Health care is complex: its issues are complicated and solutions in some cases are not clear —
as the 2012 election nears, health reform takes center stage
Dr. Paul Keckley, Executive Director for the Deloitte Center for Health Solutions
shares ten myths about the health reform debate
1
Most Americans like our current system.
They want the current system protected at all costs.
Facts:
• The majority of Americans think the current system is inefficient,
expensive, and wasteful
• The public is increasingly concerned about its costs
• Our polls say the public wants to see the system fixed using
technologies that increase efficiency, reduce error, and expand the role
of nurses and pharmacists in the delivery of care
Source: 2012 Deloitte Survey of U.S. Health Care Consumers
Copyright © 2012 Deloitte Development LLC. All rights reserved.
1
Our studies say that 69% of Americans think fraud
and abuse in the payment system contribute to
waste.
Percent who believe each source contributes to waste in health care system
Fraud and abuse in the payment/reimbursement system
69%
Individuals not taking enough responsibility for their own health
and leading unhealthy lifestyles
49%
Duplication of tests and procedures because physicians don’t
share patient health information
38%
Unnecessary paperwork
34%
Doctors providing more services than necessary and/or refusing
to treat high risk patients to avoid possibly being sued
34%
Over-regulation of the health care industry
Taking extreme measures to extend life when there is little hope
of recovering and returning to a meaningful life
Doctors performing tests and procedures outside evidencebased guidelines
Source: 2012 Deloitte Survey of U.S. Health Care Consumers
30%
20%
18%
Copyright © 2012 Deloitte Development LLC. All rights reserved.
1
34% of individuals making $100k or more annually feel
financially prepared to handle future health care costs
compared to 13% of families making less than $100k.
Percent of individuals who feel financially prepared to handle future health care costs, 2009-2012
50%
40%
40%
42%
43%
34%
30%
20%
20%
15%
18%
13%
10%
0%
2009
2010
2011
2012
Annual income of $100,000 or higher
Source: 2009-2012 Deloitte Survey of U.S. Health Care Consumers
2009
2010
2011
2012
Annual income of less than $100,000
Copyright © 2012 Deloitte Development LLC. All rights reserved.
2
Most Americans understand the U.S. system
and think it’s better than others.
Facts:
• Most Americans do not understand and are rarely exposed to the
complex, “under-the-hood” aspects of our system
• It’s more likely that they understand the parts of the system they
connect with directly: doctors, hospitals, insurance plans, and the public
and private health programs they use in their local communities
• Only a handful of consumers have direct knowledge of systems in
other countries
• Notably, our polls of consumers in countries like France, Germany,
Switzerland, and others reveal their constituents understand their
systems more and rate their system more favorably than U.S. citizens
rate our health care system
Copyright © 2012 Deloitte Development LLC. All rights reserved.
Percent who feel the health care system
of their country works better than most
systems in the world
24% 42%
Percent who believe that the quality of
care in their country’s health care system 37%
is comparable to the best in the world
44%
UK
Switzerland
Portugal
Mexico
Luxembourg
Germany
France
China
Canada
Brazil
Belgium
US
2
Consumers in countries like France, Germany, and
Switzerland rate their health care system more
favorably than U.S. citizens rate ours.
6%
41% 13% 55% 46% 52%
8%
10% 46% 39%
4%
38% 13% 50% 42% 42%
9%
13% 57% 31%
Percent who feel physicians and
hospitals in their country’s health care
system have access to latest
technologies and treatments
58% 44% 16% 38% 24% 49% 50% 31% 28% 21% 65% 31%
Percent who gave the health care system
a grade of "A" or "B"
22% 57%
Source: 2011 Deloitte Survey of Health Care Consumers Global Report
8%
50% 30% 51% 39% 69% 15% 18% 52% 46%
Copyright © 2012 Deloitte Development LLC. All rights reserved.
A higher percentage of consumers in other countries feel
they have a good understanding of how their health care
system works compared to U.S. consumers.
