Headache in chidren - Pediatrics
advertisement

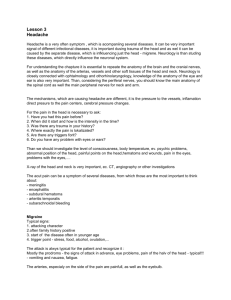
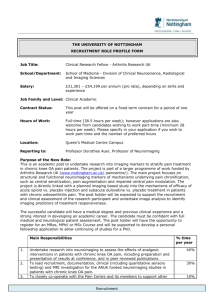
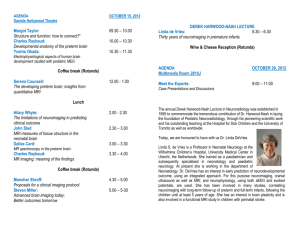
Headache , Meningitis Advancements in diagnostic imaging have revolutionized the practice of modern medicine. Neuroimaging allows more accurate diagnosis of central nervous system disorders and analysis of neuroanatomical differences. Observation of current practice patterns indicates that neuroimaging overuse is common in the clinical evaluation of certain symptoms such as headache in children and adolescents Details of bony structures: Provides good details about bony structures Details of soft tissues: Less tissue contrast compared to MRI Time taken for complete scan: Usually completed within 5 minutes Cost: from $1,200 to $3,200; they usually cost less than MRIs. Helical (spiral) scanners obtain images in fractions of a second and allow rapid, high-quality threedimensional and two-dimensional reformations. sedation is not necessary for CT scanning Disadvantages: Exposure to high to moderate radiation dose : Doses from a single pediatric CT scan can range from eabout 5 mSv to 60 mSv. Among children who have undergone CT scans, approximately 1/3 have had at least 3 scans. In comparison to some of the Japanese survivors of the atomic bombs who received 5 to 20 mSv . These survivors, who are estimated to have experienced doses only slightly larger than those encountered in CT, have demonstrated a small but increased radiation-related excess relative risk for cancer mortality. Pregnant women should not have CT scans . Radiation Dose Comparison Typical Effective Dose (mSv)1 Number of Chest X rays (PA film) for Equivalent Effective Dose2 Time Period for Equivalent Effective Dose from Natural Background Radiation3 Chest x ray (PA film) 0.02 1 2.4 days Skull x ray 0.1 5 12 days Lumbar spine 1.5 75 182 days I.V. urogram 3 150 1.0 year Upper G.I. exam 6 300 2.0 years Barium enema 8 400 2.7 years CT head 2 100 243 days CT abdomen 8 400 2.7 years Diagnostic Procedure MRI scans are best for imaging soft tissue. Details of bony structures: Less detailed compared to CT scan MRI machines can produce in any plane without moving the patient. They also have the ability to change the contrast of the images making them more clear than CT scan. Costs range from $1200 to $4000 (with contrast); which is usually more than CT scans and X-rays, and most examining methods. Time taken for complete scan: about 30 minutes. Disadvantages People with surgical clips, metallic fragments, cardiac monitors cannot have MRI. In cases with pacemakers MRI’s magnetic and radiofrequency fields can disrupt the pacemaker’s setting or cause wires to overheat, resulting in unintended heart stimulation, device electrical failure, or tissue damage.and even Trigger rapid pacing. But in Feb. 2011 FDA approves 1st pacemaker designed to work safely during some MRI exams (Medtronic's Revo MRI SureScan ) costs $5,000 to $10,000 Magnetic Resonance Angiography (MRA) and Computed Tomographic Angiography (CTA):For studies of the intracranial vasculature Cerebrospinal Fluid Flow Imaging: detects interruptions of normal flow patterns. Useful In patients with Chiari I and II malformations when they are being considered for foramen magnum decompressions. Magnetic Resonance Neurography: highlight nerve fascicles as they course through the brachial plexus, arms, legs, or neck. excellent for searching for intrinsic pathology in peripheral nerves Magnetization Transfer: (MTC) is useful in assessing myelination and demyelination Perfusion Imaging Diffusion Tensor Imaging:can be used to assess brain maturation, detects reduced diffusion in the acute phase after a traumatic, metabolic, or toxic injury to the brain. Proton MR Spectroscopy:useful in the assessment of encephalopathic neonates , in detection and diagnosis of some inborn errors of metabolism , in developmental delay , and in post-therapeutic assessment of intracranial tumors Special Imaging of Brain Function Common symptom in children and adolescents. Has many potential causes, but clinicians generally distinguish primary headache (ie, pain without evidence of a serious underlying illness) from secondary headache (ie, pain resulting from a serious pathologic condition). Neuroimaging can be a valuable diagnostic tool for conditions for which headache is coupled with other worrisome signs and symptoms. Practice parameters for the evaluation of children and adolescents with recurrent headaches, published in 2002, recommend that diagnostic neuroimaging be considered for children with an abnormal neurologic examination or other historical features that suggest neurologic dysfunction. These recommendations emphasized that obtaining a neuroimaging study on a routine basis is not indicated for children with recurrent headache and a normal neurologic examination. Change in the pattern of headache Onset of seizures Headache associated with systemic illness, including fever Personality change Symptoms suggestive of raised intracranial pressure, such as new onset headache in the early morning; or headache that is worsening with coughing, sneezing, or straining An abnormal neurological finding, unless the finding is longstanding. In this present study neuroimaging findings in 400 nonacute pediatric headache patients from the most recent study years 2000 and 2004 were analysed neuroimaging results were categorized as normal, remarkable without clinical action, remarkable with clinical follow-up action, and abnormal. 