et al
advertisement

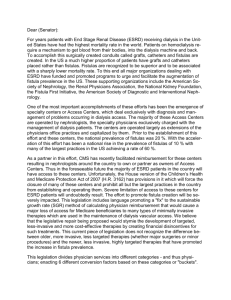
SNAP How to treat enterocutaneous fistulas Oslo - March 13, 2015 Pär Myrelid MD, PhD Dept of Surgery Unit of Colorectal Surgery Linköping University Hospital Linköping, Sweden Outline – Enterocutaneous fistulas (ECF) • Definition and classification • Causes of ECF • Dangers with ECF • Prevention • Prognosis • SNAP – the concept • Abdominal wall defects • Outcome and Quality of life 2 ECF – Definition and classification • An abnormal communication between two epithelialized surfaces – most often between the small or large bowel and the skin • Other common entries of the fistulas are e.g. bladder or vagina Fistula Inflamed small bowel 3 Berry et al Surg Clin North Am 1996, Evenson & Fisher J Gastrointest Surg 2006 ECF – Definition and classification • Simple fistula One bowel segment – fistula – skin • Complex fistula One bowel segment – abscess/fistula system – skin • Multiple fistula Multiple bowel segment involved • Entero-atmospheric fistula Bowel loops in abdominal defect (without fistulous tract) 4 Berry et al Surg Clin North Am 1996, Evenson & Fisher J Gastrointest Surg 2006 ECF – Definition and classification • Low-output fistula < 200ml/day • Moderate-output fistula 200-500ml/day • High-output fistula >500ml/day Berry et al Surg Clin North Am 1996 5 ECF – Causes • Surgical disasters (75 %) • Enterotomy after e.g. adhesiolysis • Anastomotic leak • Repeat laparotomies • Spontaneous (20-30 %) • Crohn´s disease • Cancer • Intra-abdominal sepsis (perforation) • Radiation enteritis • Ischemia • Trauma 6 Agwunobi et al Dis Colon Rectum 2001, Berry et al Surg Clin North Am 1996, Fischer et al J Trauma 2009, Falconi et al, Digestion 1999 The viscous circle ECF – Dangers • Sepsis • Intra-abdominal • Line sepsis • Fluid and electrolyte imbalance • Thrombosis • Malnutrition • 7 A high-output fistula (>500 ml/day) increases the risk of fluid and electrolyte imbalance as well as malnutrition Agwunobi et al Dis Colon Rectum 2001, Evenson & Fisher J Gastrointest Surg 2006, Kaushal & Carlson Clin Colon Rectum 2004 ECF – Prevention Colon • Risk assessment pre-operatively • Risk factors • Intra-abdominal sepsis (abscess/fistulas) • Steroid treatment • Low albumin • Malnutrition/weight loss (>10 % within 6 months or 5 % within 1 month) • Anemia • Emergency surgery • Severe adhesions • Increasing risk with increasing number of risk factors • High risk – consider diverting with temporary stoma 8 Myrelid et al Dis Colon Rectum 2009, Post et al Ann Surg 1991 Yamamoto et al Dis Colon Rectum 2000, Alves et al World J Surg 2002, Myrelid et al Colorectal Disease 2012 Ileum ECF – Prognosis • Late 1980´s mortality risk 40-65 % • Today 5-20 % mortality risk, in high output ECF still 30-35 % • Improved intensive care, management of sepsis, malnutrition, fluid/electrolyte imbalance and surgical technique • Up to 70 % close on conservative therapy 9 • Of those 91 % heal within 1 month of successful sepsis treatment • The remaining heal within 3 months Falconi et al Digestion 1999, Dudrick et al Digestion 1999, Reber et al Ann Surg 1978 ECF – Favourable prognosis • End fistulas (leakage through an intestinal stump) • Jejunal fistulas • Colonic fistulas • Continuity-maintained fistulas • Small-defect fistulas • Long-tract fistulas Martinez et al J Gastrointest Surg 2011, Prickett et al South Med J 1991 10 ECF – Unfavourable prognosis “FRIENDS” • Foreign body (e.g. mesh) • Radiation • Infection/Inflammation/IBD • Epithelialization of the fistula tract • Neoplasm • Distal obstruction • Steroids “With friends like these you don´t need enemies” Martinez et al J Gastrointest Surg 2011, Prickett