GERD IN THE
ST
21
CENTURY:
More than just a spoonful of sugar
UPMASA A G C
July 2015
DAVID ESTORES, MD
David.Estores@medicine.ufl.edu
Learning Objectives
Become familiar with:
• Pathophysiology of GERD
– Acid pocket
– Belts
• Evolution of the definition of GERD
• Symptoms of GERD
– Definitions
– Ability of symptoms to predict GERD
Learning Objectives (2)
Become familiar with:
• Use of PPI Test in GERD
– Definition
– Test characteristics
• pH and Impedance testing
• Patient with GERD Best candidate for
surgery
40 yr old male with reflux
• For the past 3 months
• Takes a standard dose of PPI BID
• Reflux symptoms immediately after a
meal
• Relief with antacids
Does this even make sense?
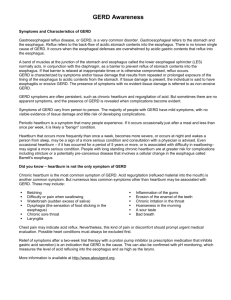
The Acid Pocket The Acid Raft
ACID POCKET
STOMACH
ESOPHAGUS
Fletcher et al. Gastro 2001
NORMAL/CONTROL
LARGE HIATAL HERNIA
Acid Pocket (Beaumont et al.)
52 yr old man walks into
your office
• Worsening heartburn for the past 2
years
• Unresponsive to once a day PPI
• Had an endoscopy (Normal)
• Weight gain of 20 lbs
Belts and reflux (Lee et al.)
• 16 Patients (8 obese and 8 non-obese)
• Test meal = french fries and battered fish
• Application of “belt”
– Nike weight belt
– Standard blood pressure cuff inflated to have a
constant pressure of 50 mmHg
Lee Gut 2013
• SCJ = squamocolumnar
junction
• HPZ = high pressure zone
• PIP = Pressure inversion
point (separates the
intrathoracic LES from
the intraabdominal LES)
• pLOS (pLES) = Peak LES
pressure (apex of
triangle
E
S
O
P
H
A
G
U
S
S
T
O
M
A
C
H
Postprandial Effects of a Belt
Lee et al Gut 2013
John D. (78 y.o. man)
• Retired university faculty member
• Stated that “you have to do something about
my heartburn due to GERD”– for 20+ years
• Points to his epigastrium
• Pain is NOT associated with meals
• <25% relief with PPIs (BID)
• Undergone an extensive work-up
Jane D. (52 y.o. woman)
• University faculty member
• Substernal burning pain for over 10 years
– Mostly post-prandial
– No relief with PPI (BID)
• Subsequently underwent extensive work-up
History of the Definition of
GERD
Montreal definition, 2006
GERD SPECTRUM PYRAMID
ENDOSCOPY -, pH +
ENDOSCOPY +
Vaezi M, et al GI and Hepatology 2003
RESPONSE RATE DATA ON RCT’S (ACID SUPPRESSION)
Practical Manual of GERD- Eds. Vela, Richter, Pandolfino 2013
Practical Manual of GERD- Eds. Vela, Richter, Pandolfino 2013
Why is symptom evaluation in
GERD important?
•
•
•
•
•
Make the initial diagnosis
Assess the severity of disease
Formulate a diagnostic work-up
And/or starts treatment
Assess the response to treatment
SYMPTOMS ARE WHAT MATTERS MOST!!!
HRQL dimensions (assessed by SF-36) in German patients with
GERD vs. general population
Managing GERD in Primary Care: The Patient Perspective
Kullig et al. Alimen Pharm Therap 2003
Spectrum of GERD
• Normal GE reflux
• When does GER become GERD?
• What is the gold standard??
Definition of heartburn and
regurgitation
• Heartburn - burning retrosternal painful
sensation of short duration associated with a
meal
• Regurgitation - the retrograde flow of
presumed gastric contents or sensation of
bitter contents in the mouth without
associated nausea or retching
John D. (78 y.o. man)
• Retired university faculty member
• Stated that “you have to do something about
my heartburn due to GERD”– for 20+ years
• Points to his epigastrium
• Pain is NOT associated with meals
• <25% relief with PPIs (BID)
• Underwent an extensive work-up
Jane D. (52 y.o. woman)
• University faculty member
• Substernal burning pain for over 10 years
– Mostly post-prandial
– No relief with PPI (BID)
• Subsequently underwent extensive work-up
What GERD associated HB is not!
