ways that best serve patients interests
Pharmacists will refer to and abide by The Royal Pharmaceutical Society of Great Britain Code of
Ethics.
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
5
5. INDICATIONS FOR USING THE SYRINGE PUMP
NB: Uncontrolled pain is not a reason to commence the syringe pump (Cooper and Mitten 2000;
Danne et al 2000; Dickman et al 2005).
The indications are as follows:
Swallowing problems – e.g. oral or oesophageal cancers, when liquid or transdermal preparations are inappropriate or patient is unable to swallow liquid preparations.
Uncontrolled nausea – i.e. oral medication not effective (NB: resume oral medication when
controlled).
Uncontrolled vomiting – Unable to tolerate oral medication (NB: resume oral medication when
controlled).
Intestinal obstruction
Too weak to take oral medication – semi-conscious, coma.
Terminal agitation – Even if not accompanied by pain.
Malabsorption – Rare but take into consideration when symptoms are not being managed despite titration of appropriate oral medication (Cooper and Mitten 2000; Danne et al 2000;
Dickman et al 2005; Johnson 1998; Northern Lincolnshire and Goole Hospitals NHS Trust
(NL&G) 2003).
NB: If patient has transdermal Fentanyl (Durogesic®)) patch insitu DO NOT remove - please seek
Specialist Palliative Care advice
6. MEDICATION
6.1 Combinations of More than One Drug in a Syringe Pump
Situations often arise in palliative care where two or more drugs are required to be combined in one syringe. Many combinations have been used in clinical practice. Supporting compatibility data
/ information should be obtained from Section 5.2 of this guideline prior to using combinations of drugs.
General principles that should be adhered to when two or more drugs are used in a syringe driver:
Mixtures of drugs may be termed physically compatible. This implies that on mixing, the solution remains colourless, clear and free from particles over the specified time.
This does not confirm stability because unseen chemical reactions may occur and would only become apparent by laboratory analysis or an adverse event affecting the patient.
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
6
Rational use of drugs should be observed. It is important to ensure that the drugs are pharmacologically and chemically distinct.
The majority of these drugs are not licensed for administration by subcutaneous infusion or in combinations. The recommendations for combinations and doses given in
Section 5.2 of this guidance reflect both local and national experience and practice.
Two Drugs
The majority of published laboratory stability data is for 2 drug combinations. When the use of two drugs is deemed necessary, well-validated reference sources should be used.
Three Drugs
There is little laboratory data available on the mixing of three drugs in a syringe. The majority of laboratory data is concentration dependent, therefore one cannot assume that if a combination is compatible at one concentration it applies to all concentrations.
If you are unsure about any combinations, please seek advice from the Specialist Palliative Care team.
Diluent
N.B. Whilst Water for Injections is the diluent of choice; the following drugs may be mixed with either Water for Injection or 0.9% Saline unless explicitly stated otherwise .
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
7
7.1
Drug Recommended Dose Comments
DIAMORPHINE
Used because of its high solubility
Available as: -
5mg ampoules
10mg ampoules
30mg ampoules
100mg ampoules
500mg ampoules
No maximum dose. Titrate upwards until pain is controlled and there are no intractable side effects.
Please carefully monitor for toxicity.
When converting from oral Morphine divide total
24 hour dose by 3 to obtain total 24 hour dose of
Diamorphine
Example One
A patient taking modified release oral Morphine
Sulphate (e.g. MST / Zomorph) 60mg BD will require 40mg of subcutaneous Diamorphine for equivalent pain control i.e.
60 + 60 = 120mg oral Morphine / 24 hours
120mg divided by 3 = 40 mg subcutaneous
Diamorphine / 24 hours
To calculate the appropriate therapeutic dose of medication for breakthrough pain, calculate the total amount of Diamorphine given in the driver over 24 hours and divide by 6, e.g. Patient taking
40mg of Diamorphine subcutaneously over 24 hours.
40 divided by 6 = 5mg Diamorphine subcutaneously PRN (to nearest rounded figure )
Caution in renal failure
If pain was not controlled previously, increase total daily dose by one third to one half.
N.B.do not increase if malabsorption of oral medication is considered a contributing factor
It is advisable to have a one sixth of the total 24-hour dose prescribed as subcutaneous injection for breakthrough pain if there is concern about adequate pain relief.
