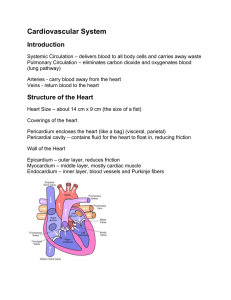
The Cardiovascular System: Blood Vessels and Circulation
advertisement

The Cardiovascular System: Blood Chapter 14 Function • Transportation-hormones, gasses, nutrients, ions, heat • Regulation- pH, temperature, water balance in cells • Protection- clotting, white cells interferons, complement Composition • • • • Connective tissue-Two parts Plasma = soluble materials (~55%) Formed Elements = cells (~45%) Percent occupied by red blood cells (RBC) = hematocrit (Hct) • White blood cells (WBC) ~1% Figure 14.1a Figure 14.1b Plasma • • • • • ~91% water, 7% proteins, 1.5 % other solutes Proteins: Albumin (54%)- osmosis and carriers; Globulins (38%)- antibodies Fibrinogen (7%)- clotting Other: Electrolytes , nutrients, gases, hormones, vitamins & waste products Formed Elements I. Red Blood Cells II. White blood cells – A. granular Leukocytes 1. Neutrophils 2. Eosinophils 3. Basophils – B. Agranular leukocytes 1. T & B lymphocytes & natural Killer cells 2. monocytes III Platelets Formation of Blood Cells • Called hemopoiesis • Just before birth and throughout life occurs in red bone marrow • Contains pluripotent stem cells • In response to specific hormones these develop through a series of changes to form all of the blood cells Figure 14.2a Figure 14.2b Erythrocytes (RBCs) • Hemoglobin package- carries oxygen – Also carries some CO2 • Male has ~ 5.4 million cells/µl; Female has ~4.8 million • membrane, no nucleus, flexible structure • use glucose for ATP production to maintain ionic composition – No mitochondria • Wear out fast- live ~120 days RBC Cycling • cleared by macrophages (liver & Spleen) • Fe- recycled in bone marrow – Carried in blood on transferrin • Heme bilirubin and excreted (bile) • Globin A.A. recycled. Figure 14.3 RBC Synthesis • called erythropoiesis • From stem cells: hemocytoblasts • Released as reticulocytes – Mature to erythrocytes in 1-2 days • • • • Production & destruction is balanced Low O2 delivery (hypoxia) erythropoietin release (EPO) from kidney Stimulates erythropoiesis Figure 14.4 White Blood Cells • Defenses: phagocytes, antibody production and antibacterial action • Phagocytes: – Neutrophil- first responders – Monocytes macrophages (big eaters) – Eosinophil- phagocitize antibody-antigen complexes Involved in suppressing allergic responses – Basophil- intensify allergic reactions • Immune response: – T-cells, B-cells& natural killer (NK) cells WBC Life Span • • • • • 5000-10,00 WBC /µl blood Limited number of bacteria can be eaten Life span is a few days During active infection may be hours Leukocytosis= increased WBC numbers response to stresses • Leukopenia = decreased WBC numbers Platelets • Myeloid stem cells megakaryocytes 2000 -3000 fragments = platelets • Plug damaged blood vessels • Promote blood clotting • Life span 5-9 days Hemostasis • Hemostasis = stationary blood • 1. Vascular reactions (spasm) – Response to damage – Quick reduction of blood loss • 2. platelet plug formation – Become sticky when contact damaged vessel wall • 3. blood clotting (coagulation) – Series of chemical reactions involving clotting factors • Clotting in unbroken vessel= thrombosis Coagulation • Extrinsic pathway common steps – tissue factor(TF) from damaged cells 1 • Intrinsic Pathway common steps – Materials “intrinsic” to blood 1 • 1. prothrombinase which causes • 2. prothrombin thrombin causes • 3. fibrinogen fibrin clot Clot Retraction & Vessel Repair • • • • • Clot pugs ruptured area Gradually contracts (retraction) Pulls sides of wound together Fibroblasts replace connective tissue epithelial cells repair lining Control Mechanisms • Fibrinolysis: dissolving of clot by activated plasmin enclosed in clot • Clots can be triggered by roughness on vessel wall = thrombosis • Loose clot = embolus and can block a small vessel = embolism Figure 14.5 Blood Types • Surface antigens- react with antibodies • Divided into groups based on antigens – > 24 blood groups and > 100 different antigens • We will deal with ABO and Rh groups ABO Group • • • • • Two antigens = A & B If have only A –type A If have only B –type B If neither then Type O Blood usually has antibodies that can react