2
Percent of consumers that report having a good understanding of how their health care system
works, by country, 2011
50%
39%
40%
31%
30%
33%
34%
34%
27%
23%
20%
32%
16%
23%
24%
17%
10%
0%
Source: 2011 Deloitte Survey of Health Care Consumers Global Report
Copyright © 2012 Deloitte Development LLC. All rights reserved.
3
There’s not enough money in the U.S. health system.
Facts:
• There’s plenty of money in the U.S. health system: more than $8,000
per capita
• The U.S. system is built around cures and fixes to complicated
problems; incentives to prevent disease are modest; incentives to “fix”
diseases are attractive; this is counterintuitive, as it costs more to fix a
problem than to prevent it
• Our health care system is not organized: it’s a complicated array of
highly regulated, capital intense, labor intense sectors — each setting
has its own rules which are virtually independent of each other
• Minimal integration and coordination across sectors leads to
administrative waste
Copyright © 2012 Deloitte Development LLC. All rights reserved.
3
There’s plenty of money in the U.S. system: more than $8,000
per capita.
$8,233
United States (2010)
Switzerland (2011)
$5,489
Country (year)
Luxembourg (2009)
$4,786
Canada (2011)
$4,608
Germany (2010)
$4,338
France (2010)
$3,974
United Kingdom (2011)
$3,433
Japan (2009)
$3,035
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
$8,000
$9,000
Per capita health care spending
Source: 2011 Deloitte Survey of Health Care Consumers Global Report
Copyright © 2012 Deloitte Development LLC. All rights reserved.
4
Government health care programs — Medicare and
Medicaid — are poorly managed and need overhaul.
Facts:
• Federal and state administrative costs associated with Medicare and
Medicaid are less than those associated with commercial health
insurance: less than 2% and 5% versus 12%, respectively
• Costs of these programs are soaring due to increased enrollment and
rising costs of health care utilization
• Overhaul of these programs is necessary due to the realities of demand
and medical inflation, not necessarily the ineptitude of administrators
Copyright © 2012 Deloitte Development LLC. All rights reserved.
4
The administrative costs for federal programs are less than the
administrative costs for commercial health insurance.
14%
12%
10%
8%
6%
4%
2%
0%
Medicare
Medicaid
Source: CMS, Office of the Actuary, Table 14: National Health Expenditure by Type of Expenditure and Program, 2010
Commercial insurance
Copyright © 2012 Deloitte Development LLC. All rights reserved.
5
There is a shortage of primary care physicians.
Facts:
• If the presumption is that ONLY MDs/DOs are capable of providing
primary care to patients and incentives continue to be based on
visits, not results, then the statement is accurate
• If new incentives for managing health existed, technologies to
enable self-care were accessible, and all practitioners were
allowed to practice to the full extent of their training, there might not
be a shortage
• The myth presumes a reformed system where sick-care and
well-care are not appropriately balanced and funded
Copyright © 2012 Deloitte Development LLC. All rights reserved.
5
If practitioners including nurses, nutritionists, pharmacists,
and counselors were allowed to practice to the full extent of
their training, there would be no shortage.
Total U.S.