et al South Med J 1991 11 ECF – Need of a dedicated team • Gastroenterologist • Colorectal surgeon • Nurses and nurses aids Refer patient to a • Nutritionist • Stoma therapist specialised centre! • Physiotherapist • Social worker • Home care • Pain care (try to withdraw opioids) • (Psychologist) Schein W J Surg 2008 12 SNAP – The Concept • SNAP • Sepsis and Skin care • Nutritional support • Anatomy • Patience and a Planned procedure 13 SNAP – Sepsis • Drain collections • CT/US-guided • (Open) • Prevent line-sepsis • Antibiotics • Anti fungus • Protect skin – wound care • Acidic/Alkaline • Enzymes • Decrease fistula output • PPI/Octeotride • Loperamide/Codeine Carlson Proc Nutrition 2003, Evenson & Fisher J Gastrointest Surg 2006 14 SNAP – Skin Care • Dedicated and creative stoma therapists Fistula opening 15 SNAP – Skin Care • Dedicated and creative stoma therapists 16 SNAP – Nutritional support • Compensate losses of fluid and electrolytes • Check for imbalance in urine as well • If the gut works – use it! • Patients loose appetite with parenteral nutrition • Parenteral nutrition/support • Remember risk of liver failure – if signs of cholestasis need of days without lipids • Home nutrition • Fistuloclysis 17 Levy et al Br J Surg 1988, Carlson Proc Nutrition 2003, Teubner et al Br J Surg 2004 , Lal et al Aliment Pharmacol Ther 2006 SNAP – Intestinal Anatomy • Rule out further collections • CT scan/Ultrasonography • If collections – Drain! • Define involved bowel segments • Make sure no down stream obstructions/stenosis • Endoscopy • Colonic contrast enemas • Stoma contrast enemas • Fistulogram (water soluble contrast) • 18 Sometimes combined with CT scan Carlson Proc Nutrition 2003, Schein World J Surg 2008 Teubner et al Br J Surg 2004 , Lal et al Aliment Pharmacol Ther 2006 Colonoscopy or colonic contrast investigation 19 Colonic enema passing through a mucous fistula Fistulogram - Contrast through the fistula to an ileocolonic anastomotic fistula 21 Fistulogram - Contrast through a prolapsing fistula which is 10 cm proximal of an end ileostomy CT and fistulogram - Fistula in a hernia with a catheter placed in the fistula No strictures between fistula and down stream loop ileostomy SNAP – Planned Procedure • Patience, patience, patience…… • Prolapse of bowel loops – “mature abdomen” • Softened adhesions • Plan for a whole day procedure • Experienced team of surgeons • Gentle and sharp surgery • Resect fistula segment • Put all bowel into continuity • Beware of anastomoses in septic area • No closed bowel loops 25 ECF – Abdominal wall defects • Often big defects • Component separation • Polyglactin mesh • Most certainly hernia later on • Biological mesh • Pig dermis Connolly et al Ann Surg 2008 26 ECF – Quality of Life • Low HRQoL • Improved after successful treatment • Dependant – burden for others • Leaks and wound care major impact • Patients develop coping strategies • Nurses important in the care and support Härle Master Thesis Linköping, 2013, Visschers et al Br J Surg 2008 27 ECF – Outcome • Closure achieved in approx 85 % of operated ECF patients • Severe morbidity • Postop infections Approx mortality • Totally 15 % • Low output fistulas 6% • High output fistulas 30 % • Complex fistulas 40 % Martinez et al World J Surg 2008 28 Take Home Message • Prevent enterocutaneous fistulas • Pre-operative risk stratification • If complication - divert • When enterocutaneous fistulas occur 29 • Sepsis and skin care • Nutritional support • Intestinal anatomy clarified • Planned procedure • Dedicated team • Patience! Thank you Acknowledgement For photos and truly dedicated work Åsa Gustafsson & Christina Schulz www.liu.se