with antigens – e.g. anti-A antibody or anti-B antibody • You don’t react with your own antigens – Thus: type A has anti-B and vice versa Figure 14.6 Rh Blood Group • • • • Antigen discovered in rhesus monkey If have antigen- Rh+ Normally don’t have antibodies antibodies develop after the first exposure from transfusion Transfusions • If mismatched blood given antibodies bind to it and hemolyze cells • Type AB has no AB antibodies so can receive any ABO type blood called Universal recipients • Type O have neither antigen so can donate to any other ABO type called Universal donors • Misleading because of many other blood groups that must be matched The Cardiovascular system: Heart Chapter 15 Location • Thoracic cavity between two lungs – ~2/3 to left of midline • surrounded by pericardium: • Fibrous pericardium– Inelastic and anchors heart in place • Inside is serous pericardium- double layer around heart – Parietal layer fused to fibrous pericardium – Inner visceral layer adheres tightly to heart – Filled with pericardial fluid- reduces friction during beat. Figure 15.1 Heart Wall • Epicardium- outer layer • Myocardium- cardiac muscle – Two separate networks via gap junctions in intercalated discs- atrial & ventricular – Networks- contract as a unit • Endocardium- Squamous epithelium – lines inside of myocardium Figure 15.2a Figure 15.2b Figure 15.2c Chambers • 4 chambers • 2 upper chambers= Atria – Between is interatrial septum – Contains fossa ovalis- remnant of foramen ovalis • 2 lower chambers = ventricles – Between is interventricular septum • Wall thickness depends on work load – Atria thinnest – Right ventricle pumps to lungs & thinner than left Great Vessels Of Heart- Right • Superior & inferior Vena Cavae – Delivers deoxygenated blood to R. atrium from body – Coronary sinus drains heart muscle veins • • • • R. Atrium R. Ventricle pumps through Pulmonary Trunk R & L pulmonary arteries lungs Great Vessels Of Heart-Left • Pulmonary Veins from lungs – oxygenated blood • L. atrium Left ventricle • ascending aorta body • Between pulmonary trunk & aortic arch is ligamentum arteriosum • fetal ductus arteriosum remnant Figure 15.3a Figure 15.3b Figure 15.3c Valves • Designed to prevent back flow in response to pressure changes • Atrioventricular (AV) valves – Between atria and ventricles • Right = tricuspid valve (3 cusps) • Left = bicuspid or mitral valve • Semilunar valves near origin of aorta & pulmonary trunk • Aortic & pulmonary valves respectively Figure 15.4ab Figure 15.4c Figure 15.4d Figure 15.5a Figure 15.5b Blood Supply Of Heart • Blood flow through vessels in myocardium = coronary circulation • L. & Right coronary arteries – branch from aorta – branch to carry blood throughout muscle • Deoxygenated blood collected by Coronary Sinus (posterior) • Empties into R. Atrium Conduction System • 1% of cardiac muscle generate action potentials= Pacemaker & Conduction system • Normally begins at sinoatrial (SA) node • Atria & atria contract • AV node -slows • AV bundle (Bundle of His) • bundle branches Purkinje fibers • apex and up- then ventricles contract Pacemaker • • • • • • Depolarize spontaneously sinoatrial node ~100times /min also AV node ~40-60 times/min in ventricle ~20-35 /min Fastest one run runs the heart = pacemaker Normally the sinoatrial node Figure 15.6 Electrocardiogram • Recording of currents from cardiac conduction on skin = electrocardiogram (EKG or ECG) • P wave= atrial depolarization – Contraction begins right after peak – Repolarization is masked in QRS • QRS complex= Ventricular depolarization – Contraction of ventricle • T-wave = ventricular repolarization – Just after ventricles relax Figure 15.7 Cardiac Cycle • after T-wave ventricular diastole – Ventricular pressure drops below atrial & AV valves open ventricular filling occurs • After P-wave atrial systole – Finishes filling ventricle (`25%) • After QRS ventricular systole – Pressure pushes AV valves closed – Pushes semilunar valves open and ejection occurs – Ejection until ventricle relaxes enough for arterial pressure to close semilunar valves Action Potential • • • • • Review muscle Heart has addition of External Ca2+ creates a plateau prolonged