Legal Issues in Pain Medicine

Utilization of the Emergency Department by
Chronic Pain Patients to Obtain Pain
Medications:
A Study of Barriers to Treatment, Abusive
Behaviors and Psychological Factors
• Scott M. Fishman, MD
Chief: Div. of Pain Medicine
Dept. of Anesthesia &
Pain Medicine
UC Davis Medical Center
Professor of Anesthesiology
Univ. of California, Davis
School of Medicine
Background
• Mayday Foundation RFP
• ED paper
» Literature review
~ Chronic pain evaluation
• LBP
• Headaches
• Sickle Cell
• Ureterolithiasis
Wilsey, Fishman, Rose, Papazian, Pain management in the ED. Am J Emerg Med 2004; 22: 51-7
Barriers to Treatment
• Quantitative data
» Questionnaires
~ Patients
~ Physicians
~ Nursing staff
• Qualitative analysis
» Interviews
~ On perceived barriers to care in the ED from the perspective of physicians
Utilization of the Emergency
Department by Chronic Pain
Patients to Obtain Pain
Medications: A Study of Barriers to Treatment, Abusive Behaviors and Psychological Factors
Scott Fishman, MD, Barth Wilsey, MD,
Ingela Symreng, PhD, Dan Mungas, PhD,
Christine Ogden, BS
Overview
• Study Structure
• Method of Recruitment
• Selected Population
~ Patient Demographics
•
~ Provider Demographics
• Status of Recruited Patients
Successful and Failed Recruitment
Techniques
Study Structure
Visit 1
•
•
Subject recruited while they are in the ED to be treated for chronic pain, duration
6 months
»
»
Fill out as many questionnaires as possible
~ Demographics, CAGE and Compton/Jameson Questionnaires
I-S.O.A.P., C.M.S.D., P.B.Q., PDQ-4+, C.S.Q.,
C.P.S.S., S.E.F., S.E.O.S., STAI, and BDI-II
Subject given contact information
» Advised of a F/U appointment with the psychologist
~ Scheduled within 14 days after the ED visit
Study Structure
Visit 2
•
•
Subject contacted within one week of ED Visit to schedule a F/U visit with psychologist
»
»
If all questionnaires are not complete
~ Opportunity at time of F/U visit to complete all questionnaires
The patient will meet with the psychologist for the
S.C.I.D.
» After meeting with the psychologist, the patient is informed about payment for participation
Completed Subject
» A set of complete questionnaires, BDI-II, and S.C.I.D. evaluation
•
•
Method of Recruitment –
Academic Offices
Ability to view the ED “Whiteboard” via remote computer in our
Academic Offices enables remote screening
» Research Assistants can utilize computers to look for patients who complain of the following generalized symptoms:
~ Chronic or Mild Stable Pain
~ Chronic Back Pain
~ Headache
~ Earache
~ Rx Refill Request
~ Diffuse Body Pain
~ Vague Abdominal Pain
Students travel to the ED to recruit these identified subjects
Method of Recruitment – ED
•
•
Students within the ED have significant access
»
Electronic “Whiteboard”, patient charts, and physical
“Whiteboard”
» Patients recruited using the inclusion/exclusion criteria designated by the protocol
Students approach patients within different Areas, including the waiting room, where they will proceed through the following steps:
»
»
»
»
Brief introduction to the study
Informed Consent
Administration of Study Questionnaires
Collection of all study materials before student and/or patient departs from the ED
Continued Contact
Post ED Visit
• A Research Assistant will contact subject via telephone within 1 week of the initial ED visit
» At this time, the subject is scheduled to complete
Visit 2 within 14 days of the initial ED visit
» The subject is contacted by telephone up to three times before the patient will be discontinued due to lack of compliance
