Commissioning Plan Refresh 2015/16
advertisement

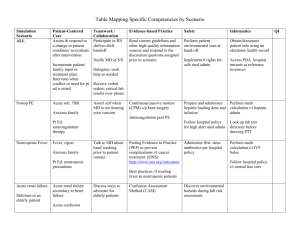
Commissioning Plan Refresh 2015 - 2016 Context Five Year Forward View: - Focus on prevention and CCG partnership working with LA/ Public Health; Obesity/ smoking/ alcohol/ other risk factors - Development of Multi-speciality Community Providers - Integration opportunities within Health and Social Care Economy - Implement primary care co-commissioning as joint commissioners - New models of primary care provision - Future hospital models strategy to be developed; Capita ‘end to end review’ phase 2 to support - Dedicated resource delivered Winterbourne View action plan 2014/15. All cases allocated to Continuing Treatment Review. Financial Context Financial plan overview: - Exit 2014 / 15 with underlying deficit Distance from target remain £12m (4.6% ) BCF contribution exceeds minimum requirement £7.5m (3%) QIPP challenge identified Builds in activity growth based on historic trends and provider consultation - Financial plans deliver NHS England business rules in full - Provider economic models used in consultation with main acute provider to identify cost improvement opportunities aligned to CCG change programmes - 10% reduction in running costs delivered Operational Delivery 2015/ 16 Improving Quality: - Outcomes based commission supported by COBIC for intermediate care - 2 year contracts awarded in 2014/15 with all providers - Strong quality measures within contracts - Managed and monitored via monthly contact quality meetings - Clinical quality focus groups themed to address areas requiring improvement involving provider and commissioning clinicians - Triangulation of patient experience, complaints and patient forum to feed into quality review process - Regular clinical audits presented from providers Operational Delivery 2015/ 16 Constitutional Standards: - Consistent use of the NHS Standard Contract Early warning measures built into local quality standards Planned capacity in contracts to meet RTT standards (fig1) Delivery plans for achievement of sustainability of Accident and Emergency performance - Adequate capacity within Improved Access to Psychological Therapies contract to maintain delivery. Access delivered (Q4 2014/15) and waiting time targets (Q4 2014/15) Scatter plot between elective activity plans 2015/16 and incomplete spells (fig 1) 120,000 R² = 0.9999 Planned cumulative total EL and DC 100,000 80,000 60,000 Series1 Linear (Series1) 40,000 20,000 0 5000 10000 15000 20000 25000 Cumulative total incomplete pathways 30000 35000 Operational Delivery 2015/ 16 Information Revolution and Transparency: - NHS Number as primary identify in contracts since 2014/15 NHS Number adopted by Local Authority for Better Care Fund Electronic prescribing in all practices from 2014 /15 SystmOne provides online patient access to 23 practices Electronic discharge summaries commenced 2012 /13 - 95% received with 21 day local quality standard for 7 days not met - Integrated Digital Care record procurement on-going - Stage 2 Work following on from select committee inquiry into information sharing - Referral Facilitation will increase electronic referral rate Operational Delivery 2015/ 16 Modern Health and Care Workforce: - Training and development program for care home staff - Support for primary care nursing workforce via Practice Makes Perfect educational programme - Accredited training program with Edge Hill University for nursing revalidation - Promoting whole system workforce plan across providers - Working with North West Continued Professional Development Visual Overview Community Primary Care Ambulatory Emergency Care Elective Psychiatric Liaison Sub Acute Services Intermediate Care Referral Gateway Specialised Impact Non-Elective Change Programmes Foundations Foundations Primary Care Clustering GP/ primary care services around identified population Delivering sustainable primary care services by integrated working approaches and workforce skill mix Increased and extended hours access Reducing service variability and delivering consistent high quality primary care services Delivery of ‘core’ Primary Care service in all practices Impact: Increases accessibility of primary care services Reduces unscheduled acute activity Promotes patient self management Manages pro-active care Contributes to improved wellbeing and quality of life for service providers and patients Secures sustainable Primary Care Acuity/Complexity Model of Care Warrington Health Plus By utilising collaborative approaches across primary care, deliver a range of projects to transform care and models of delivery; Guided Care to work with patients to manage their own health conditions and access wider services to impact on the determinants of health and wellbeing Risk Stratification system to focus resources on managing complex patients closer to home, Complex Case Management to work with risk stratification to support complex patients maintaining stability and preventing avoidable unscheduled care activity Care Homes enhanced support to target this patient cohort, working with care homes staff to increase skills, identify consistent high quality care interventions and prevent avoidable unscheduled activity Telecare to increase capacity in primary care by enhancing the range of models available to offer health care and innovative health monitoring strategies Impact: Increases the range of community support available Promotes multi agency working and resulting potential efficiencies Reduces unscheduled acute activity by effective maintenance of complex patients Focuses resources for maximum benefit and return on service investment Contributes to pro-active