Chest Trauma
advertisement

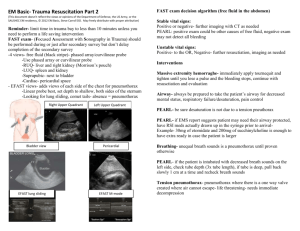
Chest Trauma Chest Trauma - BLUNT Chest Trauma - PENETRATING Chest Trauma - INCIDENCE Sudden and dramatic Directly => 20 – 25% (1 in every 4) trauma deaths Contribute to 25-50% of the remaining deaths => 16,000 deaths per year in USA Chest Trauma - CARE Improved pre-hospital & peri-operative care => More pts getting to ER alive Many die after coming to hospital Deaths possibly preventable => by prompt Dx and Tx Chest Trauma - HISTORY 3000 BC – treating gladiators chest injuries 1635 - De Vacca => removal of arrowhead from chest wall 1814 -Larrey reported injuries to subclavian vessels 1902 - Hill performed first cardiorrhaphy in US 1934 - Blalock first American to successfully repair an aortic injury BOUNDARIES of Chest Superiorly => clavicles Inferiorly => diaphragm Laterally => rib cage BOUNDARIES of Chest Anteriorly => sternum Posteriorly => vertebral bodies & ribs STRUCTURES Injured Any organ in chest potentially susceptible – especially to penetrating trauma CONTENTS - Thoracic cavity - Chest wall and ribs - Lungs and pleura - Great and thoracic vessels - Heart and mediastinal structures - Diaphragm CONTENTS - Thoracic cavity Esophagus Thoracic duct Tracheobronchial system OTHER ORGANS at risk Thoraco-abdominal injury any wound below nipples in front and inferior scapula angles dorsally may result in intra abdominal injury OTHER ORGANS at risk Peritoneal viscera – – – – – Liver Spleen Stomach Colon & small intest. Biliary system Retro-peritoneum kidneys RESULTING INJURIES – Rib fractures – Sternal fractures – Open or Closed Pneumothorax - unilateral / bilateral – Hemothorax – Hemopneumothorax RESULTING INJURIES – Pneumo-mediastinum – Pulmonary contusion – Myocardial contusion – Diaphragmatic rupture RESULTING INJURIES Subcutaneous emphysema CLINICAL CONSEQUENCIES RELATED TO : Mechanism of injury – Location of injury – Associated injuries – Co-morbidities Mechanism of Injury BLUNT Mostly managed non-operatively – Simple intubation & ventilation or – chest tube placement Mechanism of Injury PENETRATING Low energy Medium energy High energy Penetrating (Low energy) Impalements Knife wounds => disrupts only structures penetrated Penetrating (Medium energy) Bullet wounds from most handguns => primary tissue damage < than higher velocity forces Penetrating (High energy) From rifles and military weapons + Shotguns (low velocity) Transfers kinetic energy to tissues => cavitation => high velocity. Amount of tissue damage proportional to amount of energy exchanged between the penetrating object and the body part. Pathophysiology Quite serious 1. HYPOXIA / HYPO-VENTILATION Primary acute killer of trauma patients inadequate delivery of O2 to tissues Signs of HYPOXIA Increased RR Change in breathing pattern (shallow) Anxious behavior Poor air movement Diaphoresis Dilated pupils Cyanosis – (late sign) 2. Hypovolemia Inadequate intravascular volume => BLOOD LOSS 3. Ventilation / Perfusion Mismatch Contusion Hematoma Alveolar collapse 4. CHANGES IN INTRATHORACIC PRESSURE RELATIONSHIPS - Tension pneumothorax - Open pneumothorax 5. METABOLIC ACIDOSIS Hypo perfusion of tissues (shock) MANAGEMENT - Chest Trauma ABCs PRIMARY SURVEY – Most important feature of chest injury evaluation => Aim to identify & treat immediately life threatening conditions MANAGEMENT - Chest Trauma EARLY INTERVENTIONS geared towards – identifying / correcting / preventing problems Tension pneumothorax Massive hemothorax Open pneumothorax Cardiac tamponade Flail chest MANAGEMENT - Chest Trauma Resuscitation of vital functions REMEMBER : - Most life threatening injuries txd by - Airway control - Chest tube MANAGEMENT - Chest Trauma - Detailed Secondary Survey Influenced by: Mechanism of injury High level of suspicion May show: Simple pneumothorax Hemothorax Pulmonary contusion Myocardial contusion Blunt aortic injury Rib fractures Diaphragmatic rupture MANAGEMENT - Chest Trauma Definitive care Usually operative MANAGEMENT - Chest Trauma Adjuncts CXR => basis for initiating other investigations ALL wounds to thoracic cavity bounded back & front by Neck & umbilicus for stabs Neck & pelvis for GSW – MUST HAVE CXR => UPRIGHT if possible Adjuncts - FAST Focused Abdominal Sonography for Trauma (FAST) - All hemodynamically unstable blunt trauma pts Adjuncts - Cat Scan - (CT angio) Becoming a primary diagnostic tool fast (spiral) allow for reconstruction etc SPECIFIC CHEST INJURIES Chest Wall