When starting a patient on a syringe driver it is advisable to give an initial bolus dose subcutaneously to raise blood plasma levels quickly as the subcutaneous infusion has a slow onset of action.
Example Two
For combinations of
Diamorphine with other drugs please see individual drug tables.
A patient taking 120mg of modified release Oral
Morphine (e.g. MST / Zomorph) bd will require 80 mgs of subcutaneous Diamorphine over 24 hours i.e.
120 mg x 2 = 240mg oral Morphine / 24 hours
240 mg divided by 3 = 80 mg subcutaneous
Diamorphine / 24 hours
To calculate the appropriate therapeutic dose of medication for breakthrough pain, calculate the total amount of Diamorphine given in the driver over 24 hours and divide by 6, e.g. Patient taking
80mg of Diamorphine subcutaneously over 24 hours
80 divided by 6 = 15mg Diamorphine subcutaneously PRN (to nearest rounded figure )
NB: Reassess daily - all breakthrough analgesics used in previous 24 hours to be considered in dosage
calculations.
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
8
7.2
Drug
OXYCODONE
Available as: -
10mg/ml ampoules
50mg/ml ampoules
Recommended Dose Comments
No maximum dose. Titrate upwards until pain is controlled ensuring there are no intractable side effects.
When converting from oral Oxycodone
(Oxycontin) divide total 24 hour dose by 2 to obtain total 24 hour dose of subcutaneous
Oxycodone
Example One
A patient taking oral Oxycodone (Oxycontin) 40 mg bd will require 40mg of subcutaneous
Oxycodone for equivalent pain control i.e.
40 + 40 = 80mg oral Oxycodone / 24 hours
80mg divided by 2 = 40 mg subcutaneous
Oxycodone/ 24 hours
To calculate the appropriate therapeutic dose of medication for breakthrough pain, calculate the total amount of Oxycodone given in the syringe driver over 24 hours and divide by 6, e.g. Patient taking 40mg of Oxycodone subcutaneously over 24 hours.
40 ÷ 6 = 5mg Oxycodone subcutaneously PRN
(to nearest rounded figure)
Example Two
If pain was not controlled previously, increase total daily dose by one third to one half. N.B.do not increase if malabsorption of oral medication is considered a contributing factor
It is advisable to have a one sixth of the total 24-hour dose prescribed as subcutaneous injection for breakthrough pain if there is concern about adequate pain relief.
When starting a patient on a syringe driver it is advisable to give an initial bolus dose subcutaneously to raise blood plasma levels quickly as the subcutaneous infusion has a slow onset of action.
Diluent
Water for injection or
0.9% Saline
Compatibility
Do not mix with subcutaneous
Cyclizine
A patient taking 150mg of Oxycodone
(Oxycontin) bd will require 120 mgs of subcutaneous Oxycodone over 24 hours i.e.
150 + 150 = 300mg oral Oxycodone / 24 hours
300 ÷ 2 = 150mg subcutaneous Oxycodone/
24hrs
To calculate the appropriate therapeutic dose of medication for breakthrough pain, calculate the total amount of Oxycodone given in the syringe driver over 24 hours and divide by 6, e.g. Patient taking 150mg of Oxycodone subcutaneously over 24 hours
150 divided by 6 = 25mg Oxycodone subcutaneously PRN
NB: All breakthrough medication used in previous 24 hours to be included in dosage calculations.
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
9
7.3
Drug
CYCLIZINE
Available as: -
50mg / ml ampoules
Recommended Dose
50mg – 150mg / 24 hours
Usual starting dose is 150mg
NB: Seek Specialist Palliative Care advice if
maximum dose is not effective
Comments
Anti-emetic (Anti-histamine) useful for nausea and vomiting due to vagal stimulation from gastrointestinal tract (i.e. constipation, colic) and genitourinary tract or raised intra cranial pressure.
Acceptable combinations in syringe based on laboratory data and clinical practice at recommended doses and concentrations:
3 drugs
Cyclizine + Diamorphine
+Haloperidol
(Concentration dependent) or
+ Midazolam
(Concentration dependent) or
+ Hyoscine Hydrobromide
(Concentration dependent)
2 drugs
Cyclizine
+Haloperidol or
+ Diamorphine (At concentration less than 10mg / ml of each drug)
Incompatible with Saline
0.9%
Use Water for Injection as diluent
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
10
7.4
Drug Recommended Dose Comments
METOCLOPRAMIDE
Available as: -
10mg / 2ml ampoules
30mg – 60mg / 24 hours
Usual starting dose 30mg
NB: Seek Specialist Palliative Care advice if
maximum dose is not effective
Concurrent use of Cyclizine and Metoclopramide antagonises the prokinetic effect of Metoclopramide – do not combine.