Subject Selection
•
•
•
•
•
Inclusion Criteria
Male/Female
18 yrs of age
Patient is being seen at the University of California Davis ED for Schedule II medications
Patient has had pain for 6 months or longer prior to enrollment for which schedule II medications are already being prescribed
Patient presents to the ED with a complaint of vague head, abdomen, or back pain of nonacute onset, diffuse body paint, etc
Patient is able to read, understand, and voluntarily sign the approved informed consent form prior to the performance of any study specific procedures
•
•
•
•
Exclusion Criteria
Patient arrived by ambulance
Patient has an emergency medical condition
Patient states that they are not comfortable reading and comprehending
English
Patient is unwilling or unable to comply with the study visit schedule
15
10
5
0
30
25
20
50
45
40
35
Patient Demographics:
Gender
Female
Male n = 77
44
33
35
30
25
20
15
10
5
0
50
45
40
1
< 3 mo
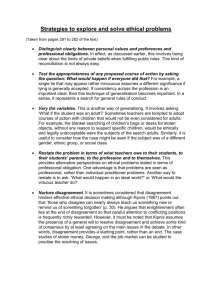
Patient Demographics:
Duration of Chronic Pain
5
8
17
3-6 mo 6mo-1yr
Duration of Pain
1-5yr n = 76
45
5+ yrs
Patient Demographics:
Ethnicity
40
35
30
25
20
15
10
5
0
35
White
28 n = 83
10
9
Black
1
0
American Indian Alaskan Native Asian or Pacific
Islander
Hispanic
Patient Demographics:
Annual Income n = 70
35
30
25
20
15
33
16
10
5
0
7 7
3 3
1
0
< 10,000 10,001-20,000 20,001-30,000 30,001-40,000 40,001-50,000 50,001-60,000 60,001-70,000 70,001+
Dollars
Patient Demographics:
Education
30
25
20
15
25
10
5
0
High School
8
24
14 n = 73
GED Some College Graduated college
1
Masters
1
Advanced Degree
60
50
40
30
20
10
0
Patient Demographics:
Employment
Employed
Not Employed n = 73
55
18
Types of Employment
• Currently Employed : Line of Work
~ Building Maintenance
~ Scrub Technician
~ Construction
~ Testing Technician
~ Stock Worker
~ Telemarketer
~ Editor
~ Housekeeper
~ Receptionist
~ Physical Therapist
~ Luggage Handler
~ Drug and Alcohol Counselor
~ Customer Service Clerk
~ Environmental Manager
~ Wildland Firefighter
~ Mental Health Worker
~ Writer
~ Cable
~ Truck Driver
~ Musician
• Currently Unemployed: Longest Employment
~ Fence Builder
~ Presser/Dry Cleaner
~ Retail Management
~ Cable
~ Dock worker
~ Contractor
~ Engineering Technician
~ Insurance
~ Figure Skater
~ Analytical Chemistry
~ Housekeeping
~ Janitor
~ Painter
~ Roofing
~ Asst. Supervisor for Distrib.
~ Lumberjack
~ Homemaker ~ Homemaker
~ Nursery Employee ~ Truck Driver
~ Underground Construction ~ Cashier
~ Limousine Company
~ Restaurant Work
~ Army
~ Cook
~ Bakery Machine Operator ~ Healthcare Research
~ Fast Food Customer Service ~ Cabinet Worker
~ Warehouse Worker
~ Operating Engineer Miner
~ Office Furniture Installer
~ Mental Health Case Mgr.
~ Accounting
~ Sales
~
~
~
~
~
Plumbing/Electrical
Computer Programmer
Mechanic
Welder/Fabricator
In House Security
Provider Demographics
25
20
15
10
5
0
40
35
30
14
Attending
Provider Demographics:
Different Providers
36 n = 56
5
Resident Nurse
1
Nursing Student
26
25.5
25
24.5
24
23.5
28.5
28
27.5
27
26.5
Provider Demographics:
Gender
28
Male
Female n = 53
25
Provider Demographics:
Ethnicity
30
25
20
15
10
5
0
45
40
35
41
White
1
Black n = 48
2
Asian
2
Hispanic
0
Indian
2
Other
Status of Study Subjects
Completers vs. Non-Completers
60
50
40
30
20
10
0
Completers vs. Non-Completers n = 90
51
39
Completers Non Completers
Non-Completers:
• Patients have or have not completed some portion of the questionnaires. They have NOT completed the S.C.I.D.