Rib fractures Most common sign of blunt chest injury – Fx scapula, first rib, sternum suggest massive force of injury – 1st & 2nd rib fx associated with serious other injuries – Upper ones => suspect vascular injury Rib Fractures Rib fractures Signs and Symptoms - Deformity - Localized pain - Tenderness - Crepitus Rib Fractures Treatment Analgesia (PCA) Pulmonary toilet Observe for possible pneumothorax Flail Chest Segment of chest wall that does not have continuity with rest of thoracic cage Usually 2 fractures per rib in at least 2 ribs Segment does not contribute to lung expansion Disrupts normal pulmonary mechanics Accompanied by pulmonary contusion in 50% of patients with flail chest Flail Chest - Pathophysiology A major problem is the injury to the underlying lung => Pulmonary Contusion Flail Chest – Signs & Symptoms Dyspnea Chest pain Paradoxical chest wall movement Poor air movement Crepitus Hypoxia Cyanosis Flail Chest - Treatment Pain control Humidified O2 Close observation for respiratory decompensation Aggressive pulmonary & physical therapy Flail Chest - Treatment Selective intubation and ventilation: significant other injuries respiratory rate > 35 paO2 < 80 paCO2 > 66 Other treatments: tight fluid resuscitation Flail Chest - Treatment Operative fixation not usually required (historical) Lung Injuries Pneumothorax or Hemothorax – most treated with simple tube thoracostomy Pneumothorax Less than 1-2 cm may be observed in otherwise healthy pts if stable on f/u CXR 6-8 hrs after Open Pneumothorax Open sucking chest wound if opening 2/3 of diameter of trachea air will come through wound (preferentially) allows free passage of air into and out pleural cavity => effective ventilation impaired => hypoxia & hypercarbia Open Pneumothorax Signs & Symptoms Penetrating chest wound Decreased breath sounds Sucking sounds on inspiration Open Pneumothorax Treatment : 3 sided occlusive dressing Observe for tension pneumothorax Operative Tension Pneumothorax One way valve allows air leak from lung or chest wall => air forced into chest cavity without escape Tension Pneumothorax Collapses ipsilateral lung Tension Pneumothorax Displaces mediastinum to opposite side Tension Pneumothorax Compresses opposite lung Tension Pneumothorax Decreases venous return Tension Pneumothorax Signs & Symptoms – – – – – – – – – air hunger chest pain respiratory distress tachycardia hypotension tracheal deviation absent breath sounds hyper-resonant percussion JVD Tension Pneumothorax - Treatment Immediate decompression – large bore needle 2nd intercostal space midclavicular line – chest tube as definitive tx NOTE – may mimic a collapsed lung on the other side – - i.e. trachea deviates towards the collapsed lung – - however, one resonant (empty), other tympanic (full) Pulmonary Contusion Largest # of pts are those with blunt trauma Most common chest injury in children Usually develops over 24 hours Can occur with or without laceration of parenchyma Pulmonary Contusion Results from: Leakage of blood and fluid into interstitial spaces of lung - Significant inflammatory reaction to blood components in the lung Pulmonary Contusion - Pathophysiology Loss of normal lung structure & function leads to - poor gas exchange - increased pulmonary vascular resistance - decreased lung compliance Pulmonary Contusion - Complications – – – – Atelectasis Pneumonia ARDS Respiratory failure Pulmonary Contusion - Diagnosis Parenchymal infiltrate seen in CXR adjacent to injured chest wall Pulmonary Contusion - Diagnosis No real clinical findings especially initially dyspnea chest wall contusions / abrasions increased RR may have crackles Pulmonary Contusion - Diagnosis Lung gets stiffer causing dyspnea and increased RR Blood gases worsen 2-3 days as edema increases CXR changes may lag 12 48hrs behind May underestimate the true extent CT - very sensitive – can allow quantifying Pulmonary Contusion - Treatment MOSTLY supportive - usually resolve in 5-8 days O2 + observation in milder cases - Pain control to allow: - adequate ventilation and better management of secretions - Fluid restriction - Intubation + mechanical ventilation if respiratory distress present - Pulmonary Contusion Indications for intubation Respiratory distress Co-morbidities esp. lung disease Other injuries – intra-abdominal Myocardial contusion Physical bruising of the cardiac muscle Usually associated with fractures of the sternum Any severe anterior chest injury Myocardial contusion Difficult