kkkkkkk
advertisement

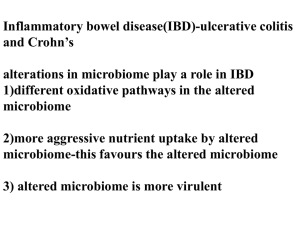
Parenteral NS • Fluid and electrolyte requirements. • Calculate enteral and parenteral formulations. PNS Routes • Peripheral access • Short-term central access • Long-term central access Peripheral Access • Veins in limbs • Cannot exceed 800-900 mOsm/kg • PICC - enter at peripheral but end of tube at subclavian vein Central Access • • • • • Figure 20-3 here Cephalic vein Subclavian vein Internal jugular vein Superior vena cava Fig. 20-3. Central access Central Access • Short-term – percutaneous technique • Long-term – implanted vascular devices PNS • Time frame for use of PNS – 5 days or less is short-term • Total nutrients needed • Capacity of pt to handle fluid PNS • Condition of peripheral veins • If can take adequate oral intake in 5 day - DO NOT do central line PNS Components • Protein – crystalline amino acids – 3% to 15% solutions – 10% = 100g protein/L – 4 kcal/g protein – NPC non-protein calories PNS Components • Carbohydrate – dextrose monohydrate – 5% to 70% solutions – D50W = 50% solution – 10% solution = 100g/L – 3.4 kcal/g dextrose PNS Components • Lipid – soybean or safflower oil – 10%, 20% & 30% solutions – 10% = 1.1 kcal/ml – 20% = 2.0 kcal/ml – 30% = 3.0 kcal/ml PNS Components • Lipid – 10% kcal/day every day will provide 4% of kcal need to prevent EFA deficiency – if have long chain fatty acids PNS Components • Electrolytes, vitamins, minerals PNS • PPN – less than 8.5% AA – 5-10% dextrose – lipid not more than 1g/kg/day PNS • PPN – Rule of thumb for PPN – D5W or D10W with 8.5% AA – D20W with 5% AA and lipid at 125 ml/hr PNS • Compounding methods – mix the dextrose and AA – ‘piggy’ back the lipid and filter before mix with dextrose and AA PNS • Initiating TPN – start less than 50 ml/hr and 1 L/day – advance 12 - 24 hr intervals PNS • Monitoring – amount receiving – Na –K – BUN – prealbumin PNS • Monitoring – cholesterol – TG –I&O – body wt – blood glucose McClaren 165. Essential fatty acid deficiency. McClaren 166. Same pt. 165 after EFA supplementation. Complications TPN • Catheter in wrong place • Sepsis • Deficiencies – EFA def – trace minerals - added routinely Complications TPN • Metabolic complications – overloading – imbalances Complications TPN • Overloading – solute or fluid - meas. Serum osmolality – CHO, fat, amino acids Complications TPN • Imbalances – glucose intolerance – hypokalemia – reactive hypoglycemia – hypophosphatemia – hypo or hypermagnesemia Refeeding Syndrome • Too aggressive administration after ‘starving’ • Hypokalemia • Hypophosphotemia Transition Feeding • Parenteral to enteral – start enteral slow – keep TPN going & decrease as increase enteral – receive 75% from enteral before stop TPN Transition Feeding • Parenteral to oral – start oral and slowly decrease TPN – be careful of hyperosmolality of common clear liquids – receive 75% of needs before stop TPN Transition Feeding • Enteral to oral – ?? – mOsm/kg for different clear liquids be careful not too high TPN END • Questions? • Now for calculations