• Total: 51/90 = 56%
------------------------------------------------------------------
No Information Collected : 2
CAGE Only : 1
Dem* , CAGE : 13
Dem , CAGE , C\J** : 11
* Dem = Demographics
**C\J = Compton\Jameson
Dem , CAGE , C\J , I-S.O.A.P. : 2
Dem , CAGE , C\J , I-S.O.A.P., CMSD : 1
Dem , CAGE , C\J , I-S.O.A.P., CMSD , PBQ, STAI : 1
Dem , CAGE , C\J , I-S.O.A.P., CMSD , PBQ , PDQ-4+ : 1
Dem , CAGE , C\J , I-S.O.A.P., CMSD , PBQ , PDQ-4+, BDI-II : 2
Dem , CAGE , C\J , I-S.O.A.P., CMSD , PBQ , PDQ-4+, CSQ : 1
Dem , CAGE , C\J , I-S.O.A.P., CMSD , PBQ , PDQ-4+, CSQ , CPSS , SEF , SEOS : 1
Dem , CAGE , C\J , I-S.O.A.P., CMSD , PBQ , PDQ-4+, CSQ , CPSS , SEF , SEOS , STAI : 8
Dem , CAGE , C\J , I-S.O.A.P., CMSD , PBQ , PDQ-4+, CSQ , CPSS , SEF , SEOS , STAI , BDI-II : 7
Completers:
Patients have completed all necessary questionnaires AND the S.C.I.D.
Total: 39/90 = 43%
----------------------------------------------------------------------------------------
Dem , CAGE , C\J , I-S.O.A.P.,
CMSD , PBQ , PDQ-4+, CSQ ,
CPSS , SEF , SEOS , STAI , BDI-II ,
S.C.I.D. : 39
Summary of Recruitment
Successful Strategies and Barriers
Recruitment
• Useful Recruitment Strategies
~
Presence of recruiter in the ED between the hours of 11am-8pm
M-F (five day coverage to maximize patient recruitment)
~ Patient completion of BDI-II along with as many questionnaires as possible within the ED
• Barriers to Recruitment
~
2 nd Visit does not receive as much of a response from patients
~ 2 nd visit can only be completed on Fridays
~ Excluding patients who arrive by ambulance: Some chronic pain patients, utilize the ambulance to “get a ride” to the
ED.
~ 14 day interval between visits is too small
Quantitative Study of Barriers
• Questionnaire for
Patients &
Providers
» Same questions
~ Framed differently
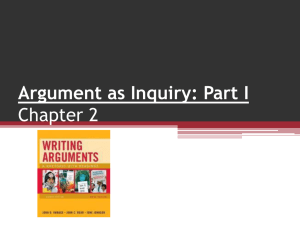
Lack of Time
•
• Patient
I do not have adequate time to assess and treat
ED patients complaining of chronic pain
•
• Provider
Doctors and nurses avoid spending enough time to talk about your chronic pain
5
4
3
2
1
0
] nurse n=37
]
Strong agreement
Moderate agreement
Some agreement
]
Some disagreement
Moderate disagreement patient n=54 lack of time physician n=19
Strongly disagreement
Dunnett t-test post-hoc ns patient vs physician .113
sig patient vs nurse .003
Prioritization
•
• Provider
The treatment of chronic pain in the ED takes a back seat to treatment of more pressing issues like trauma or myocardial infarctions
•
• Patient
Doctors and nurses have more pressing issues than chronic pain
(like seeing injured people or those with heart attacks)
5
4
3
2
1
0
] ]
Strong agreement
Moderate agreement
]
Some agreement
Some disagreement
Moderate disagreement nurse patient physician n=37 n=54 n=19 more pressing issues
Strongly disagreement
Dunnett t-test post-hoc ns patient vs physician .184
ns patient vs nurse .075
Fatalism
•
• Provider
Chronic pain has little chance of improving
•
• Patient
Chronic pain has little chance of improving
5
4
Strong agreement
Moderate agreement
]
3
2
1
]
]
Some agreement
Some disagreement
Moderate disagreement
0 patient physician nurse n=37 n=54 n=19
Little Chance of Improving
Strongly disagreement
Dunnett t-test post-hoc sig patient vs physician .001
sig patient vs nurse <.001
Belief in Pathology
•
• Provider
I do not believe the validity of a pain complaint in the absence of physical findings or a lack of objective findings on imaging studies, EMG, etc
•
• Patient
When the doctor cannot find something wrong on exam or by an
X-ray, they tend not to believe you could be in pain
5
4
Strong agreement
Moderate agreement
]
3 Some agreement
2
1
0
Some disagreement
] Moderate disagreement
] patient physician nurse n=37 n=54 n=19
