Pulmonary Function Studies Review
advertisement

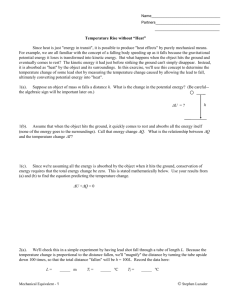
Pulmonary Function Studies: Review By Elizabeth Kelley Buzbee AAS, RRTNPS, RCP Lone Star college Systems- Kingwood • Identify the indications for PFT answer • according to the AARC CPG, PFT need to be done to: [1] diagnosis restrictive defects, [2] to differentiate between restrictive and obstructive defects, [3] assess the patient’s response to interventions [4] pre-op assessment of patients at risk for pulmonary limitations [5] evaluate pulmonary disability [6] Quantify air trapping; is it getting worse, better • What are the hazards of PFT? answer • According to the AARC CPG, the relative contraindications include • [1] untreated pneumothorax • [2] hemoptysis • [3] unstable hemodynamics • [4] aneurysms. – If persons have claustrophobia, upper body paralysis or cast that makes the ‘body box’ impossible, this single test may be deferred. • Identify this type of pulmonary function study answer • This is a flow volume loop used to find both obstructive and restrictive defects. • The shape of the curve can give the RCP information about where an obstruction is located: intra-thoracic large airway, large fixed or small airways • • Read the FVC of the blue tracing and compare it to the normal one answer • The FVC of the blue tracing on the flow volume loop is 200 ml [the line starts at 100 so we need to subtract that from the end point] • The FVC of the normal flow volume loop is 600 ml. • The percent of predicted is 200/600 or 33% of predicted • There is very severe derangement of the FVC values • Is the blue tracing consistent with a restrictive defect or an obstructive defect? answer • The blue tracing is 33% of predicted which demonstrates a very severe restrictive defect. • Identify the peak inspiratory flow rate of the blue tracing • Identify the peak expiratory flow rate of the blue tracing answer • the peak inspiratory flow rate of the blue tracing is about 65 LPM • The peak expiratory flow rate is also about 65 LPM • Compare the blue tracing of the PIFR to the normal one • Compare the blue tracing of the PEFR to the normal one answer • PIFR is about 80 LPM so 65/80 = 81% predicted or normal • PEFR is about 100 LPM so 65/100 is 65% of predicted which is consistent with mild airway obstruction • Discuss the clinical significance of VT that is 50% of predicted. answer • A VT by itself is not too helpful; we could have a restrictive defect or an obstructive one. • The most use we get out of this value is during weaning parameters. • Discuss the clinical significance of a FEV1 that is 45% of predicted answer • A FEV1 that is 45% of predicted implies that there is a severe obstructive defect, but we need to see the FVC also • If both are down, we may have restrictive defect • If FVC is ok, but there is a lower FEV1 then it is clear we have obstruction • Calculate the FEV1/FVC. A normal person should be able to exhale 70% of his FVC in the first second • • Discuss the clinical significance of a FEV1/FVC that is higher than normal. answer • The person with a FEV1/ FVC that is high may have a normal exhaled flow, but have a low FVC due to a restrictive defect. • Discuss the clinical significance of an elevated FRC. answer • High FRC implies that there is air trapping which is associated with obstructive defects • Discuss the clinical significance of a TLC that is 135% of predicted answer • TLC that is elevated shows significant hyperinflation if the FRC is also higher than normal • If a person’s RV is increased what problems does this imply? answer • An elevated RV implies that there is airtrapping associated with obstructive defects such as asthma, COPD or emphysema • How do we ask a patient to perform the flow volume loop? answer • We ask him to perform a FVC into the computer which will display the graphics • We ask him to inhale as deeply as possible from the end expiratory of a normal breath then exhale as completely and as quickly as possible • What is the function of the MVV? answer • The MVV is used to monitor the ability of a patient to maintain rapid and deep breaths over a period of time • The person with significant obstruction cannot do this because he will start to air trap • The person with restrictive defect will have problems getting a big enough VT with each breath---the most important diagnostic benefit of looking at the MVV is assessing the patient for his ability to tolerate pulmonary rehabilitation • How do we measure a value like the RV that cannot leave the body? answer • To collect the value of the RC which is needed to calculate the FRC, we need to measure this volume indirectly by helium dilution studies or by N2 washout [over several minutes] • What is the function of the single breath N2 washout study answer • In the single-breath N2 washout study we are looking at gas distribution which is directly related to the level of airway obstruction • What is the significance of having a higher TGV by body box than TLC by helium dilution answer • If the body box results in a higher volume than the helium dilution, it is because there are airways that have not been exposed to the other airway—they are completely obstructed • What circumstances can result in decreased diffusion of Carbon monoxide during diffusion studies? answer • Any disorder that results in hypoxemia can result in diffusion defect. • If there are no s/s of restrictive or obstructive defects on PFT, but there is diffusion, we worry about disorders such as pulmonary emboli. Case study # 1 • Your patient is a 45 YO Asian male who presents with episodes of SOB associated with weather changes and increased activity. • He is tested in the Pulmonary function lab: • you see the following: FVC - 63% predicted Slow VC - 88% predicted What does this imply? answer • If the slow VC is higher than the forced VC, we may have an obstructive defect without a restrictive componant • He also has this: – IC – 89% predicted – FRC- 136% predicted – PEFR – 65% predicted – PIFR 91% predicted answer – IC – 89% predicted- this is WNL and shows that there is no restrictive defect – FRC- 136% predicted- this shows that there is no restrictive defect. But that there is obstructive defect associated with air trapping – PEFR – 65% predicted- the peak flow is decreased showing mild obstructive defect – PIFR 91% predicted is WNL; there is no upper airway obstruction • • • • • He has the following data: FEV1 62% predicted FEV1/FVC 67% predicted FEV 25-75% 65% predicted MVV – 54% of predicted answer • FEV1 62% predicted: implies that there is moderate obstructive defect • FEV1/FVC 67% predicted: supports this obstructive defect • FEV 25-75% 65% predicted- mild obstruction in the smaller airway • MVV – 54% of predicted: shows that this patient would have poor exercise tolerance, but could undergo pulmonary rehab • What is your overall impression of this patient? answer • This patient has several indices for mildmoderate obstructive defect with air trapping • This patient has no evidence of restrictive defect Case study #2 • Your patient is a 58 YO LAF who presents with the following s/s: She is in considerable respiratory distress at rest with RR 25 BPM, HR 109 with sinus tachycardia. Systemic BP is 156/99. She is afebrile at this time, but has recurrent pneumonias over the last few years. On 12-lead EKG we see right axis deviation. • • • • • She has the following PFT: FVC - 49% predicted Slow VC - 49% predicted IC – 50% predicted FRC- 45% predicted answer • FVC - 49% predicted: implies there is might be a severe restrictive or obstructive defect • Slow VC - 49% predicted: supports a severe restrictive defect • IC – 50% predicted: implies moderate restrictive defect • FRC- 45% predicted: implies there is severe restrictive defect answer • The patient has the following parameters on PFT: • PEFR – 88% predicted before and after BD: no obstructive defect • PIFR 95% predicted no obstructive defect • FEV1 120% predicted: WNL no obstructive defect • FEV1/FVC 145% predicted: implies there is restrictive defect • FEV 25-75% 98% predicted: no obstruction in the small airways • MVV – unable to complete • What is your overall impression of this patient? answer • This patient has moderate-severe restrictive defect with no obstruction