Blood, part 3
advertisement

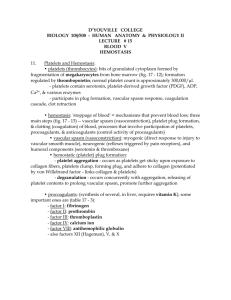
Blood, part 3 Thrombocytes, Hemostasis, Hemostatic Disorders, Blood Typing and Transfusions Thrombocytes (platelets) • Not true cells • Cytoplasmic fragments w/purple granules that contain chemicals for blood clotting Activated platelet – Enzymes amorphous – Serotonin w/extensions that help them stick to vessels – Ca2+ ions and each other – ADP – PDGF (Platelet-derived Growth Factor) • Normally kept in “inactive” state by molecules secreted by endothelial cells of blood vessels • When activated, form temporary plug that helps to seal breaks in blood vessels Thrombopoiesis (Platelet formation) • Cytoplasmic fragments derived from megakaryocytes – Mega = large – Karyo = nuclei – Cyte = mature cell • Thrombopoietin promotes formation of megakaryocyte, created by multiple mitosis w/o cytokinesis • Megakaryocyte presses against sinusoid (capillary) of bone marrow and pinches off to make fragments Hemostasis • Series of reactions to stop a bleed • Phases: 1. 2. 3. 4. 5. Vascular spasm Platelet plug Coagulation (clotting) Clot Retraction Fibrinolysis (Clot Eradication) 1. Vascular Spasm 1. Vascular Spasm • Constriction of damaged vessel, triggered by: - Endothelium - platelets - Pain receptors • Slows the bleed 2. Platelet Plug Formation • Damaged endothelium activate platelets by releasing – VWF (von Willebrand Factor) • Platelets become amorphous: – Stick to exposed collagen fibers of endothelium – Release • serotonin ( spasms) • ADP (attract more platelets) • Thromboxane ( both ) • Prostacyclin (inhibits aggregation elsewhere) 3. Coagulation (Blood Clotting) • Blood transformed from liquid to gel • 3 Critical Steps: 1. Prothrombin Activator Forms (complex series of biochemical rxns!) - require Ca2+ ion and procoagulants to promote sequence of rxns - Two pathways: a. Intrinsic Pathways (slower) – within damaged vessel b. Extrinsic Pathway (faster) – outer tissue around vessel 2. Prothrombin converted to Thrombin 3. Thrombin catalyzes joining of fibrinogen into fibrin mesh - Glue platelets together 4. Clot Retraction • Clot Retraction – Platelets contract (like a muscle) to stabilize clot • Contractions pulls on fibrin squeeze out serum from clot Compact the clot Ruptured ends of blood vessel drawn closer together – PDGF and VEGF released from platelets • (PDGF) Stimulates fibroblast and smooth muscle mitosis to rebuild wall • (VEGF) Promotes endothelial restoration 5. Fibrinolysis • tPA (Tissue Plasminogen Activator) – Released by endothelium around clot – Activates plasminogen – Plasminogen plasmin • Plasmin – Digestive “clot busting” enzyme • Remnants of clot phagocytized by WBCs – Macrophages – eosinophils How are clots prevented from becoming TOO large? 1. Fast moving blood – Washes away excess Thrombin 2. Inhibition of clotting factors – Anti-thrombin III (ATIII): plasma protein inactivates thrombin – Protein C: inhibits clotting factors – Heparin: enhances ATIII Hemostatic Disorders: Undesirable Clotting • Thrombus: a clot that develops in an unbroken vessel – blocks circulation tissue death – Coronary thrombosis Heart attack Death of cardiac muscle Hemostatic Disorders: Undesirable Clotting • Embolus: freely floating thrombus in bloodstream – Pulmonary Embolism • Impairs O2 delivery • Death of lung tissue – Cerebral Embolism • Stroke, • Death of brain tissue Hemostatic Disorders: Undesirable Bleeding Thrombocytopenia • reduced platelet count < 50,000/mm3 – Bone marrow disease or destruction • petechiae on skin due to widespread hemorrhage • Treatment: blood transfusions Hemostatic Disorders: Undesirable Bleeding Hemophilia: • Hereditary • Lack of clotting factors – hp A - defective Factor VIII (83%) – hp B - defective Factor IX (10%) • Genentech. Inc. - now engineers tPA and Factor VIII less transfusions needed Human Blood Groups • glycoprotein antigens exist on external surfaces of RBCs • Antigens are: – Unique to the individual – “foreign” to other individuals – promotes agglutination • Presence or absence of these antigens is used to classify blood groups Blood Typing • anti-A or anti-B antibody serums are added to blood • agglutination occurs between the antibody and the corresponding antigens Blood Donors and Recipients Blood Type Antigen Serum Antibody A A Anti-B A and AB A and O B B Anti-A B and AB B and O AB O Donate To A and B None AB only None Anti-A Anti-B All Types Receive From All Types O only Rh Blood Groups • Rh antigens: – 8 types – Most common: types C, D, and E • Anti-Rh antibodies do not exist in Rhindividuals until they are exposed to Rh+ blood (1st pregnancy) • Leads to complications during 2nd pregnancies, if Rh- mother is carrying Rh+ child Transfusions • Blood bank: – – – – Mix donor blood with anticoagulants that bind to Ca2+ Tested for viruses, ABO, and Rh factor 35 day shelf life at 40 C Blood separated into component parts • Whole blood: (rare) – Only for rapid and substantial blood loss • Packed red cells (plasma removed) – To restore O2 carrying capacity Transfusion Reactions • Occur when mismatched blood is infused • Donor’s blood cells are attacked by the recipient’s plasma antibodies causing: – – – – – Ruptured RBCs Diminished O2 carrying capacity Clumped cells (agglutination) Blood clots “Free” hemoglobin due to lysis of RBC • Hemoglobin solidifies in kidneys – Kidney fails