Belief in Pathology
Strongly disagreement
Dunnett t-test post-hoc sig patient vs physician .001
sig patient vs nurse <.001
Fear of Addiction
•
• Provider
I believe that chronic pain patients who come to the ED are addicted to their pain medications
•
• Patient
I think that I am addicted to pain medications
5
4
Strong agreement
Moderate agreement
3
2
]
]
Some agreement
Some disagreement
1
0
Moderate disagreement
] patient physician nurse n=37 n=54 n=19
Fear of Addiction
Strongly disagreement
Dunnett t-test post-hoc sig patient vs physician .003
sig patient vs nurse .001
Fear of Dependence
• Provider
I avoid administering opioids because patients will develop physical dependence and go through withdrawal when they abruptly halt the intake of the medicine
• Patient
I avoid taking pain medications because taking them will lead to withdrawal symptoms if I have to stop them
5
4
Strong agreement
Moderate agreement
3
2
]
Some agreement
Some disagreement
1
0
Moderate disagreement
]
] patient physician nurse n=37 n=54 n=19
Fear of Dependence
Strongly disagreement
Dunnett t-test post-hoc sig patient vs physician .018
sig patient vs nurse <.001
“Bad” Patient
• Provider
I find myself labeling chronic pain patients as
“bad patients” or
“drug seekers”
• Patient
I believe that telling doctors and nurses about my pain leads them to consider me to be a “bad patient” or a
“drug seeker”
5
4
Strong agreement
Moderate agreement
3
2
1
]
]
]
Some agreement
Some disagreement
Moderate disagreement
0 patient physician nurse n=37 n=54 n=19
“Drug Seeker”
Strongly disagreement
Dunnett t-test post-hoc ns patient vs physician .108
ns patient vs nurse .313
Qualitative Research
Through Interviews
•
•
Access using conversations and consultations with
ED physicians
Taped and transcribed interviews
» Anonymity and confidentiality maintained
Qualitative Research
• Questions
» Most problematic chronic pain patient
» Limitations on care
» Potential sources of improvement
Qualitative Research
• Responses
»
“ED not designed to see these patients”
»
»
“Appropriate referrals to pain specialists difficult”
Advised patients “find a primary care doctor”
» Provide short acting opioids
~ 20-30 pills of vicodin, codeine, or oxycodone
Estimated Numbers (in Millions) of Lifetime Nonmedical Use of Selected Pain Relievers among Persons Aged 12 or Older: 2002 http://oas.samhsa.gov/2k4/pain/pain.htm
Abusive Behaviors
Estimated Numbers (in Millions) of Persons Aged 12 or Older with Past Year Illicit Drug
Dependence or Abuse, by Drug: 2002 http://oas.samhsa.gov/2k4/pain/pain.htm\
Prescription Drug Abuse in ED
» Modeling using multiple regression
~ Dependent variable
• Screener and Opioid Assessment for Patients in Pain (SOAPP)
~ Independent variable
• Spielberger State-Trait Anxiety Inventory (STAI)
• Beck Depression Inventory (BDI-II)
• Chronic Pain Self-Efficacy Scale (CPSS)
• Coping Strategies Questionnaire (CSQ)
Screener and Opioid Assessment for Patients in Pain (SOAPP)
•
•
Unrestricted grant from Endo
Pharmaceuticals Inc.
Inflexxion, Newton, MA
» Concept mapping procedures to obtain input from a panel of pain and addiction medicine specialists
~ Predict which patients will require more or less monitoring on longterm opioid therapy http:/www.painedu.org.
Screener and Opioid Assessment for Patients in Pain (SOAPP)
~ Prescription Drug Use Questionnaire (PDUQ)
~ Judgement by two out of the three staff member groups (e.g., using a physician, nurse, and/or a receptionist) that the patient had a serious drug problem
~ Urine toxicology screening
Compton PJ, Darakjian J, Miotto K. Screening for addiction in patients with chronic pain and
"problematic" substance use: evaluation of a pilot assessment tool. J Pain Symptom Manage
1998;16:355-63.
