A Real-time Electronic Medical
Record to Drive the Quality
Improvement Program of Haiti
On behalf of The Ministry of Public Health and Population (MSPP) & CDC-Haiti:
The HIVQUAL-Haiti Team
Bruce Agins, MD MPH; Director, HEALTHQUAL International
Kuala Lumpur, July 2013
Overview of the presentation
•
•
•
•
Haiti and HIV
EMR genesis and implementation.
HIVQUAL Haiti
How you use national data to drive
improvement at national level
• How the EMR is used at the clinic to drive QI
Situation of HIV epidemic in Haiti
HIV Prevalence in 20121
Adult
15-49
2.2% (1.9-2.6)
Women
2.2%
Men
2.0%
Urban
2.4%
Rural
2.0%
Prevalence estimated in 2012
Population =10,085,214 hab. (est
142,000 HIV+ (~1.4% de la pop)3
Around half of HIV+ (~ 60,000 - 71,000)4
are eligible for ART
Around 70% - 80% of eligible (~48,000)5
are on ART
2010)2
1 EMMUS-V (2012)
2 ihsi.ht
3 NASTAD Haiti
4 ONUSIDA
5 mesi.ht
Rationale for Implementing the EMR
Paper based system:
• Data collection and reporting processes separate
• Constraints for formatting data
• Difficulties for maintaining integrity of data
• Security and backup of data
• Difficulties for searching, analysis and sharing information
• 2005 I-TECH began developing iSanté at the request of the Haiti MOH and the Centers
for Disease Control and Prevention Global AIDS Program in Haiti (CDC GAP).
•
iSanté is an electronic medical record (EMR) that supports both individual and
population health care of patients in Haiti. .
• iSanté supports health care workers and clinics to manage and utilize patient data, and
facilitates timely and accurate reporting on national HIV, primary care and maternal
health service delivery and surveillance.
• There are more than 100 sites employing iSanté including government facilities, private
hospitals, faith-based organizations, NGOs, and other networks, with a total of more than
160,000 patient records. Forty-nine iSanté clinics / hospitals have local servers, which
eliminates reliance on slow Internet connections and allows automatic replication of
patient data to a central patient data repository.
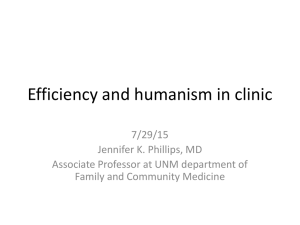
Architecture of the EMR
iSante is an open source
system developed in an
environment
LAMP (Linux OS, Apache
web server, MySQL
database, and PHP
scripting language)
Timeline for the Development of an EMR **
Phase 1 (~4 months)
Phase 3 (~10 months)
Refine paper-based HIV medical forms
Develop EMR for national pilot sites
Develop,
provide,
review, and
validate
forms
Finalize forms
and
guidelines on
unique
patient
identifiers
Identify reports to
be generated from
the database
Provide
support for
form use
Database matching
paper-based forms
Identify sites
for EMR
expansion
Protocols for data
cleaning, management,
and reporting
Interface to
support
interactive
EMR
Protocols for
use of EMR
and
reporting
Training,
implementation,
and support
Phase 2 (~9 months)
Develop data entry system for paper-based HIV medical record
**PARTNERSHIP BETWEEN HAITI MSPP-CDC-ITECH-TULANE
Deploy EMR
and train
personnel
The Rollout
• Development of system and preparation took
approximately one year
• Personnel capability required teamwork by an
electrical engineer, Database specialist,
Programmer Analyst and Network Specialist
• 10 people are engaged in operation of the system
• Customization can occur with appropriate skills
and knowledge
• Training of HCW requires 2 days
• Piloting was conducted over a 3-month period
Wide set of report for decision making
Multiple retrospective
or prospective reports
that generate case lists
for care reminders can
be use at all levels
Clinics
Departments
National
Visit scheduled next 7 days
USING THE EMR DATA AT THE NATIONAL LEVEL:
A Systematic Approach to Quality Improvement
HEALTHQUAL HAITI Timeline
December 2007
•the MOH adopted the HIVQUAL methodology as a national program for
monitoring and improving systems of care delivery for persons living with HIV.
•Constitution by MOH of a National Advisory Committee of PEPFAR partners and
stakeholders : (DG MSPP – LNSP – CDC – USAID – GHESKIO – PIH – AR - MSH –
ITECH – FOSREF – FHI – POZ – GF – FEBS).
•First training session on QI for HIVQUAL coaches by NYSDOH AI.
•19 HIV clinics were selected to begin HQ-HT, representing a mix of regions, clinic
types and degree of support by partners
•Ten performance indicators to measure the quality of HIV services covering
adult and pediatric care and treatment, and PMTCT.
August 2008
•
Data collection was expedited by the incorporation of the indicators
into the EMR : iSante
March 2012
•Decision of the National Committee to move towards HEALTHQUAL in 71 health
facilities
•19 indicators ( HIV - TB – MCH – Nutrition – Immunization - Mental health).
March 2013
•As of March 2013 , 90 health facilities are implementing HEALTHQUAL with the
backbone of an EMR
Quality Management
Program
HealthQual-Haïti Organigram
National Quality Advisory Board
Responsible: DG MOH
Secretariat
Resp: MOH
Core Team
Resp: MOH, CDC
HEALTHQUAL International
Resp: NYSDOH AI
Departmental Quality Committee
Resp : DD
Clinic Quality Committee
Resp : Medical Dir,
Coordinnator or Site Manager
Coaching Team
Resp: CDC
Departmental Quality Committee
Resp : DD
Clinic Quality Committee
Resp : Medical Dir,
Coordinnator or Site Manager
Departmental Quality
Committee
Clinical Quality
Committee
Semiannual meeting of National HEALTHQUAL
Advisory Board
– Evaluate performance improvement of clinics regarding
the indicators from the EMR
– Set benchmark for next review period.