185 of 400 patients (46%) had neuroimaging. Of these, 78.4% of neuroimaging studies were normal, and none was considered abnormal. 21.5% had remarkable findings in the neuroradiology report. One third of these patients received further consultation or neuroimaging because of incidental findings. Conclusion: In the evaluation of nonacute pediatric headache, overuse of neuroimaging leads to frequent discovery of incidental findings and increased testing. Urgent scan if any of the following: Witnessed loss of consciousness >5 minutes worsening level of consciousness Amnesia (antegrade or retrograde) >5 minutes Abnormal drowsiness ≥3 Discrete episodes of vomiting Clinical suspicion of nonaccidental injury Post-traumatic seizure GCS <14 in emergency room (Paediatric GCS <15 if aged <1) Suspected open or depressed skull fracture or tense fontanelle Signs of base of skull fracture Focal neurological deficit Aged <1 - bruise, swelling or laceration on head >5 cm Dangerous mechanism of injury (high-speed RTA, fall from >3 m, highspeed projectile) MRI is particularly indicated in patients with one or more of the following. Onset of seizures at any age with evidence of focal onset in history or EEG. Onset of unclassified or apparently generalised seizures in the first year of life or in adulthood. Evidence of a focal fixed deficit on neurological or neuropsychological examination. Difficulty in obtaining control of seizures with first-line anti-epileptic drug treatment. Loss of control of seizures with anti-epileptic drugs or a change in the seizure pattern that may imply a progressive underlying lesion. Imaging studies are not the means by which meningitis is diagnosed; therefore, imaging is not performed routinely other than to ensure the absence of hydrocephalus or abscess before a lumbar puncture is performed. Neuroimaging is indicated if the clinical diagnosis is unclear, if neurologic deterioration occurs secondary to increased intracranial pressure, if the meningitis is associated with persistent seizures or focal neurologic deficits, or if patient recovery from the disease is slow And finally imaging is best reserved to look for complications of meningitis in children with complicated clinical courses. Computed tomography and MR studies in uncomplicated cases of purulent meningitis are usually normal. Occasionally, some enhancement of the meninges will be seen on postcontrast scans . In granulomatous meningitis, enhancement is most typically seen in the basal meninges In bacterial meningitis typically shows enhancement over the cerebral convexities. In either type of meningitis, contrast-enhanced MR is more sensitive than contrast-enhanced CT in detecting inflammatory changes in the meninges Clinicians are reliant on CT to detect patients where LP should be avoided . In a series of 445 children by Rennick, 4.3% of patients had clinical signs of herniation. CT was performed at the time of herniation in 14 patients and five (36%) of the scans were normal despite the clinical picture. In another study, approximately 50% of patients with clinical features suggestive of raised intracranial pressure had a normal CT scan There is evidence to show that performing a CT prior to lumbar puncture may delay the institution of antibiotics with the time delay ranging from 2 to 4.9 hours A thorough clinical assessment prior to imaging is important as the imaging findings may not be supportive of raised intracranial pressure and may provide false reassurance for clinicians. Hydrocephalus evaluated well by all imaging modalities; MR is the most effective at localizing the level of the obstruction Thrombosis of deep veins, cortical veins, and venous sinuses is an uncommon complication of meningitis. Develops more often in the presence of superimposed dehydration. In the acute phase (when the clot is dense), thrombus can be seen on CT as high density in the sagittal sinus on a noncontrast scan . Subacute sinus thrombosis is recognizable on CT by the so-called “empty delta sign,” which is a triangle of decreased density in the posterior portion of the affected sinus on a contrast enhanced scan. On MR, sinus thrombosis is readily diagnosed when the thrombus is subacute Figure 11-16 Sagittal sinus thrombosis secondary to meningitis. A: Noncontrast CT scan shows high attenuation in the torcular herophili (arrows) at the junction of the straight sinus (also hyperdense and thrombosed) and the superior sagittal sinus. The presence of high density within blood vessels in a child beyond the first few months of life is extremely suspicious for sinus thrombosis. B: Sagittal SE 600/11 image shows high signal intensity in the posterior half of the superior sagittal sinus (black arrows). The straight sinus (white arrowheads) also appears thrombosed. C: Coronal FLAIR image shows high signal intensity (arrow) within the superior sagittal sinus, supporting the diagnosis of sagittal sinus thrombosis. D: Axial SE 2500/70 image shows hyperintensity in the superior sagittal sinus, suggesting the presence