Increased risk of extrapyramidal side effects in patients less than 20 years old (especially women) if combined with Haloperidol or Levomepromazine.
Do not use if complete intestinal obstruction is suspected.
Promotes gastric emptying
Acceptable combinations in syringe based on laboratory data and clinical practice at recommended doses and concentrations:
3 Drugs
Metoclopramide
+ Diamorphine
+ Haloperidol or
+ Midazolam
2 Drugs
Metoclopramide
+ Diamorphine
(Concentration dependent) or
+ Midazolam
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
11
7.5
Drug Recommended Dose Comments
HALOPERIDOL
Available as: -
5mg / ml ampoules
1.5mg – 10mg / 24 hours
Usual anti-emetic starting dose is 1.5mg – 5mg
/ 24 hours
Use higher doses if sedative or antipsychotic action required e.g. 10mg / 24 hours
NB: Seek Specialist Palliative Care advice if
maximum dose is not effective
Anti-emetic of choice to prevent opiate induced nausea and vomiting.
Side-effects include
Sedation
Dizziness
Headache
Skin rashes
Acceptable combinations in syringe based on laboratory data and clinical practice at recommended doses and concentrations:
3 Drugs
Haloperidol + Diamorphine
+ Cyclizine
(Concentration dependent) or
+ Metoclopramide or
+ Midazolam
(Concentration dependent) or
+ Hyoscine Hydrobromide
2 Drugs
Haloperidol
+ Hyoscine Hydrobromide or
+ Midazolam or
+ Cyclizine or
+ Diamorphine
Incompatible with Saline
0.9%
Use Water for Injection as diluent
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
12
7.6
Drug Recommended Dose Comments
LEVOMEPROMAZINE
Available as: -
25mg / ml ampoules
6.25mg – 50mg / 24 hours
(higher doses can be used if indicated – please contact specialist palliative care team for advice)
For anti-emetic action: starting dose
6.25mg – 12.5mg / 24 hours
For sedative effect: starting dose
12.5mg – 25mg / 24 hours
NB: Seek Specialist Palliative Care advice if
maximum dose is not effective
Anti-emetic with a broad action.
Powerful sedative at higher doses – useful for very agitated patients.
Side-effects
Somnolence (especially at doses higher than 25mg
/day)
Postural hypotension
Extra-pyramidal effects at higher doses
Use 0.9% Sodium Chloride as diluent
Can sometimes cause local skin reaction.
Acceptable combinations in syringe based on laboratory data and clinical practice at recommended doses and concentrations:
3 Drugs
Levomepromazine
+ Diamorphine
+ Hyoscine hydrobromide
(Concentration dependent) or
+ Hyoscine Butylbromide
2 Drugs
Levomepromazine
+ Diamorphine
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
13
7.7
Drug Recommended Dose Comments
MIDAZOLAM
Available as: -
10mg / 5ml ampoules
Or
10mg / 2ml ampoules.
5mg – 60mg / 24 hours
Starting dose 5 – 10mg over 24 hrs
Ensure careful titration when increasing dose.
NB: Seek Specialist Palliative Care advice if maximum dose is not effective
Benzodiazepine with anxiolytic, anticonvulsant and amnesic properties.
Useful for agitation and in terminal stages.