to dx => HIGH LEVEL OF SUSPICION ALL pts with pattern of injury must have an EKG Myocardial contusion - Diagnosis Ectopy ST elevation Tachycardia Friction rub Enzymes may be normal Myocardial contusion - Treatment Monitor in ICU & treat dysrhythmias Serial enzymes Analgesia Massive Hemothorax Pleural cavity hold 3 liters blood 200cc – 1L in chest cavity seen on CXR 90% from internal mammary or intercostals 10% from pulmonary vessels Massive Hemothorax - Treatment – Decompression – Chest tube (most need just that) – Bleeding may stop when lung re-expands Aortic Rupture / Great Vessel Injuries Abrupt deceleration or compression injury Sudden motion of heart / great vessels within thorax Great vessel injury may occur in 0.3 => 10% penetrating trauma Often rapidly fatal Only 10% survive to hospital Only 20% survive > 1 hour 90% who reach hospital will die EARLY DX and aggressive tx best chance Aortic Rupture - Signs and Symptoms – Hypovolemic shock – Chest wall ecchymosis – Marked difference in BP b/l arms – Fx 1st, 2nd, 3rd ribs especially on left Aortic Rupture - Diagnosis Consider mechanism of injury – widened mediastinum on CXR – 40% normalizes with sitting up Aortic Rupture - Diagnosis Mediastinum > 8cm wide Blurring of aortic knob Aortic Rupture - Diagnosis Deviation of NGT to right Aortic Rupture - Diagnosis CT with contrast then angiogram if abnormal Aortic Rupture - Treatment Contained injury => BP control Operative repair Cardiac Injury Highly lethal : fatality rates - 70 => 80% Mostly ventricular – right > left Cardiac Tamponade => Blood in pericardial sac Occurs most frequently with penetrating injuries Cardiac Tamponade - Signs and Symptoms Shock JVD Dyspnea PEA Beck’s triad = minority of pts - Distended neck veins - Muffled heart sounds - Hypotension Cardiac Tamponade - Treatment Volume resuscitation Pericardiocentesis Surgery - Pericardial window - sternotomy - thoracotomy Diaphragmatic Rupture Traumatic herniation of abdominal contents into the chest Diaphragmatic Rupture Mostly on left side Diaphragmatic Rupture Liver “protective” on right side Diaphragmatic Rupture Frequent in thoracoabdominal trauma – 15% stab wounds – 46% GSW – 15% greater than 2cm long May be no immediate herniation of abdominal contents Diaphragmatic Rupture - Signs and symptoms No distinctive signs / symptoms seen High index of suspicion needed especially with mechanism of injury dyspnea cyanosis shoulder pain bowel sounds in lower chest Diaphragmatic Rupture - Treatment Up to 13% acute injuries missed initially 85% presenting in 3 years as - obstruction or with - decreased cardio / pulmonary reserve Goal of treatment: - Maintain adequate oxygenation => intubate - NG decompression of stomach Diaphragmatic Rupture - Surgery Esophageal Injuries Most due to penetrating trauma Diagnosis - Difficult If delayed => rapid sepsis & high mortality Requires aggressive investigation Radiography Endoscopy Thoracoscopy Treatment - Thoracotomy, etc. Thoracic Duct Injuries Accompany thoracic vessel injuries Noted much later i.e. not in acute phase Huge morbidity due to severe nutritional depletion Mn – => initially aggressive and nonoperative = hyperalimentation => TPN and if not sealed in 5-7 days – surgical intervention Emergency Thoracotomies “ACUTE” THORACOTOMY Cardiac tamponade (relieved) Vascular injury to thoracic outlet Massive air leak Endoscopic/radiographic evidence of tracheal or bronchial injury Esophageal injury Chest tube output – immediate evacuation of 1500ml blood – or > 250cc/ hour – TREND MORE IMPORTANT than initial output “ER” THORACOTOMY – survival rates < 8% “ER” THORACOTOMY - To do or NOT to do… Type of CARDIAC ACTIVITY asystole bradycardia tachycardia “ER” THORACOTOMY - To do or NOT to do… Type of VITAL SIGNS electrical cardiac activity (PEA) palpable pulse recordable blood pressure “ER” THORACOTOMY - To do or NOT to do… LOCATION of LOSS of vital signs street in transit ambulance/helicopter unloading area hallway resuscitation area “ER” THORACOTOMY - Unlikely to benefit if ... BLUNT injury with arrest Arriving without pulse/BP Penetrating injury with arrest Better chance High likelihood of – isolated / correctable intra-thoracic injury (?GSW?) – still EXTREMELY RARE “ER” THORACOTOMY - Bottom line ER THORACOTOMY if presence of MEASUREABLE – pulse – blood pressure – organized cardiac activity (or just lost IN trauma bay) MUST consider also – age – co-morbidities (ie infectious diseases) AVOID if arrest – occurs OUTSIDE