depolarized period. Can not go into tetanus. Figure 15.8 Flow Terms • Cardiac Output (CO) = liters/min pumped • Heart Rate (HR) = beats/minute (bpm) • Stroke volume (SV) = volume/beat • CO = HR x SV Controls- Stroke Volume (S.V.) • Degree of stretch = Frank-Starling law – Increase diastolic Volume increases strength of contraction increased S.V. – Increased venous return increased S.V. • increased sympathetic activity • High back pressure in artery decreased S.V. – Slows semilunar valve opening Controls- Heart Rate • Pacemaker adjusted by nerves – Cardiovascular center in Medulla • parasympathetic- ACh slows – Via vagus nerve • Sympathetic - norepinephrine speeds • Sensory input for control: – baroreceptors (aortic arch & carotid sinus)- B.P. – Chemoreceptors- O2, CO2, pH Other Controls • Hormones: – Epinephrine & norepinephrine increase H.R. – Thyroid hormones stimulate H.R. – Called tachycardia • Ions – Increased Na+ or K+ decrease H.R. & contraction force – Increased Ca2+ increases H.R. & contraction force Figure 15.9 Exercise • Aerobic exercise (longer than 20 min) strengthens cardiovascular system • Well trained athlete doubles maximum C.O. • Resting C.O. about the same but resting H.R. decreased Figure 15.10 The Cardiovascular System: Blood Vessels and Circulation Chapter 16 Blood Vessels • Arteries- from heart 1. Elastic => large 2. Muscular => distribution to organs 3. Arterioles => distribution to capillaries- mostly muscle • • Capillaries- thin walled for diffusion Veins- to heart 1. Venules => from capillaries 2. Veins from tissue to vena cavae to heart Figure 16.1ab Figure 16.1c Blood Vessel Structure • Three layers • Arteries-> thicker tunica media – Elastic tissue and/or muscle – As they get smaller-> more muscle – Arterioles-> very muscular- control • Veins- bigger lumen and thinner walls • Veins-> valves to prevent backflow – Venules very thin, no valves Vessel Functions • Muscular arteries & arterioles regulate flow • Sympathetic activity to smooth muscle vasoconstriction (narrowing) • Decreased sympathetic activity or NO causes relaxation or dilation • Arterioles adjust flow into capillaries • Systemic veins & venules serve as blood reservoirs (~64% total blood volume) Capillary Details • Capillaries only have endothelium – Very thin cells & cell nuclei protrude into lumen- easy diffusion • Connected from arterioles to venules in networks – Sometimes direct route from arteriole to venule • Filling controlled by small arterioles & precapillary sphincters Figure 16.2a Figure 16.2b Capillary Exchange • Slow flow through capillaries – Allows time for exchange through wall • Blood pressure – filtration of fluid out of capillary – Mostly in first ½ of vessel length • Osmosis (protein concentration) – Reabsorption of fluid from outside to inside – Mostly in last ½ of vessel length • Balance determines fluid in circulation – Excess fluid returned via lymphatic system – Local signals can adjust capillary flow Figure 16.3 Venous Return • Blood enters veins at very low pressure. • Needs more pumping to get back to heart • = action of heart; muscle pumps; respiratory pump • Some pressure from heart action • Not enough to overcome gravity Muscle & Respiratory Pumps • Contracting skeletal muscles squeeze veins emptying them • Because of venous valves flow is toward heart • Respiratory pump has similar action • Inhalation decreased thoracic pressure & increased abdominal pressure – Blood flows toward heart • Exhalation allows refilling of abdominal veins Figure 16.4 Blood Flow • from high pressure area to lower pressure area, i.e. down pressure gradient – Greater gradient greater flow • Ventricular contraction blood pressure (BP) – Highest in aorta and declines as flows through vessels – 110-70 mmHg in aorta ~16 mmHg at venules – 0 at R. Atrium • Resistance= opposition to flow • depends on lumen diameter & length & blood viscosity – Smaller lumen greater resistance – Higher viscosity greater resistance – viscosity of blood depends on Hct Resistance • Depends on vessel lumen diameter – Smaller lumen greater resistance • And blood viscosity – Higher viscosity greater resistance – viscosity of blood depends on Hct • And total