Degree and education
professionals
Clinical training
Total years education
and training
Physicians: Medical
Doctors (MDs) and
Doctors of
Osteopathic
Medicine (DOs)
661,400
Requires 4 years undergraduate (B.A. or Residency training is required to
B.S.) degree with pertinent science
practice clinically, typically 3 to 7
coursework; 4 years medical school
years; may be followed by
fellowship of 1 to 3 years to further
specialize
11-18 years, depending
on residency and
fellowship
Nurse practitioner
(NP)
140,000
Requires registered nurse (RN) training
(through bachelors or associate degree),
and NP master’s degree (2 years) or
doctorate (4 years); national board
certification by area of specialty through
state nursing boards
Advanced clinical training
is part of RN and NP
education programs; no additional
clinical requirements after
certification
4-6 years
Physician Assistant
(PA)
74,800
Accredited PA educational programs
include certificate programs and
masters, bachelor’s, and associate
degrees; all require at least 2 years, and
admissions requirements vary; many
students have B.A.s prior to entering; all
graduates must pass the Physician
Assistant National Certifying
Examination to practice
Some clinical training is
included in PA educational
programs; additional education is
possible after
attaining certification but is not
required
4-6 years
Pharmacist
269,900
2 years of professional study, usually at
a college or university, are required to
pursue a degree, followed by 4 years of
a Pharm.D. program
Pharm.D. studies include some
clinical training; 1 to 2 year
residency and fellowship programs
are available but not required
6-10 years, depending
on undergraduate degree
fulfillment, residency, and
fellowship
Source: Deloitte Center for Health Solutions, “Primary Care: Today and Tomorrow,” 2011
Copyright © 2012 Deloitte Development LLC. All rights reserved.
6
The major driver of health costs is unhealthy lifestyles, and
the Affordable Care Act (ACA) doesn’t address this at all.
Facts:
• Cost associated with chronic diseases and lifestyle choices is only
one factor
• Other cost drivers include: financial rather than clinical incentives to do
more tests and procedures, and the underlying cost of technologies and
regulatory compliance
• The ACA has a number of provisions that address lifestyle and chronic
disease management; beginning in 2014, most health plans will be
required to cover preventive wellness and chronic disease management
services
Copyright © 2012 Deloitte Development LLC. All rights reserved.
6
Many factors contribute to the costs of health care in the
U.S. system.
Major drivers of cost
Key points
Medical technology advances
•
Dominant driver of long-term cost increases
•
Modern diagnosis and treatment technologies may replace less expensive options or create new
opportunities for care
•
May account for as much as half of long-term increases to U.S. health care spending
•
Delayed adoption of best care practices and/or poor physician performance
•
Patient injury and ineffective treatment concerns
•
$102-154 billion waste estimate (2011)
•
Fragmented care leads to increased dependency and readmission rates
•
$25-45 billion waste estimate (2011)
•
Care provided despite no proven health benefit
•
$158-226 billion waste estimate (2011)
•
Inefficient administrative procedures reduce physician and hospital productivity
•
$107-389 billion waste estimate (2011)
•
Lack of transparency leads to greater profits than expected in normal marketplace
•
$84-178 billion waste estimate (2011)
Fraud and abuse
•
$82-272 billion waste estimate (2011)
Chronic disease treatment
•
Increased chronic disease prevalence requires additional health care expenditures
•
Over 75% of U.S. health care spending related to treatment of chronic conditions
•
Obese population may lead to higher health care costs due to correlation between weight and the
development of some chronic diseases
Failures of care delivery
Failures of care coordination
Overtreatment
Administrative complexity
Pricing failures
Sources: Robert Wood Johnson Foundation, “High and rising health care costs: Demystifying U.S. health care spending”, Oct. 2008; Journal of the American Medical Association,
“Eliminating Waste in U.S. Healthcare”, Mar. 2012; Congressional Budget Office, “Technological Change and the Growth of Health Care Spending”, Jan. 2008; Centers for Disease
Control and Prevention, “Chronic diseases: the power to prevent, the call to control”, 2009
Copyright © 2012 Deloitte Development LLC. All rights reserved.
6
ACA provisions target unhealthy behavior.
Section
Provision
Section 4108:
Incentives for prevention
of chronic diseases in
Medicaid
Grants to states to provide incentives for Medicaid beneficiaries to participate in
programs providing incentives for healthy lifestyles. Must have demonstrated
success in helping individuals lower or control cholesterol and/or blood pressure,
lose weight, quit smoking and/or manage or prevent diabetes, and may address
co-morbidities, such as depression, associated with these conditions.
