File

Case Study
Presentation
Angela Stancil
Dietetic Intern
10/18/13
Pre-diabetes
Impaired Fasting Glucose (IFG) or Impaired Glucose Tolerance (IGT)
Occurs when hyperglycemia is present but diabetes has not been diagnosed
Behan KJ. New ADA guidelines for diagnosis, screening of diabetes. Laboratory.2011;20 (1):2. http://laboratory-manager.advanceweb.com/Archives/Article-
Archives/New-ADA-Guidelines-for-Diagnosis-Screening-of-Diabetes.aspx
. Accessed October 16, 2013.
States with Highest Percentages of U.S. Adults Who
Have Ever Been Told They Have Pre-diabetes, 2010
State
Tennessee
California
Hawaii
Idaho
Kentucky
Alabama , Alaska
New Hampshire
Mississippi
Minnesota
Percentage
7.2
7.0
6.8
6.7
6.6
10.2
8.0
7.5
7.3
States with Lowest Percentages of U.S. Adults Who
Have Ever Been Told They Have Pre-diabetes, 2010
State
Vermont
Wyoming, Massachusetts
Montana
Utah
South Dakota
Ohio, Connecticut
Iowa, Nebraska
New York, Illinois, D.C.
Percentage
5.2
5.3
5.4
5.5
4.4
4.8
4.7
5.1
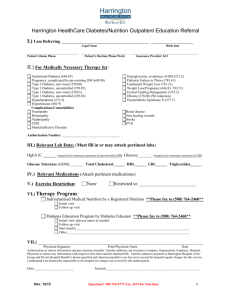
Tennessee - Percentage of Adults (aged 18 years or older) Reporting Pre-diabetes, 2008 - 2010
Etiology
Under Normal Conditions
Liver makes basal level of glucose
Body is able to sense changes in basal BG level and is adjusted
When you eat:
Insulin increases
Blood glucose decreases
Etiology
Pre-diabetes/Diabetes
Take in more CHOs than insulin is able to clear
Extra calories stored as visceral fat
Visceral fat releases chemicals
Insulin increases
Gluconeogenesis increases
Kidney is unable to clear excess glucose
3 P’s
Excess glucose stored as visceral fat
FFA released
Risk Factors
Symptoms
Acanthosis nigricans
Complications of Disease
Treatment
Mr. H
Overview of Patient
51 y/o, AA, M
Past Medical History:
GERD, Colonic polys, Chronic arthritis, smoking, ETOH, marijuana use
Medical Diagnosis: Pre-diabetes
Referred to Nutrition Copper clinic due to A1C of 6.2 and the
3 P’s
Nutrition Assessment
Anthropometrics:
Ht: 68 in.
Wt:144.3 lbs
DBW: 138 – 169 lbs
% DBW: 94%
Recent Weight Changes: -2 lbs since last visit with PCP
BMI 21.9 (normal)
Nutrition Assessment
Pertinent Labs: A1C of 6.2 % , all other labs WNL
Pertinent Medications: Omeprazole
Physical Activity : None
Diet History:
Breakfast Lunch
Nothing Nothing
Dinner
"country meal“
Proteins: baked chicken
Vegetables: mashed potatoes, lima beans
Grains: roll, cornbread
Snacks
Snack cakes
(oatmeal cream pies) candy bars
(Paydays, Kit-
Kats) pork rinds (after dinner)
Beverages
Water
Cranberry juice (
4-5 8 oz servings daily)
≤ 1 soda per day
Nutrition Diagnosis
Imbalance of nutrients related to meal inconsistency and frequent intake of calorically dense snacks as evidenced by
A1C of 6.2% at last PCP visit.
During the Session the Following was Discussed:
Concern about improving blood glucose to prevent diabetes
Desire to eat healthier foods
Concern about vision
Sleep
Patient mentioned fasting for religious reasons for up to 7 days at a time
Nutrition Education
Patient was educated on how hyperglycemia can negatively affect organs
Patient was introduced to the importance of maintaining blood glucose through meal consistency
Handouts provided:
Nutrition Goals
Nutrition Intervention
NUTRITION PRESCRIPTION:
Decrease blood glucose to A1C ≤ 5.7 %
NUTRITION INTERVENTION:
1.
Meal consistency a. aim for three meals/snacks daily
2. Choose foods that you like for these meals
3. Reduce juice to ≤ 4-8oz. servings/day
NUTRITION MONITORING and
EVALUATION:
Lab values WNL - A1C at goal of ≤ 5.7 %
Comply with appropriate diet - meal or snack three times daily
Summary
Disease Prognosis
“Without lifestyle changes to improve their health, 15% to
30% of people with pre-diabetes will develop type 2 diabetes within five years.”
Center for Disease Control and Prevention
Nutrition Prognosis
Comprehension : Good
Expected Compliance : Fair – the patient seemed to understand the importance of changing his diet but not ready to make big changes
Q & A
References
American Diabetes Association. Prediabetes. Diabetes Basics webpage. Available at http://www.diabetes.org/diabetes-basics/prevention/pre-diabetes/ . Accessed October 14, 2013.
Center for Disease Control and Prevention. Diabetes Report Card 2012:National and State Profile of
Diabetes and its Complications. Diabetes webpage. Available at http://www.cdc.gov/diabetes/pubs/reportcard/prediabetes.htm. August 12, 2012. Accessed October
14, 2013.
Center for Disease Control and Prevention. Prediabetes. Diabetes webpage. Available at http://www.cdc.gov/diabetes/consumer/prediabetes.htm
. August 13, 2012. Accessed October 14,
2013.
National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health.
Prediabetes: What You Need to Know. Available at http://diabetes.niddk.nih.gov/dm/pubs/prediabetes_ES/ . July 24, 2013. Accessed October 14, 2013.
Center for Disease Control and Prevention. Diabetes Data and Trends. Diabetes webpage. Available at http://apps.nccd.cdc.gov/DDTSTRS/Index.aspx?stateId=47&state=Tennessee&cat=riskfactorsfordiab etes&Data=data&view=TO&trend=Prediabetes&id=27 . Accessed October 16, 2013.
Center for Disease Control and Prevention. 2011 National Diabetes Fact Sheet. Diabetes webpage.
Available at http://www.cdc.gov/diabetes/pubs/general11.htm
. May 20, 2011. Accessed October 16,
2013.