May cause sedation
Acceptable combinations in syringe based on laboratory data and clinical practice at recommended doses and concentrations:
3 Drugs
Midazolam + Diamorphine
+ Haloperidol or
+ Hyoscine Hydrobromide or
+ Metoclopramide or
+Hyoscine Butylbromide or
+ Cyclizine
2 Drugs
Midazolam
+ Diamorphine or
+ Haloperidol or
+ Hyoscine Hydrobromide or
+ Metoclopramide
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
14
7.8
Drug
HYOSCINE
BUTYLBROMIDE
Do not confuse with
Hyoscine Hydrobromide
Available as: -
20mg / ml ampoules
Recommended Dose
For colic:
60mg – 120mg / 24 hours
(higher doses sometimes used)
Usual starting dose 60mg
For respiratory secretions:
20mg – 60mg / 24 hours
Comments
Useful for spasm of smooth muscle (gastro-intestinal and ureteric colic)
Used to dry up noisy respiratory secretions
Less likely to cause CNS effects (including sedation) than Hyoscine Hydrobromide
Acceptable combinations in syringe based on laboratory data and clinical practice at recommended doses and concentrations:
3 Drugs
Hyoscine Butylbromide +
Diamorphine
+ Levomepromazine or
+ Midazolam
2 Drugs
Hyoscine Butylbromide +
Diamorphine or
+ Haloperidol
+ Midazolam
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
15
7.9
Drug
HYOSCINE
HYDROBROMIDE
Do not confuse with
Hyoscine Butylbromide
Available as: -
400 microgram / 1ml ampoules
600 microgram / 1ml ampoules
Recommended Dose Comments
For bronchial secretions:
800 micrograms –
2400 micrograms / 24 hours
Usual starting dose
1200 micrograms, reduce if patient frail and
/ or elderly
For Colic: 600 micrograms– 1200 micrograms / 24 hours
NB: Hyoscine Butylbromide may be preferred for colic.
Anti-cholinergic drug
Use to dry up noisy respiratory secretions (it may not relieve the noise of existing secretions but is likely to prevent further exacerbation)
May also relieve colic associated with intestinal obstruction.
Some anti-emetic action
Side effects – more likely if dose
exceeds 1200 micrograms
Dry mouth
Dizziness
Constipation
Confusion
Acceptable combinations in syringe based on laboratory data and clinical practice at recommended doses and concentrations:
3 drugs
Hyoscine hydrobromide +
Diamorphine
+ Levomepromazine or
+ Midazolam or
+ Haloperidol or
+ Cyclizine
2 drugs
Hyoscine hydrobromide +
Diamorphine
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
16
7.10
Drug Recommended Dose Comments
GLYCOPYRRONIUM
Available as: -
200 microgram / 1ml
ampoules
600 microgram / 3ml ampoules
For bronchial secretions:
600 micrograms –
1200 micrograms / 24 hours
Usual starting dose
600 micrograms - reduce if patient frail and/or elderly
For Colic and intestinal obstruction: 600 micrograms– 1200 micrograms / 24 hours
Antimuscarinic drug
Use to dry up noisy respiratory secretions (it may not relieve the noise of existing secretions but is likely to prevent further exacerbation)
Less sedating than Hyoscine
Hydrobromide.
Does not cross the blood brain barrier – therefore is less likely to cause confusion than
Hyoscine Hydrobromide
May also relieve colic
Some anti-emetic action
Side effects
Dry mouth
Constipation,
Transient bradycardia (followed by tachycardia)
Urinary urgency and retention,
Visual disturbances,
Flushing and dryness of the skin.
Nausea, vomiting, and giddiness;
Constipation
Confusion (particularly in the
elderly),
Very rarely, angle-closure
glaucoma
3 drugs
Glycopyrronium + Diamorphine
+ Levomepromazine or
+ Midazolam or
+ Haloperidol or
+ Cyclizine
2 drugs
Glycopyrronium + Diamorphine
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
17
7.11
Drug Recommended Dose Comments
DEXAMETHASONE
(Dexamethasone Sodium
Phosphate)
Available as: -
Dexamethasone
4mg / ml ampoules
8mg / ml vials
4mg – 16mg Dexamethasone
Do not mix with other drugs – use a separate syringe driver
Remember: Dexamethasone has a long half life and can be given as a once or twice daily injection rather than setting up a syringe driver. If administered by this method, do not give after
14.00 as can cause insomnia.
Use 0.9% Sodium Chloride as diluent
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
18
7.12
Drug Recommended Dose Comments
OCTREOTIDE
Available as: -
50 microgram / 1ml ampoules
100 microgram / 1ml ampoules
500 microgram / 1ml ampoules
200 micrograms – 600 micrograms / 24 hours
Starting dose 200 micrograms
NB: Refer to Specialist Palliative Care for advice if maximum dose is not effective.
Stimulates water and electrolyte absorption and inhibits water secretion in bowel
Useful for nausea and copious vomiting associated with intestinal obstruction
Can be used for leaking fistulae, e.g. rectal / vaginal
Use 0.9% Sodium Chloride as diluent
NB: seek advice before mixing with other drugs
Combination data is the best available at the time of publication. Practitioners should ensure that when combinations are in use the syringe and the patient should be monitored closely especially if any of the doses or concentrations are modified.