vessel length – Longer the length of flow the more friction with wall – Total body resistance increases with growth and addition of tissue Anatomical Design • Length and pressure • Design and local flow control- central pressure Pressure Gradients • Adult anatomy gives constant length • If central blood pressure is controlled it is constant • Only variable is radius of the arterioles • Each tissue can do it separately • Review design in picture below – All tissues have the same pressure gradient Pressure Gradients (Cont.) • Note pulse in aorta & large arteries – MAP • pressure fall related to resistance – Note role of arterioles • Note low venous pressures – can’t get back to the heart! Figure 16.5 Regulation of Blood Pressure & Flow • • • • • • Fast responses: e.g. standing up Slower responses: e.g. blood volume Distribution: e.g. to working muscles Balance of CO with flow to body Interacts with many other control systems Cardiovascular (CV) Center major regulator Inputs • Higher centers: – – – – – cerebral cortex, limbic system, hypothalamus HR increases before race; flow adjusted for body temperature • Sensory receptor input: – proprioceptors, – baroreceptors – chemoreceptors Inputs (Cont.) • Proprioceptors: – Start HR change as activity starts • Baroreceptors: in aorta & carotid pressure parasympathetic & sympathetic stimulation CO • Chemoreceptors: in aorta & carotid – Low O2, high H+, CO2 vasoconstriction BP Figure 16.6 Output • ANS to heart – Sympathetic HR & force of contraction – Parasympathetic HR • Vasomotor – to arterioles vasomotor tone – To veins move blood to heart BP Hormone regulation • Renin-Angiotensin system – Angiotensin II vasoconstriction+ thirst – aldosterone Na+ & water loss in urine on • Epinephrine & Norepinephrine CO • ADH = Vasopressin constriction BP Thirst & water retention in kidney BP • ANP- from cells in atria – Vasodilation & loss of salt & water in urine BP Figure 16.7 Checking Circulation- Pulse • Pulse in arteries = HR – Use radial artery at wrist, – carotid artery, – brachial artery • Tachycardia = rapid rest rate (>100 bpm) • Bradycardia= slow rest rate (<50 bpm) Blood Pressure • Use sphygmomanometer – Usually on brachial artery • Raise pressure above systolic– stop flow • Lower pressure in cuff until flow just starts – first sound Systolic Pressure • Lower until sound suddenly gets faint – Diastolic pressure • Normal values <120 mmHg for systolic & < 80 mmHg for diastolic Circulatory Routes • Two parts: Systemic & Pulmonary • Systemic circulation- throughout body – Oxygenated blood deoxygenated as it goes • All systemic arteries branch from aorta • All systemic veins empty into Superior Vena Cava, Inferior Vena Cava or the Coronary Sinus – Carry deoxygenated blood to heart Figure 16.8 Figure 16.9 Figure 16.10a Figure 16.10b Figure 16.10c Figure 16.11 Figure 16.12 Figure 16.13 Figure 16.14a Figure 16.14b Figure 16.14c Figure 16.15 Pulmonary Circulation • From right ventricle pulmonary trunk • R. & L. pulmonary arteries – Carry deoxygenated blood • R. & L. lungs – Gas exchange occurs • 2 R. & 2 L. pulmonary veins – Carry oxygenated blood • L. atrium Hepatic Petal Circulation • Portal vein transports blood from one capillary bed to another • GI organs • Splenic & superior mesenteric veins • hepatic portal vein • sinusoids in liver – Mixes with oxygenated blood • hepatic vein inferior Vena Cava Figure 16.16a Figure 16.16b Fetal Circulation • Specialized for exchange of materials with maternal blood and bypass of lungs • Exchange in placenta umbilical vein • liver ductus venosus • inferior vena cava R. atrium – Mixes with deoxygenated blood from lower body • foramen ovale L. Atrium • Or R. Ventricle Pulmonary trunk ductus arteriosus aorta • internal iliacs umbilical arteries Placenta Figure 16.17 At Birth • Umbilical arteries medial umbilical ligaments • Umbilical vein ligamentum teres • Ductus venosus ligamentum venosum • Placenta expelled • Foramen ovalis closes fossa ovale • Ductus arteriosus ligamentum arteriosum Aging • Stiffening of aortae • Loss of cardiac muscle strength – Reduced CO & increased systolic pressure • Coronary artery disease • Congestive heart failure • atherosclerosis