Subramanian
advertisement

Income inequality and health
S V Subramanian
Harvard School of Public Health
Acknowledgements: Ichiro Kawachi
January 6, 2006
PURE Steering Committee and Operation Meeting
Dubai, UAE
Income inequality: some facts
S V Subramanian
2
World inequality
S V Subramanian
Source: UNDP, 2005, Human Development Report
3
World inequality trend
Source: Milanovic B, World Apart: international and world inequality
S V Subramanian
4
What is driving global income inequality?
• Largely between-country (rather than withincountry)
• BUT, within country contribution not trivial
– Of the 73 countries for which data are
available, 53 (80% of the world’s population)
have seen inequality rise, while only 9 (4%
of the population) have seen it narrow.
S V Subramanian
5
Income distribution in the US
S V Subramanian
6
Is this news?
Sources: 1947-79: Analysis of U.S. Census Bureau data in Economic Policy Institute, The State of Working America 1994-95 (M.E.
Sharpe: 1994) p. 37.; 1979-2001: U.S. Census Bureau, Historical Income Tables, Table F-3
S V Subramanian
7
S V Subramanian
8
So what?
• Economic residential segregation
• Crime and rising prison population
• Drag on economic growth
• Erosion of social cohesion
• Worse health status?
S V Subramanian
9
Income and health: a typology
• Absolute or Relative
• Individual or Community
S V Subramanian
10
Income and health: absolute and
individual interpretation
hi f ( yi )
• Where hi is an individual’s level of well-being (for
example, years of life), and yi refers to that
individual’s own level of income.
• The relationship between individual income and
individual health is concave, i.e., a $ increase is
accompanied by relatively small or even no
improvement in health, beyond a particular level
of income.
S V Subramanian
11
Concavity effect
y2
Health y1
x1
S V Subramanian
x2
x
Income
x3
x4
12
Income and health: relative and individual
interpretation
• Inspired by the concept of relative deprivation
formulated by Runciman (1966). It is “the extent of
the difference between the desired situation and
that of the person desiring it”.
• “…we can roughly say that A is relatively deprived
of X when (i) he does not have X, (ii) he sees some
other person or persons, which may include himself
at some previous or expected time, as having X
(whether or not this is or will be in fact the case), (iii)
he wants X, and (iv) he sees it as feasible that he
should have X.” (Runciman 1966) (p.10)”
S V Subramanian
13
Income and health: relative and individual
interpretation
hi f ( yi yr )
• Where health of an individual is a function of the
term (yi-yr ) that denotes the relative gap between
an individual’s income, yi, and the income of
some reference population, yr . The reference
population could be the income of co-workers,
neighbors, or the national population.
S V Subramanian
14
Income and health: absolute and
community interpretation
hij f (Y j , yij )
• Health of an individual i in community j is a
function of their own income (yij) AND the
average income levels of community (Yj) in which
the individuals reside.
S V Subramanian
15
Income and health: relative and
community interpretation
hij f ( I j , yij )
• Where Ij refers to a summary measure of
income distribution (e.g., Gini coefficient) for the
community in which the individual resides.
S V Subramanian
16
Pollution effect
Life expectancy
Effect of income redistribution
Income
S V Subramanian
17
Income inequality hypothesis:
intrinsically multilevel
hij f ( I j , yij , ( yij yrj ), Yij )
Health of an
individual in a
community
Community
Income
inequality
Individual
Absolute
income
Individual
Relative
income
Community
Absolute
income
For substantive and technical reasons, we need a
multilevel regression approach to estimate the above.
S V Subramanian
18
What does the evidence using multi-level
data-sets suggest?
S V Subramanian
19
Detectable patterns in US studies
• Positive studies
– US states
– Wide range of outcomes
– Larger samples
• Null studies
– US counties/metropolitan areas
– Smaller samples
S V Subramanian
20
Conditions
OR
95%CI
No individual income effect
1.32
(1.19-1.46)
Linear effect of income
1.31
(1.18-1.46)
Income transformed into log
1.30
(1.17-1.45)
Non-linear (2nd order polynomial)
1.31
(1.17-1.45)
Income as deciles
1.29
(1.15-1.43)
Income as quintiles
1.29
(1.16-1.44)
Income as categories
1.30
(1.17-1.45)
OR for Gini based on 0.05 (5%) change in Gini;
Note: All models additionally controlled for individual age, sex, marital status, race, years of
education, covered by health insurance and state median income.