– Identify weakness and gaps of the health system
– Provide feedback about implementing quality program
in the clinics
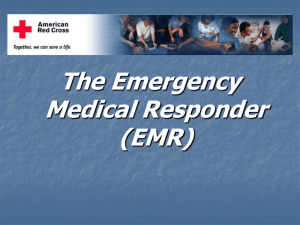
Cotrimoxazole Prophylaxis ( N: 10666 → 36685 pts )
Pourcentage de patients VIH+ qui ont reçu du Cotrimoxazole
100
Interventions
Earthquake- Cholera
Hurricane
Hanna
90
National
Score moyen des cliniques en (%)
80
70
• Diffusion of
National
Guidelines to all
clinics
• Distribution of
case list of taken
from iSanté to the
pharmacy unit
60
50
40
• Systematic data
entry of
pharmacy form in
iSanté
30
20
10
0
Jan-Juin
Juil-Dec
2008
Jan-Juin
Juil-Dec
2009
Jan-Juin
Juil-Dec
2010
Jan-Juin
Juil-Dec Oct-Mars Avr-Sept
2011
FY 2012
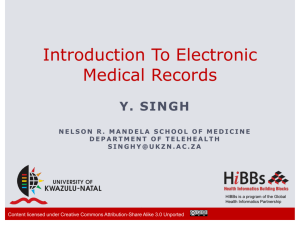
PMTCT ( N : 289 → 737 pts )
Pourcentage de femmes enceintes VIH+ ayant démarré la prise des ARV
100
Interventions
Seisme - Cholera
Cyclone
Hanna
90
National
Score moyen des cliniques en (%)
80
• Revision and
dissemination of
PMTCT Guidelines
• Introduction of
female Case
Managers in all
clinics.
70
60
50
• Agressive Tracking
of HIV+ PW by field
agents in the
community.
40
30
20
• Early dispensing of
ART HIV+ PW
10
0
Jan-Juin Juil-Dec Jan-Juin Juil-Dec Jan-Juin Juil-Dec Jan-Juin Juil-Dec Oct-Mars Avr-Sept
2008
2009
2010
2011
FY 2012
• Systematic data
entry of OBGYN and
pharmacy form in
iSanté.
USE OF EMR AT CLINIC LEVEL TO IMPROVE QUALITY
ANALYSES
SYSTEMES
Implémentation
Idées pour
surmonter les
Barrières
Improvement of ART enrollment through improvement of quality of service
Experience of Hopital Universitaire de la Paix
Derival Raymonde, MD; Bogart Mie Johanne, Nurse; Maisonneuve Yvette, Nurse; Isaac Daniel, SW; Aristile William,Data
Clerk; Auguste Marie Carmen , Nurse; Jenny X; Clerrier Nadege
Immunisation
PMTCT
Family Planning
Nutrition assess
TB Screnning
Adherence
Px TMS
ARV Enrol
HIVQUAL report jul-dec 10
Monit CD4
100
90
80
70
60
50
40
30
20
10
0
Continuity ARV
%
BACKGROUND -Rationale of the ART Enrollment project
All medically eligible HIV positive patients should be enrolled on
ART. ART enrollment will reduce the morbidity and mortality
rate and improve the patients’ quality of life.
From our Electronic Medical
Record, data of HIVQUAL
report from July to Dec 10
revealed that only 82 among
331 medically eligible
patients (24.8%) had
benefited from ART
enrollment.
A multidisciplinary team was created by the
Quality Management Committee to assess the
problem, led by 1 MD , with 3 nurses, 1
data cler, 1 field agent and 1 patient.
AIM STATEMENT: To improve ART enrollment
from 24.8% to 45% over six months.
IMPROVEMENT CHANGES &
INTERVENTIONS
First Strategy-Patient Awareness:
Psychologist & SW counsel patients about
importance of visits; Clerk highlights new
patients in register
Second Strategy - Reduction in Pre-ART period:
Weekly visits required for patients until ART
Enrollment.
Third strategy –Enrollment Acceleration:
Increase number of new enrollees with new
verifcation process by data clerk. Participation
in post-test clubs.
Reduction of pre-ART wait
and increasing patient had
the greatest impact
LESSONS LEARNED:
-Coordination between psychosocial and
medical units was key to success of ART
enrollment.
-Need sufficient time for committee meetings to
select patients for enrollment from pre-ART list.
-Staffing levels require more than one
psychologist to help patients accept treatment and
address mental health problems.
IMPLEMENTATION NEEDS AND CHALLENGES
• Technology
– power
– IT (Servers, LAN, PC…)
• Workforce: EMR and QI
– Involvement of all MOH unit in the deployment of EMR and Healthqual
program
– Reinforcement of capacity of MOH departmental staff in data analysis,
quality improvement
• Resources
– Financial and human
Lessons learned
• Utilization of iSante allowed standardization of care across
the country
• Leadership and commitment of highly qualified personnel
are needed for development and rollout of the system with
adequate financial reosurces
• Reminders in the EMR can prevent harm and improve
quality of care
• A national quality improvement strategy (HEALTHQUAL
Haiti) was required to spread implementation of data use
for improvement throughout the country and required
government ownership with support from donors to build
technical capacity and management processes
• Check it out….
• https://isantedemo.cirg.washington.edu/isante/
• username: demo
• password: demo
Special thanks to Nicasky Celestinn and Margareth Jasmin
 0
0