Section 2502:
Elimination of exclusion
of coverage of
certain drugs
Beginning with drugs dispensed on January 1, 2014, smoking cessation drugs,
barbiturates, and benzodiazepines will be removed from Medicaid’s excludable
drug list
Section 4004:
Education and outreach
campaign regarding
preventive benefits
National public/private partnership for the purposes of conducting a national
prevention and health promotion outreach and education campaign
Section 4103:
Provides coverage under Medicare, with no co-payment or deductible, for an
Medicare coverage of
annual wellness visit and a personalized prevention plan. Such services would
annual wellness visit
include a comprehensive health risk assessment.
providing a personalized
prevention plan
Source: The Patient Protection and Affordable Care Act, 2010
Copyright © 2012 Deloitte Development LLC. All rights reserved.
7
The ACA does nothing to lower costs.
Facts:
• The ACA includes a complicated set of demonstrations and pilots that
“might” bend the cost curve:
– Avoidable readmission penalties to hospitals, limitations on physician selfreferrals and private inurement, increased transparency to equip consumers
to understand treatment options and underlying evidence, etc.
• Its major tenet for cost reduction is often missed:
– By increasing access to insurance coverage for 32 million people, changing
incentives from fee-for-service to performance and value, and requiring use
of information technologies to improve diagnostic accuracy and reduce error,
it fundamentally shifts the system to a consumer-directed one in which
individuals bear more responsibility for their own decisions; therein,
significant cost reduction may be achieved
Copyright © 2012 Deloitte Development LLC. All rights reserved.
7
The ACA includes a complicated set of demonstrations
and pilots that “might” bend the cost curve.
Section
Provision
Sec. 2403: Money Follows the
Person Rebalancing
Demonstration
Extends the Money Follows the Person Rebalancing Demonstration through September 30, 2016
and changes the eligibility rules for individuals to participate in the demonstration project by
requiring that individuals reside in an inpatient facility for not less than 90 consecutive days
Sec. 2704: Demonstration
project to evaluate integrated
care around a hospitalization
Establishes a demonstration project, in up to eight states, to study the use of bundled payments for
hospital and physicians services under Medicaid
Sec. 2705: Medicaid global
payment system demonstration
project
Establishes a demonstration project, in coordination with the CMS Innovation Center, in up to five
states that would allow participating states to adjust their current payment structure for safety net
hospitals from a fee-for-service model to a global capitated payment structure
Sec. 2706: Pediatric
Accountable Care Organization
demonstration project
Establishes a demonstration project that allows qualified pediatric providers to be recognized and
receive payments as Accountable Care Organizations (ACO) under Medicaid; the pediatric ACO
would be required to meet certain performance guidelines; pediatric ACOs that meet these
guidelines and provide services at lower costs will share in those savings
Sec. 3024: Independence at
home demonstration program
Creates a new demonstration program for chronically ill Medicare beneficiaries to test a payment
incentive and service delivery system that utilizes physician and nurse practitioner directed homebased primary care teams aimed at reducing expenditures and improving health outcomes
Sec. 3123: Extension of the
Rural Community Hospital
Demonstration Program
Extends the program for five years, expanding eligible sites to additional states and rural hospitals,
and makes adjustments to payment levels provided within the demonstration program
Source: The Patient Protection and Affordable Care Act
Copyright © 2012 Deloitte Development LLC. All rights reserved.
8
Most of the care that’s recommended is necessary, therefore
most of the system spend is appropriate and unavoidable.
Facts:
To be fair, no one knows for sure…
• What we do know: quality of care is dependent on geographic location
• According to the Institute of Medicine (IOM), adherence to evidencebased practices (EBPs) by clinicians is highly variable; applying EBPs
to all treatment and patient management recommendations could
reduce costs by up to 30%
• Most of the care is probably necessary but a substantial amount may
not be, and knowing the difference between the two is essential to
improve health outcomes and lower costs
Copyright © 2012 Deloitte Development LLC. All rights reserved.