OF RESUSCITATION AREA or – due to BLUNT trauma. “ER” THORACOTOMY - Consider . . . Be mindful that circulatory arrest => cerebral hypoxia => permanent neurologic deficits => non-functional survivor occurs in 10 => 15% of survivors Chest tube insertion Most common intervention Relatively simple procedure Definitively manage > 85% of chest trauma : penetrating or blunt Has significant complication rate 219% May be minor but May require operative intervention and Can result in death Chest tube insertion - Indications Drain contents of pleural space – – – – air blood chyle gastric contents Prevent development of pleural collection i.e. after thoracotomy Prevent tension pneumothorax in ventilated pt with rib fractures Chest tube insertion - Indications Absolute indications Relative indications – rib fractures and pneumothorax positive pressure hemothorax ventilation traumatic – profound arrest - (b/l) hypoxia/hypotension with penetrating chest injury Placement may be diagnostic or therapeutic Bright red blood – suggest arterial injury = possible thoracotomy Intestinal contents esophageal, stomach, diaphragm intestinal injury Large air leak - bronchial disruption Technique = important to avoid complications Chest tube insertion - Insertion Site mid or anterior axillary line behind pectoralis major above 5th rib since on expiration diaphragm rises that high count down from sternomanubrial joint (2nd rib) Chest tube insertion - Analgesia Painful especially in muscular pts – Morpine IV or Ketamine 20mg in adult – 10-20 ml local analgesia along line of incision perpendicularly thru all layers of chest wall to rib below space up into pleural cavity after aspirating air Chest tube insertion - Procedure Prep and drape Incise along upper border of the rib below the intercostal space to be used Track is to be directed over top of lower rib so as to avoid intercostal vessels lying below each rib should be big enough to fit finger Use curved clamp to develop tract by blunt dissection only – use to spread the muscle fibers, develop tract with fingers On reaching rib, clamp angled upward just above the rib and dissection continued till pleural space entered Chest tube insertion - Procedure Finger inserted into pleural space and area palpated 32-36 F tube attached to clamp and inserted along track into the pleural cavity Chest tube insertion - Procedure Connect tube to underwater seal and suture in place Examine chest to check effect CXR to check placement and position POSITION - Dependent on direction of tract Blunt chest trauma pts lying flat – place drain anteriorly – prevents blockage of tube and development of tension pneumothorax Penetrating Posteriorly & basally directed drain Last hole should be INSIDE the CHEST CAVITY If too far in could cause severe intractable pain when up against mediastinum Chest tube insertion - Underwater Seal Allows air to ESCAPE but NOT RE-ENTER chest cavity Negative pressure dependent upon level of water Pleurovac must always be below level of patient Persistent bubbling = air leak from lung Chest tube insertion - Underwater Seal May be connected to suction (water level 20cm H2O) Aid lung re-expansion especially if there is an air leak CHEST TUBES SHOULD NEVER BE CLAMPED = TENSION PNEUMOTHORAX Chest Tube Removal When? When no air leak No more fluid draining How? Occlude hole while pulling tube Remove at end of expiration or at peak of inspiration Avoids air being drawn into cavity Remove rapidly and close wound quickly Chest tube insertion - Complications “there is no organ in the thoracic or abdominal cavity that has not been pierced by a chest drain” mainly historical since drains used to be inserted with - a steel trocar - excessive force Chest tube insertion - Acute complications Hemothorax – usually laceration of intercostals vessel, may require thoracotomy Tube placed subcutaneously – not in pleural cavity Lung laceration especially when adhesions present Tube placed too far = pain Diaphragm / abdominal cavity penetration placed too low Stomach colon injury diaphragmatic hernia not recognized Tube falls out = not secured properly Chest tube insertion - Late complications – blocked tube = clot, lung – retained hemothorax – empyema – pneumothorax after removal = poor technique Chest Trauma - Conclusion Chest trauma is – COMMON – SERIOUS AIM in TREATMENT – to provide oxygen to vital organs – Be alert to changes in clinical condition Managed MOST of the time with a CHEST TUBE CHEST TRAUMA END