Concentration dependent combinations are more susceptible to instability when doses or concentrations of drugs are changed and should be closely monitored.
7.13
Drugs not suitable for use in the syringe pump
CHLORPROMAZINE
Can cause skin irritation
PROCHLORPERAZINE
Can cause skin irritation subject to light sensitivity
DIAZEPAM
Can cause skin irritation
N.B
Once the syringe has been primed and the syringe pump infusion commenced, DO NOT add additional drugs to the driver.
If a further symptom presents that requires management using a drug via a syringe pump, a completely new syringe should be primed using a full 24 hour dose of all drugs and the driver recommenced.
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
19
8.0 The T34 McKinley Syringe Pump
8.1
. Information for Patients
A full explanation of the device and the procedure to be undertaken is to be discussed with the patient and their informed consent to the procedure must be obtained and documented.
Syringe pumps should be sited and maintained by nurses that have been assessed as competent who feel confident in their own ability and possess current knowledge and skills in relation to use of a McKinley T34 syringe pump.
All patients who are using a syringe pump and their carers need to be informed of the reasons why the syringe pump is being used. Please refer to the McKinley T34 Syringe Pump Patient Reference
Guide
Where appropriate the nurse should give information about type of medication used, and its common side effects.
Lockable boxes should be used to ensure safe administration for patient.
8.2 Labeling of the syringe in the syringe pump
All Luerlock syringes are to be labeled with patient identifiers name, NHS number, contents, name of drug, strength and dosage to be administered, volume/amount, any diluents or mixes, date, time, of preparation and date and time of expiry and nurses signature, when used for the administration of medication via a syringe pump.
Rationale:
To ensure infusion is clearly labeled.
NMC Standards for Medicines Management (August 2008)
8.3 Calibration of a syringe pump
Syringe Pumps will be calibrated and serviced on an annual basis, unless there is concern about the functioning of the syringe pump when it should be sent immediately to the Medical Physics
Department at Northern Lincolnshire & Goole Hospitals. If at the time of malfunction the syringe pump was in use then an incident form should also be completed in line with the requirements of each organization.
The McKinley T34 syringe pump will display the message “Calibration Due send for service” to inform users that a service is due when the machine is switched on. It should then be returned to
Medical Physics for servicing.
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
20
8.4 Decontamination of the McKinley T34 Syringe pump
Aim
To prevent the syringe pump from becoming a vehicle for cross infection and prevent the transfer of body fluids from one individual to another. To create a detailed log of syringe pump usage to enable an audit trail.
Process
The syringe pump must be decontaminated between individual uses; prior to service, inspection or repair; as part of good housekeeping if contaminated or if it appears visibly dirty during use
(including the main pump screw and guiding rods).
Standard precautions should be used whenever there is a potential risk of exposure to blood, body fluids, secretions and excretions.
All consumables should be disposed of in accordance with the Waste Management Policy and
Strategy. Prior to cleaning the syringe pump, a 1% hypochlorite solution should be used on blood, i.e. Virkon, HAZ-tabs or Sanichlor. This should then be wiped off to protect the equipment.
The syringe pump should be cleaned by wiping the outside with a soft cloth dampened with a diluted mild detergent. The removable outer clear plastic cover should be washed in warm soapy water, rinsed and allowed to dry.
Cleaning with organic solvents, e.g. surgical spirit or abrasive cleaners may damage some of the plastic parts and should therefore not be used.
Warning: Never dip or immerse the syringe pump in any liquid or try to sterilize it with steam or
gas. It is not completely sealed.
A record of each syringe pump should be kept, with a detailed log of when the syringe pump is removed from storage, and by whom; the name of the patient using the equipment, or a reason validating its absence, i.e., service; the date the syringe pump is decontaminated and by what method; and the date the equipment is returned to the store, and by whom.
8.5 Decontamination of the Holster bag
Aim
To prevent the holster from becoming a vehicle for cross infection, and prevent the transfer of body fluids from one individual or another.
Process
The holster bags should be decontaminated between individual uses; as part of good housekeeping. Disposable bags should be used for single patient only and disposed of after use.
Permanent Holsters should be laundered locally as per hospital equipment at 60 degrees Celsius.
Within the Community if no access to NHS laundering services, then holster bags must be disposed of after use.