• Dyspepsia (epigastric discomfort)
– Uninvestigated dyspepsia
• NSAIDs
• H. pylori
– Functional dyspepsia after testing/ endoscopy
negative Professor John D
• Functional heartburn Professor Jane D
Functional dyspepsia
• The most common form of dyspepsia
presenting to primary care physicians and
gastroenterologists
• Approach to diagnosis
•
Jaundice
Gillen and McColl Medicine 2010
FUNCTIONAL HEARTBURN
Zerbib et al. Curr Gastroenterol Rep (2012)
Zerbib et al. Curr Gastroenterol Rep (2012)
HOW COMMON IS FUNCTIONAL HEARTBURN?
NERD = 60 to 75%
Fass & Tougat
Gut 2002
Rome
III
ROUGHLY 1 IN
5 PATIENTS
PRESENTING
WITH
HEARTBURN
INTERESTING NUMBERS!!!
• Heartburn is NOT well understood (65.9%)
– % who understood (35% W, 54% B, 13% A)
• 29.7% did not describe symptoms that a
reasonable clinician would define as
heartburn
• 22.8% of patients who denied having
heartburn in fact experienced symptoms that
physicians might consider to be heartburn
Spechler et al Aliment Pharmacol Tx 2002
Diagnosis - GERD in PC setting based on
symptoms / PPI test
Dent J et al. Gut 2010;59:714-721
Copyright © BMJ Publishing Group Ltd & British Society of Gastroenterology. All rights reserved.
Sensitivity and specificity
• Based on data from the Diamond study
• HB or regurgitation as the most troublesome symptom
overall sensitivity of 49% with a specificity of 74%.
• If either HB or regurgitation is the most or second most
troublesome symptom, the sensitivity is increased to
69% accompanied by an expected decrease in
specificity to 62%.
• (Sens/Spec) Marginally higher among
gastroenterologists at 67%/70% vs. family practitioners
at 63%/63%.
The PPI test in GERD diagnosis
Lack of consensus
•
•
•
•
What PPI to use?
Dosage of the PPI? QD or BID?
How long do we use it?
Definition of treatment response?
– Complete
– Partial
Estores GICNA 2014
Proportion of patients with relief of reflux symptoms
in response to PPI day by day.
Bytzer, et al. Clin Gastro Hep 2012
Sensitivity/Specificity for the PPI
Test – Dx of GERD
• Meta analysis by Numans (Ann Int Med 2004)
– sensitivity of 78% (95% CI = 66 to 86)
– specificity of 54% (95% CI = 44 to 65)
• Bytzer et al re-analyzed Diamond study data
– positive PPI test in 69% of patients with GERD
(confirmed by pH and/or esophagitis on
endoscopy) compared to 51% of patients without
GERD
Clin Gastro Hep 2012
Why use the PPI test in GERD dx?
• Convenient
• Cost effective
• A positive response is a positive
response, no matter what the primary
diagnosis is!
Estores GICNA 2014
Impedance
pH
Bravo pH
24 hours
48 hours
Wires in use
Yes
No
Information about Non-acid reflux
Yes
No
Requires Esophageal Manometry for
placement
Yes
No
Valid for atypical symptoms
NO
NO
Direction of reflux
Yes
NO
Requires an endoscopy
No
YES
Length of study
RESPONSE RATE DATA ON RCT’S
(ACID SUPPRESSION)
Practical Manual of GERD- Eds. Vela, Richter, Pandolfino 2013
Best patient to send to a surgeon?
• Progressive damage demonstrated/physiology
– Esophagitis
– Hiatal hernia
– Regurgitation
– Nocturnal
• Abnormal acid exposure time
• Some response to PPI
Take Home Points
• Implications of acid pocket
– Use of antacids with alginate
– Not all patients will have relief from PPIs
•
•
•
•
•
Loosen belts or switch to suspenders
Symptom definition and accuracy of history
Sensitivity and specificity for symptoms alone
Use of the PPI test for diagnosis of GERD
Approach to GERD in primary care setting
Take home points
• Diagnosis of GERD = clinical + endoscopy + pH testing
– NO further w/u (do not need endoscopy/ pH testing)
• Classic symptoms
• Relief w/ PPIs
• NO Red flags
• Utility of a PPI test = 2 weeks, BID
• Testing for GERD
– pH Monitoring (pros and cons)
• pH Impedance
• Bravo wireless
Take home points
• Treatment
– Typical vs atypical
– Esophagitis
• Surgery
– Exclude achalasia
– Patients with esophagitis
– Large hiatal hernias
– Medical co-morbidities