care improved wellbeing and quality of life Reduces reliance on reactive primary care / community service provision by proactive interventions Promotes patient self-care, reduces reactive care reduces long term care need Our Map to the Future - Overview Hospital Services Non bed-based acute services GP Practice GP Practice (With Care Coordination) Intermediate Care Facility (bed bases) ‘Primary Care Home’ Clusters of Practices work collaboratively; other provider services refocused around the registered list Primary Care Home Delivery Team (Multi disciplinary team including community nursing/mental health/care coordinator/GP for nursing homes etc.) Paediatric Acute Response Team(PART) Community Services Restructure of services around practice populations; with WHP and acuity model to facilitate development Provision of care closer to home; delivered in cluster bases and patients own homes Providing responsive multi-professional interventions based on risk factors to prevent escalation Working across organisational boundaries; delivering integrated approaches based on user need Utilise telehealth/ telecare and integrated IT solutions to maximise efficiency Impact: Increases consistency and quality of service provision Promotes multi agency working and resulting potential efficiencies Reduces unscheduled acute activity Encourages patient self management Contributes to improved wellbeing and quality of life Change Programmes Referral Gateway Manages effective elective referral system in partnership with primary care Non-Elective Ensures referrals reach right clinical specialism first time, prevents multiple hand offs/ duplicate referrals for same patient Provides primary care with expert advice and support for condition management/ diagnostic work up prior to referral to acute Ensures appropriate clinical pathway management has been implemented prior to acute referral Promotes best practice condition management and reduces variability of management and referral quality Utilises effective choose and book system, facilitates patient choice Identifies service gaps for potential commissioning redesign and community services development tier 2 services Referral Gateway Non-Elective Impact: Reduced 1st out patient activity Increased use of electronic referral Managed patient flow for better patient experience Releases capacity in primary care Opportunities identified for tier 2 service development resulting in reduced acute activity Acute costs released by use of appropriate use of community services Intermediate Care Jointly re-commission the service with LA to achieve truly integrated service Non-Elective Achieve consistent delivery, against defined service specification Improved outcomes for service users demonstrated by robust performance indicators Utilise prime provider/ contractor model to maximise efficiencies and streamline contract management Provide enhanced choices for community, primary and clinicians as alternative to acute care Reduces length of stay in acute care by facilitating earlier discharge Improved outcomes includes service users maximising independence and requiring reduced levels of on-going support Intermediate Care Non-Elective Impact: Reduced activity in Accident and Emergency by use of ‘step up’ Reduced unscheduled admissions by use of ‘step up’ Reduced length of stay by use of ‘step down’ Improved personal independence and wellbeing for patients Reduced reliance on complex care packages Reduced long-term care placements Reduces discharge delays Sub Acute Services Provision of sub acute service to support medically optimised patient to ‘step Non-Elective down’ from hospital care Facilitates development of ‘discharge to assess’ model to prevent unscheduled admissions to assess Provision to support primary care with ‘step up’ alternatives to avoid hospital admission for managed care interventions Explore multi-speciality provider models for the provision of this service (5YFV) Impact: Reduced activity in Accident and Emergency by use of ‘step up’ Reduced unscheduled admissions by use of ‘step up’ Reduced length of stay by use of ‘step down’ Improved personal independence and wellbeing for patients Reduced reliance on complex care packages Reduced long-term care placements Reduces discharge delays Psychiatric Liaison Non-Elective Provides effective and appropriate management and support for people with mental health issues attending hospital Optimises mental health in patients admitted for physical health problems Facilitates access to a range of appropriate mental health and other services to avoid unscheduled admission Facilitates work to achieve parity of esteem Impact: Potential to impact on whole care pathway for this patient cohort, primary, AED, tertiary and care homes to reduce avoidable activity by effective appropriate management Reduces length of stay in acute care for people with depression, delirium and dementia Reduces frequent attenders at Accident and Emergency Ambulatory Emergency Care Non-Elective Implement further Ambulatory Emergency Care pathways to manage minor and less complex patients (DVT Pathway implemented Q3 2014/15) Develop collaborative model of primary care provision in AED via a Service Delivery and Improvement Plan with Warrington and Halton Hospitals NHS Foundation Trust. Pathways will deliver right care, right place, right professional Supports frailty pathway by more effective and appropriate acute management, preventing avoidable admission Impact: Reduces avoidable unscheduled admissions Reduces zero – 1 length of stay for clinical assessment Facilitates mixed model of unscheduled care acute provision Delivery of Accident and Emergency Standard