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
21
9.0 Standard Operational Procedure for setting up a Syringe Pump
It is the responsibility of individual practitioners to ensure that they undertake the specified training to use this piece of equipment and are deemed competent through assessment, knowledge and ongoing training. They must feel confident in their own ability with up to date knowledge and skills because they are accountable for their own practice in line with the NMC
Code of Conduct (2011) Professional Standards for Nurses and Midwives.
ACTION RATIONALE
Discuss the use, storage of drugs and siting of the syringe pump with patient and carer.
Discuss the cleaning requirements of the syringe pump and holster bag.
Check and draw up the prescribed drugs – with the correct diluent.
When using a 20mls syringe draw up to a maximum of 17mls in total.
When using a 30mls syringe draw up to a maximum of 22mls in total.
NOTE: use only 20ml or 30ml LUERLOCK syringes
Patient and carer are informed and are aware of safety issues.
Informed consent received.
Risk of cross infection/contamination reduced.
To prevent instability of drug mixtures
To ensure correct dosage/volume of diluent and prevention of syringe disconnection.
Attach the charged syringe to the winged infusion set or Sof Set
Prime the line.
Label the syringe with contents, date, time, batch number and the nurse’s signature.
Turn on the power. Ensure barrel clamp is down. Self test screen appears on the pump
LCD screen. If servicing is required the message “Calibration due send for service” will be displayed at this time.
To expel air
To ensure infusion is clearly labeled.
To ensure the pump is functioning correctly.
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
22
Use another pump and send one requiring servicing to Medical Physics.
ACTION
Allow pre-loading to complete (actuator moves to the position of the last syringe that was in place, at the start of the previous infusion). Use << FF or Back >> buttons to position actuator for syringe loading if necessary.
Checking the battery –
Always check the battery power before starting the infusion.
Press the INFO key repeatedly until the battery level appears on the screen and then press “Yes” to confirm
Discard the battery if there is less than 40% remaining. The average battery life, starting at 100%, is 3-4 days but depends on usage.
To ensure safety and reliability of pumps.
RATIONALE
Verify that there is sufficient battery power for the programme.
Load syringe – lift and turn barrel clamp arm.
Place syringe into plunger and collar sensor simultaneously (syringe scale facing towards front). Turn and lower the barrel clamp arm to secure the syringe.
The syringe size and brand option will then be displayed, if these match the screen message press “Yes” key to confirm. If the syringe size and/or brand do not match scroll down arrows until the correct selection appears, then press “Yes” key to confirm.
If the correct syringe brand cannot be found on the menu, this may be due to incorrect positioning of the syringe. Remove the syringe and refit ensuring the syringe is fitted securely into all 3 detection points.
The pump calculates and displays the deliverable volume, duration of the infusion
(24hours) and rate of infusion (mls per hour)
To ensure safe fixation of the syringe.
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
23
– Press “YES” to confirm or ON/OFF to return to the syringe options.
Pump Screen prompts “START INFUSION”- do not press “yes” at this time.
Check the line is connected to the pump.
Serious incidents have been reported involving uncontrolled flow of medication when the syringe has not been correctly or securely fitted to syringe pumps.
Select a suitable site for insertion.
In an area of as much subcutaneous fat as possible e.g. Anterior chest wall, top of thigh, upper arms, anterior abdominal wall.
To ensure correct delivery of medication
Ensure comfort of patient wherever possible.
Cleanse the skin at selected site with an alcohol skin wipe and allow to dry (clip hair if necessary). If long term use is anticipated, clean the skin with liquid soap and water and allow drying.
Insert the needle SUBCUTANEOUSLY as per guidelines for giving sets.
45 degree angle for winged infusion set.
90 degree angle for sof set and remove introducer needle.
Secure the needle and line with a vapour permeable adhesive film dressing. Specific IV dressing is preferable if available.
To follow infection control guidelines.
To enable a subcutaneous route for drug administration.
To ensure needle remains in position and the site can be observed.
Complete documentation in patient notes, drug authorization and administration record and the stock record sheet(s).
To adhere to NMC Guidelines for Record
Keeping (2008). To provide an audit trail.
