90 Membrane Potential (mV)
advertisement
")
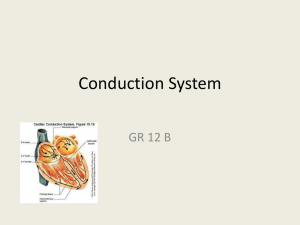
Pharmacology 4 Dr. Khalil Makki Antiarrhythmic Drugs Arrhythmias • Abnormalities in impulse formation and conduction in the myocardium. They are common: • MI(80%), anesthesia(50%),Digitalis(25%). • should be treated if cause poor circulation or threatened to do so. • All antiarrhythmic drugs are pro-arrhythmic in some circumstances. • Electrical tt of arrhythmia is becoming more commonly used. • AF is the most common type, with high risk of stroke, AC TT is essential. Types of Cardiac tissues • i.Ordinary myocardial muscle – contraction and pumping action. • ii.Specialized conducting tissue – cardiac impulse initiation and determines the order in which the muscle cells contract. • Automaticity: the capacity of cells to initiate an impulse without an external stimulus – a feature of certain parts of conducting tissue as SAN, AVN & His – purkinje system. • These pacemaker cells show slow, spontaneous depolarization during diastole Phase 4, (Ca & Na inflow). Classification of Arrhythmia • According to: site of origin of abnormality: Atrial, Junctional or Ventricular. Rate: Tachicardia or bradicardia. Their diagnosis depends on surface ECG. Precipitating Factors • Ischemia, Hypoxia, Acid base and Electrolytes disturbancies. • Autonomic effects. • Drug toxicities as digitalis and even antiarrhythmic drugs. • Overstretching of cardiac fibers or presence of scarred or diseased tissues. • However all arrhythmias result from disturbance in impulse formation and/or conduction. Re-entry Phenomenum • Normal conduction: the impulse dies out after activation of the myocardium(?). It is surrounded by refractory tissues. • Re-entry : the impulse re-excites regions of the myocardium after the refractory period has subsided, causing continuous circulation of APs. • It can result from myocardial damage(IHD) or congenital anamolies. • It is a common cause of many types of arrhytmias. Classification of Antiarrhythmic Drugs Vaughan-Williams Classification(1970) Class Mechanism Example Ia Ib Ic II Na channel blockers Intermediate dissociation fast dissociation Slow dissociation Beta Blockers Disoperamide Lidocaine Flecanide Propranolol III K channel blockers IV Ca channel blockers Other Digoxin, Adenosine,CaCl, V MgCl,Atropine,Epinephrine Amiodarone & Sotalol Verapamil &Isoprenaline Class I Drugs,Na-blockers(memb. Stabilizing) • Slow phase 0 depolarization, prolong AP and slow conduction. • They produce Use dependent channel block i.e. They bind strongly to the open and refractory channels and less strongly to the resting channels. This means, the more frequently the channels are activated, the greater the degree of block produced. • They block the high frequency excitation of the myocardium with out preventing the heart from beating at normal frequency. Clinical Uses and ADRs • Ia, Disopyramide (oral): VA, prevention of recurrent paroxysmal AF. Has atropine like effects. • Ib, Lidocaine (IV): tt and prevention of VT &VF during or after MI. CNS ADRs and convulsion. • Ic, Flecainide (oral):prevention of paroxysmal AF and recurrent tachyarrhythmia. can produce life threatening resistant VT. Class II drugs • β- Blockers: Propranolol, Timolol, Atenolol • Inhibit phase 4 depolarization i.e. the pace maker potential Inhibiting automaticty and prolonging AV conduction & decreasing the HR and contractility. • Clinical uses and ADRs: 1. Reduce mortality after MI. 2. Prevent recurrence of tachyarrhythmias as paroxysmal AF provoked by sympathetic over activity. β- Blockers ADRs • • • • • Increase bronchospasm – asthma. - ve inotropic effect. Bradycardia and fatigue. Sexual dysfunction. Cold extrimities. Class III Drugs • Block K channels, decreasing K out flow during repolarization (phase 3). • Prolong the duration of AP and the ERP. • Amiodarone: contains I2 ,has a dominant class III effect and minor I,II and IV effects • Also has antianginal effect. • Sotalol: Class III effect and non selective β- Blocker. Clinical Uses and ADRs • Amiodarone : In many SV & V tachyarrhythmias ,which are severe and refractory. • ADRs: GIT upset , pulmonary fibrosis, tremor, ataxia, diziness, hypo and hyper thyroidism, photosensitivity , hepatotoxicity and blue skin discoloration. • Satolol: Paroxysmal SVT & V T and V ectopics. • ADRs: very low ,may prolong QT. Class IV Drugs • Ca channel blockers: • Verapamil and Diltiazem, oral. • Slow phase 2 “plateau” ,slow conduction and prolonging ERP. • They show use dependent block. • Used to:1. Prevent recurrence of paroxysmal SVT and 2. Reduce ventricular rate in pts with AF and flutter. 3. Hypertension and angina. Adenosine • Naturally occurring nucleoside. • At high doses: a. Decreases conduction velocity. b. Prolongs RP. c. Decreases the automaticity in AV node Adenosine • Very rapid onset of action . • Short half- life (seconds) • Given as a rapid I.V. bolus injection For the acute termination of re-entrant supraventricular tachycardia ( paroxysmal attack) First choice. ADRs and #s • • • • • • Bronchospasm, Chest pain. Shortness of breath. Flushing of the face. A-V block. Hypotension. #s :Bronchial asthma and A-V block Others Mg Cl2: Used in:Digitalis induced arrhythmias and Sinus tachycardia KCl: Digitalis induced arrhythmias. Ca Cl2 :Ventricular tachycardia due to hyperkalemia. Atropine: Sinus bradycardia. Epinephrine : Cardiac arrest. Isoprenaline: Heart block.





![Applied Heat Transfer [Opens in New Window]](http://s3.studylib.net/store/data/008526779_1-b12564ed87263f3384d65f395321d919-300x300.png)