Katz NP, Sherburne S, Beach M, Rose RJ, Vielguth J, Bradley J, et al. Behavioral monitoring and urine toxicology testing in patients receiving long-term opioid therapy. Anesth Analg
2003;97(4):1097-102, table of contents.
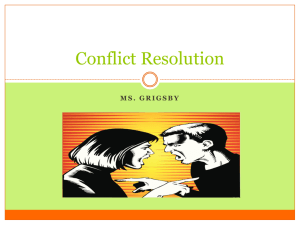
Predicting Aberrant Medication-
Related Behavior
•
•
•
A cutoff score of 8 was chosen to produce a sensitive test
Sensitivity of .90
» Correctly classified 90% of the patients who actually went on to exhibit aberrant behaviors
Specificity of .69
» 31% of the people, who scored an 8 or higher on the
SOAPP, did not go on to show detectable aberrant behavior
6
4
2
14
12
10
8
0
5 10 15 20 25 30 35
SOAPP Version 1.0 Summary Score
40 45
Mean = 19.06
SD = 8.258
N = 47
Unexpected Finding
• Biased population
» Poorly controlled
» Prescription drug abuse relatively common in ED setting
~ Short acting opioids
~ No opioid contracting
~ Multiple prescribers
• Instrument not valid in ED
Abusive Behaviors and
Psychological Factors
• Prescription drug abuse will correlate with psychological factors
» Previous study in pain clinics not confirmatory
~
“ Psychosocial testing on clinic admission failed to predict who would become an opiate abuser”
Chabal C, Erjavec MK, Jacobson L, Mariano A, Chaney E. Prescription opiate abuse in chronic pain patients: clinical criteria, incidence, and predictors. Clin J Pain 1997;13(2):150-5.
Correlates
• Self Efficacy for Coping with
Symptoms
Screening for Prescription
Drug Abuse in ED
3 or 4 simple questions
Prescription Drug Use
Questionnaire
•
•
•
I believe that I am addicted to pain medicine
I routinely have to take more medication than my doctor prescribes in order to treat my pain
I prefer certain pain medications or ways of taking these medications (IV, IM routes over the oral route)
Compton PJ, Darakjian J, Miotto K. Screening for addiction in patients with chronic pain and
"problematic" substance use: evaluation of a pilot assessment tool. J Pain Symptom Manage
1998;16:355-63.
3
2.5
2
1.5
1
0.5
0
10 20 30 iSOAPP Score
40 n = 47
Spearman rho r = 0.223
p = 0.131
2-tailed
CAGE
• Have you ever felt the need to
C ut down on your use of prescription drugs?
• Have you ever felt
A nnoyed by remarks your friends or loved ones made about your use of prescription drugs?
• Have you ever felt
G uilty or remorseful about your use of prescription drugs?
• Have you
E ver used prescription drugs as a way to "get going" or to "calm down?" http://www.nida.nih.gov/ResearchReports/Prescription/prescription6.html#Providers
4
3
2
1
0
10 20 30 iSOAPP Score
40 n = 45
Spearman rho r = 0.322
p = 0.031
2-tailed
Hx Addiction/Legal Issues
•
•
•
Is there a history of alcohol or substance abuse in your family, even among your grandparents, aunts, or uncles?
Have you ever had a problem with drugs or alcohol or attended Alcoholics Anonymous (AA) or Narcotics Anonymous (NA) meetings?
Have you ever had any legal problems or been charged with driving while intoxicated (DWI) or driving under the influence (DUI)?
Michna E, Ross EL, Hynes WL, Nedeljkovic SS, Soumekh S, Janfaza D, et al. Predicting aberrant drug behavior in patients treated for chronic pain: importance of abuse history. J Pain Symptom
Manage 2004;28(3):250-8.
3
2.5
2
1.5
1
0.5
0
10 20 30 iSOAPP Score
40 n = 45
Spearman rho r = 0.418
p = 0.005
2-tailed
Conclusions
•
•
•
Barriers are present
» Similar to other settings
Chronic pain patients seeking care in
ED are special population
» Prescription drug abuse
~ More research needed
Short questionnaire for prescription drug abuse
» No definitive answer
Collaborators
•
•
•
•
•
Barth Wilsey MD
Ingela Symreng PhD
Amy Ernst MD
Dan Mungas PhD
Matt Lewis BS, Jeanna Millman BS, &
Christine Ogden BS