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
24
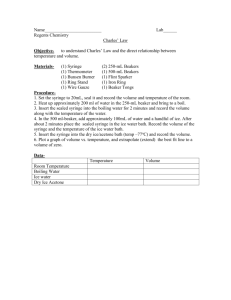
10. SKIN SITE SELECTION AND SKIN CARE
10.1 Skin For Subcutaneous Infusion
The best sites to use for continuous infusion of drugs are: -
(Cooper and Mitten 2000; Danne et al 2000; Dickman et al 2002; Johnson 1998; Macmillan et al
1994)
10.2 Sites Which Should Not Be Used For Cannula Placements Are:
Lymphoedematous limbs. The rate of absorption from the site would be adversely affected and infection could also occur.
Sites over a bony prominence: the amount of subcutaneous tissue would be diminished impairing the rate of drug absorption.
Previously irradiated skin area. Radiotherapy can cause sclerosis of small blood vessels, thus reducing skin perfusion.
Sites near a joint, excessive movement may cause cannula displacement and patient discomfort.
Broken skin.
Localised areas of disease e.g. chest wall with breast cancer.
Affected limb following lymph node dissection.
Patients may decide (in partnership with the nurse responsible for their care) for themselves, after consultation, a suitable site that will interfere as little as possible with their lifestyle (Cooper and
Mitten 2000; Danne et al 2000; Dickman et al 2002; Johnson 1998 )
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
25
10.3 Care Of the Skin Site and Checks
Hospital, Hospice and Nursing Home
Check 4 hourly.
Check position of needle
Condition of site
Volume infused (mls)
Check symptom control
Record above details on syringe driver observation chart
Community
Patient/carer may be taught how to assess if appropriate.
The District Nurse or Community Nurse will check the site at each visit.
Check position of needle
Condition of site
Volume infused (mls)
Check symptom control
Record findings
For all
The cannula should be re-sited when there is evidence of
Inflammation
Poor absorption (a hard subcutaneous swelling).
The time taken for this to occur can vary from hours to weeks dependent on the patient and the drugs being infused. Avoid immediate area for re-siting; relocate to another skin site (Cooper and
Mitten 2000; Danne et al 2000; Dickman et al 2002).
If The Skin Sites Break Down Rapidly, Suggestions Include: -
Further dilute the drug infused by using a larger volume of diluent in a larger syringe.
Change the site regularly (e.g. daily/48 hours or on visual inspection) before it breaks down.
Consider changing to an alternative brand of cannula. E.g. Teflon
Mix drugs with 0.9% Sodium Chloride if compatible
Reconsider alternative drugs and/or routes of administration.
If skin site reaction continues - seek specialist advice as further measures can be taken
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
26
11. TROUBLE SHOOTING CONSIDERATIONS
PROBLEM POSSIBLE CAUSE
Infusion ended early
Incorrect rate setting
Scale length measured incorrectly
Tampering
Infusion ended late Incorrect rate setting
Scale length measured incorrectly
Malfunctioning pump
Infusion stopped Blockage in the line
Battery exhausted
Line kinked
Syringe/tubing disconnected
ACTION
Report as an incident according to trust/organisational policy
Report as an incident according to trust/organisational policy
If infusion has been stopped for greater than one hour, report as an incident according to trust policy
Infusion won’t start Battery inserted incorrectly
Battery exhausted
Start button not depressed sufficiently
Medication crystallises
Alarm – battery is depleted
Incompatibility of drugs or diluent in syringe
Battery needs replacing
Correct as appropriate
STOP - seek urgent medical and pharmaceutical advice. Ensure that the patient is comfortable
Replace battery
Infusion motor running
Light still flashing
Periodic click
Syringe plunger mechanism has worn out
Use another syringe driver
Unit to be returned to Medical
Electronics Department
Syringe pumps should be serviced annually according to organisational policy.
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
27
12. SPECIALIST ADVICE
12.1 CONTACT NUMBERS FOR SPECIALIST PALLIATIVE CARE ADVICE
SITE CONTACT CONTACT NUMBER
St Andrews Hospice
Senior Nurse on duty (01472) 350908
Lindsey Lodge Hospice
Senior Nurse on duty (01724) 270835
Scunthorpe & Goole Hospitals
Macmillan Nurses – Palliative Care (01724) 387709
Diana Princess of Wales Hospital Macmillan Nurses – Palliative Care or
Macmillan End of Life Clinical Care
Co-ordinator
(01472) 874111 Ext 3596 or
(01472) 874111 Ext 3595 or via hospital switchboard
(01472) 250623
North East Lincolnshire
Care Plus Group
Macmillan Nurses – Palliative Care
East Riding Community Health
NHS Trust
Macmillan Nurse – Palliative Care
(Goole only)
(01405) 721314
North Lincolnshire Community
Macmillan Team
Macmillan Nurses – Palliative Care (01724) 871556
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
28
CME Medical
13 REFERENCES
AUTHOR PUBLICATION
DATE
2011
Cooper, J. &
Mitten, T.