of extracellular deoxyhemoglobin, present in subacute clot. E: Two-dimensional time of flight MR venogram shows absence of flow-related enhancement in the superior sagittal sinus and straight sinus, confirming the diagnosis of thrombosis. On CT, venous infarcts are usually poorly delimited, hypodense or mixed attenuation areas involving the subcortical white matter and producing a slight mass effect on ventricular structures The low attenuation is probably due to localized cerebral edema, whereas high attenuation areas usually represent hemorrhage. On MR, early venous infarcts may be identified by visualization of prolonged T1 and T2 relaxation times. Another early imaging sign is visualization of thrombus in the deep medullary veins with surrounding cavitatio 25 % of venous infarcts are hemorrhagic and have an imaging appearance that varies from large subcortical hematomas to petechial hemorrhages within edematous brain parenchyma The hemorrhages are generally subcortical and often multifocal with irregular margins. They are occasionally linear in nature, indicating hematoma in and around the vein. Figure 11-19 Periventricular venous infarctions in meningitis. A: Noncontrast CT early in the course of the disease shows subtle hyper- and hypodensity (arrows) in the periventricular white matter. B: Axial SE 3000/120 image the following day shows linear T2 shortening (arrows) in the deep frontal and parietal white matter bilaterally. C: Coronal FSE 3500/95 image shows small areas of cavitation between and around the thrombosed medullary veins. D: Follow-up noncontrast CT one week later shows increasing hypodensity (arrows) in the deep white matter. Figure 11-20 Bilateral middle cerebral artery infarcts secondary to meningitis. A: Noncontrast CT shows low attenuation bilaterally in the distribution of the middle cerebral arteries. B: At a higher level, the low attenuation is seen to involve the entire middle cerebral artery distribution (arrows) bilaterally. Arterial infarctions in the setting of meningitis are usually the result of arteritis secondary to involvement of the perivascular spaces and, subsequently, the arterial walls by the infection. CT or MR can reliably diagnose arteritis in the setting of meningitis by identifying the resulting infarcts, which tend to be sharply marginated and confined to a specific arterial vascular territory Diffusion weighted imaging is useful in this setting, as it will detect infarctions earlier . Frequently, multiple lacunar type infarcts are seen in the distribution of perforating vessels in the brainstem, basal ganglia , and white matter, presumably resulting from involvement of the basilar cisterns and vessels contained therein. Infants with meningitis, particularly H. influenzae, frequently develop subdural effusions Effusions are iso-intense to CSF on CT, may be slightly hyperintense to CSF on MR , and are most commonly located over the frontal and temporal regions of the brain. Occasionally, a portion of the medial surface (the cerebral surface), of an effusion will show enhancement These effusions typically regress along with the signs of meningitis over several days. Subdural empyemas show reduced diffusion compared with CSF, whereas effusions do not. It is a common complication of neonatal meningitis. The organisms enter the ventricles via the choroid plexuses. The best imaging sign of ventriculitis is the presence of proteinaceous debris in the dependent portion of the ventricle, usually the trigone or occipital horn of the lateral ventricle . If contrast is administered, intense enhancement of the inflamed ependyma is seen on both CT and MR Magnetic resonance has, perhaps, a greater sensitivity to the inflammatory process. The ventricles are nearly always dilated from reduced CSF absorption. A more ominous complication of ventriculitis is necrosis of periventricular white matter. Ultimately, multiple loculations form in the brain, separated by thin septae The septae are likely formed by astroglial response to the infection. Ultrasound and MR detect the septae better than CT. Figure 11-23 Subdural empyemas and ventriculitis secondary to meningitis. Utility of diffusion weighted imaging. A: Axial noncontrast CT show asymmetrical fluid collections over the frontal convexities. Although large CSF spaces are normal in the first year of life, they are normally symmetrical. The frontal horns are disproportionately large, suggesting injury to the frontal white matter. B: Axial SE 3000/120 image shows abnormal heterogeneity (white arrows) in the asymmetrical CSF spaces over the frontal convexities. In addition, the frontal white matter is abnormally hyperintense. C: Postcontrast SE 600/11 image shows abnormal enhancement of the frontal cortex and leptomeninges. D: Axial apparent diffusion coefficient image shows abnormally low diffusion in the fluid collections over the frontal convexities; the CSF in normal brains is hyperintense on these images. E: Axial postcontrast SE 600/11 image shows a possible fluid-fluid level (arrow) in the left occipital horn. F: Axial apparent diffusion coefficient image shows reduced diffusion (manifested as low signal intensity, arrows), diagnostic of blood or, in this case pus, layering in the occipital horns of both lateral ventricles. Thank you