*The equivalized household income categories were as follows: above $75,000: reference,
$50,000-75,000, $30,000-50,000, $15,000-30,000, below $15,000.
S V Subramanian
21
Conditions
OR
95%CI
Baseline
1.57
(1.39-1.78)
+ State median income
1.50
(1.34-1.67)
+ Age
1.53
(1.37-1.71)
+ Sex
1.52
(1.36-1.70)
+ Marital Status
1.51
(1.35-1.69)
+ Race
1.42
(1.27-1.57)
+ Years of Education
1.34
(1.21-1.48)
+ Equivalized household income
1.30
(1.17-1.45)
+ Health insurance
1.30
(1.17-1.45)
OR for Gini based on 0.05 (5%) change in Gini
S V Subramanian
22
Detectable patterns in non-US studies
• Mostly null, BUT
– ALL countries studied thus far are FAR more egalitarian
(Sweden, Denmark, Japan, UK) than the US
– ALL countries studied are also centralized states, thus raising
the issue related to the relevance of a chosen unit of aggregation
• Is US an exception; what about societies more unequal
than the US?
S V Subramanian
23
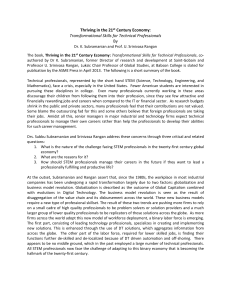
Income inequality and health in Chile
Odds Ratio for poor health
1.5
1.4
1.3
1.22
1.2
1.21
1.17
1.1
1
1
0.9
less than 0.4 (Reference)
0.4 to 0.45
0.45 to 0.50
0.50 and above
Com m unity Gini Coefficients
Source: Subramanian et.al., 2003
S V Subramanian
24
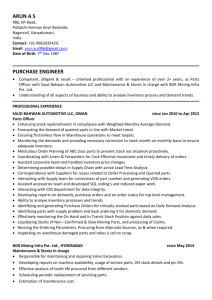
Income inequality and health in India
1.4
1.3
OR (95% CI)
1.2
1.19
1.11
1.1
1.1
1.05
1
1
0.9
<18.5
18.5-22.9
23-24.9
25-29.9
≥30
Body Mass Index
Source: Subramanian, Kawachi, Davey Smith (Unpublished)
S V Subramanian
25
Mechanisms linking income inequality
and health
•
•
•
S V Subramanian
Access to material resources
Relative comparisons
Social cohesion and social capital
26
Evidence for RD explanation?
• Defining reference groups using combinations of state,
race, education, and age, Eibner and Evans (2005) found
that high relative deprivation is associated with a higher
probability of death, self-reported limitations, body mass
index, risky health behaviors, and poor self-reported health.
– No association between state mean income and the
probability of death
– One standard deviation (0.022) increase in the Gini
coefficient is associated 8 percent increase in the
probability of death.
– Gini coefficient AND the relative deprivation measure
positively related to mortality, but RD attenuates the
coefficient associated with Gini.
Eibner CE, Evans WN. Relative deprivation, poor health habits and mortality. Journal of Human Resources. 2005;40(3):591-620.
S V Subramanian
27
For better or for worse the Gini is out of
the bottle….
If recent global and national economic trends
provide any indication, research on income
inequality and its potential effects on health will
probably be more, and not less, important.
S V Subramanian
28
FOR (in the US)
Authors, Year
Source: Subramanian, Kawachi, 2004
Sample population
Method
Kennedy et al., 1998
205245 adults from 50 U.S.
states
Marginal Models
Self-rated health
Soobader and LeClere,
1999
9,637 white males from U.S.
counties and tracts (n for counties
and tracts not reported)
Marginal models
Self-rated health
Blakely et al., 2000
279066 adults nested within 50
U.S. states
Multilevel models
Self-rated health
Diez-Roux et al., 2000
81,557 adults nested within 50
U.S. states
Multilevel models
Hypertension,
smoking,
sedentarism, body
mass index
Kahn et al., 2000
8285 women from 50 U.S. States
Marginal models
Depressive
symptoms, selfrated health
Lochner et al., 2001
546,888 adults from 50 U.S.