Danne et al
David, J
Dickman et al.
2000
2000
1992
2005
2006
TITLE
T34 Ambulatory Syringe pump. Device Use and Training
Resource
Continuous Subcutaneous Infusions
Chapter 3, P 56 In (Ed.) Cooper, J. Stepping Into Palliative
Care. A Handbook For Community Professionals. Radcliffe
Medical Press.
An Audit Of Subcutaneous Syringe Drivers In A Non-
Specialist Hospital
International Journal Of Palliative Nursing. 6, No. 5
A Survey Of The Use Of The Syringe Drivers In Marie Curie
Centres
European Journal Of Cancer Care. 4 P 23 - 28
The Syringe Driver – Continuous Subcutaneous Infusion In
Palliative Care
Oxford University Press
Duties of a Registered Doctor General
Medical
Council
Johnson, J. 1998
Macmillan et al 1994
The Syringe Driver
In (Ed.) Faull, C., Carter, Y., And Woof, R., Handbook Of
Palliative Care. Blackwell Science
A Prospective Comparison Study Between A Butterfly And
A Teflon Cannulae For Subcutaneous Narcotic
Administration
Journal Of Pain And Symptom Management. 9, P 82 - 84
Mitten, T. 2001
2008
Subcutaneous Drug Infusions: A Review Of Problems And
Solutions
International Journal Of Palliative Nursing. 17 No 2
Code of Professional Conduct Nursing &
Midwifery
Council
Nursing &
Midwifery
Council
Northern
Lincolnshire
And Goole
Hospitals NHS
Trust
2008
2006
Guidelines For The Administration Of Medicines
NMC
The Medicines Code
A Guide To The Use Of Medicines In Northern Lincolnshire
& Goole Hospitals NHS Trust
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
29
Ross, J. R. 2002
A Prospective, Within Patient Comparisons Between
Butterfly Needs And Teflon Cannulae In Subcutaneous
Infusions Of Drugs To Terminally Ill Hospital Patients
Journal Of Pain And Symptom Management. 16, P 15 - 16
Trissel, L 2003
Handbook On Injectable Drugs
12 th Edition. American Society Of Health System
Pharmacists
Twycross, R. et al
2002
Symptom Management In Advanced Cancer
Twycross et al 2011
3rd Ed. Chapter 2, P 42. Radcliffe Medical Press
The Palliative Care Formulary 4 th Edition, Radcliffe
Medical Press
ORIGINAL AUTHORS
Bealey, Muriel
Chester, Janet
Dyer, Chris
Foster, Liz
Henry, Christine
Head of Adult Services, St Andrew’s Hospice, Grimsby
Macmillan Palliative Care Nurse Specialist, N. Lincs PCT
Senior Nurse, Lindsey Lodge Hospice, Scunthorpe
Macmillan Palliative Care Nurse Specialist, NE Lincs PCT
Macmillan Palliative Care Nurse Specialist, Scunthorpe Hospital
Maloney, Lindsay Macmillan Palliative Care Nurse Specialist, NE Lincs PCT
Morris, Ann Macmillan Lead GP, N. Lincs PCT & Medical Director, Lindsey Lodge
Hospice
Prucyck, Julie
Purser, Paul
Revill, Val
Rose, Ann
Macmillan Palliative Care Nurse Specialist, Scunthorpe Hospital
Macmillan Lead GP, NE. Lincs PCT & Medical Director, St Andrew’s Hospice
Macmillan Lead Nurse for Palliative Care, NE Lincs PCT
Clinical district Nurse Lead, N. Lincs PCT
Smith, Elaine Palliative Care Support Nurse, Scunthorpe Hospital
Staniforth, Rachel Pharmaceutical Advisor, NE Lincs PCT
Turner, Martyn
Walker, Helen
Chief Pharmacist, NL&G
Medicine Information Pharmacist, NL&G
Watson, Sally
Wilkinson, Su
Macmillan Palliative Care Nurse Specialist, NE Lincs PCT
Clinical Documentation Project Manager, NL&G
Procedure for the use of the McKinley T34 syringe pump in palliative and end of life care
February 2013
30