States
Marginal models
Mortality
Subramanian et al.,
2001
144692 adults nested within 39
U.S. states
Multilevel models
Self-rated health
Subramanian et al.,
2003
90,000 adults aged 45 and above
nested within 50 U.S. states
nested within 9 census divisions
Multilevel models
Self-rated health
Subramanian and
Kawachi, 2003
201221 adults nested within 50
U.S. states
Multilevel models
Self-rated health
S V Subramanian
Outcome
29
AGAINST (in the US)
Authors, Year
Sample population
Method
Outcome
Fiscella and Franks,
1997
14407 adults from U.S.
counties (n for counties not
reported)
Single-level
regression
Mortality
Daly et al., 1998
About 6500 adults from U.S.
states (n for states not
reported)
Single-level
regression
Mortality
Mellor and Milyo,
2002
309135 adults aged 25-74
from U.S. states and
metropolitan areas (n not
reported)
Marginal models
Self-rated health
Blakely et al., 2002
18547 respondents and
adults nested within 232 U.S.
metropolitan areas; and
216 counties
Multilevel models
Self-rated health
Sturm and Gresenz,
2002
8,235 adults from U.S.
metropolitan areas (n for
metropolitan areas not
reported)
Marginal models
Self-reports of 17 common
conditions (e.g., arthritis,
depression)
Mellor and Milyo,
2003
309135 adults aged 25-74
from U.S. states
Marginal models
Self-rated health
Source: Subramanian, Kawachi, 2004
S V Subramanian
30
Outside of the US
Author, Year
Sample population
Method
Outcome
Support for
income
inequality
hypothesis
Gerdtham and
Johannesson,
2001
40,000+ adults from
Municipalities in Sweden (n
for municipalities not
reported)
Marginal models
Mortality
No
Jones et al., 2004
8720 adults nested within
207 UK constituency nested
within 22 regions
Multilevel models
Mortality
No
Osler et al., 2002
25728 adults from parishes
within Copenhagen city (n
for parishes not reported)
Single level
regression
Mortality
No
Shibuya et al.,
2002
80899 adults from Japanese
prefectures (n for
prefectures not reported)
Marginal models
Self-rated
health
No
Blakely et al.,
2003
1391118 adults nested
within regions within New
Zealand (3 alternatives,
n=14, n=35, n=73)
Multilevel models
All-cause and
cause-specific
mortality
No
Subramanian et
al., 2003
98344 adults nested within
61978 households nested
within 285 Chilean
communities nested within
13 regions
Multilevel models
Self-rated
health
Yes
Source: Subramanian, Kawachi, 2004
S V Subramanian
31
Gini coefficient
• Most popular measure of inequality developed by the
Italian statistician Corrado Gini (1912).
• Typically used to measure income inequality, but can
be used to measure distribution on any space.
• The Gini coefficient is a number between 0 and 1,
where 0 corresponds with perfect equality (where
everyone has the same income) and 1 corresponds
with perfect inequality (where one person has all the
income, and everyone else has zero income).
• Algebraically, the Gini is defined as half of the
arithmetic average of the sum of the absolute
differences between all pairs of incomes in a
population, normalized to mean income.
S V Subramanian
32
Lorenz curve
• Developed by Max O Lorenz (1905) as a graphical representation of
income distribution.
• Portrays observed income distributions and compares this to a state
of perfect income equality.
• Graphical expression of verbal statements such as, "the bottom
twenty percent of all households have ten percent of the total
income“.
• Shows, for the bottom x% of households, the percentage y% of the
total income which they have. Typically, the percentage of
households is plotted on the x-axis, the percentage of income on the
y-axis.
• The Lorenz curve is used to calculate the Gini coefficient.
S V Subramanian
33
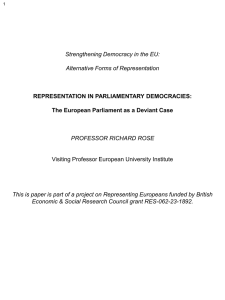
Lorenz & Gini
Ratio of the area between
the line of perfect equality
and Lorenz curve is {A},
and the area underneath
the Lorenz curve {B}.
Expressed as a
percentage or as the
numerical equivalent of
that percentage, which is
always a number
between 0 and 1.
{A}
{B}
Gini index =
A/(A+B)
S V Subramanian
34