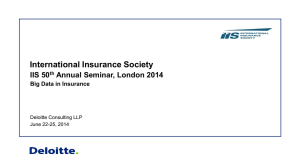
8
8% of total annual health care expenditures are related to
unnecessary care.
$210 billion
Total health care expenditures in
2010 = $2.6 trillion
8% ($210 billion) of health care services represent:
• Overuse: services beyond evidence-established
levels
• Defensive medicine
• Unnecessary choice of higher cost services
Source: Institute of Medicine, The Healthcare Imperative: Lowering Costs and Improving Outcomes, 2010
8%
$2.6 trillion
Copyright © 2012 Deloitte Development LLC. All rights reserved.
9
The health insurance industry is the problem,
and its fate uncertain.
Facts:
• The problem with the health care system is not the fault of one sector;
the entire system is fragmented and expensive
• There are two reasons insurance as an industry will thrive in
coming years:
1. Employers and consumers value the financial security they gain from
insurance coverage: they want to keep coverage
2. Enrollment in managed care will increase: state and federal programs such
as Medicare and Medicaid will increasingly embrace managed care in their
program designs to lower costs and coordinate care
Copyright © 2012 Deloitte Development LLC. All rights reserved.
9
The vast majority of employers do not anticipate dropping
health insurance coverage within the next 3 years.
Number of employers anticipating dropping health insurance coverage
in the next one to three years, by employer size, 2012
13%
79%
50-100 employees
8%
5%
82%
101-999 employees
Company size
13%
1%
95%
1,000-2,499 employees
4%
2%
91%
2500+ employees
7%
9%
81%
Total employers
10%
0%
20%
40%
60%
80%
100%
Agree: My company anticipates dropping health insurance coverage in the next 1-3 years
Disagree: My company does not anticipate dropping health insurance coverage in the next 1-3 years
Don't know
Source: Deloitte Center for Health Solutions, 2012 Survey of U.S. Employers
Copyright © 2012 Deloitte Development LLC. All rights reserved.
9
Medicaid managed care enrollment is increasing steadily.
Medicaid managed care enrollment (percent of total Medicaid beneficiaries): point in time
enrollment as of June 30th and as of July 1st for 2010
100%
80%
60%
70.91%
56.82%
57.58%
59.11%
60.68%
62.95%
65.34%
71.73%
71.45%
64.10%
40%
20%
0%
FY2001
FY2004
Source: Centers for Medicare and Medicaid Services (CMS), Managed Care Trends, 2010
FY2007
FY2010
Copyright © 2012 Deloitte Development LLC. All rights reserved.
10
Health reform is about the future of the ACA.
Health
expenditures
are the
elephant in the
room
25%
17.6%
of the U.S. gross
domestic product
19%
of household
discretionary
spending
Source: “Deloitte Heath Care Reform: Center Stage 2012”
of the federal
budget
23%
of the average
state budget
Copyright © 2012 Deloitte Development LLC. All rights reserved.
10
Health reform is about the future of the ACA.
Facts:
• Regardless of the election outcome, policymakers and the industry
must grapple with the system’s costs; it should take priority
• The big question in health reform is this:
Is our system performing at a level that’s commensurate with
the value it adds in communities, companies, and households,
and if not, how can the value gap be bridged?
• It’s about cost vs. results, perception vs. reality, platitude vs.
pragmatics, theory vs. practice, and wants vs. needs; it’s the national
discussion we have to have regardless of the ACA
Copyright © 2012 Deloitte Development LLC. All rights reserved.
Contacts
Paul H. Keckley, PhD
Executive Director
Deloitte Center for Health Solutions
Deloitte LLP
pkeckley@deloitte.com
Ama Ocran
Health Policy Specialist
Deloitte Center for Health Solutions
Deloitte LLP
aocran@deloitte.com
Sophie Stern
Health Policy Specialist
Deloitte Center for Health Solutions
Deloitte LLP
sostern@deloitte.com
Copyright © 2012 Deloitte Development LLC. All rights reserved.
To learn more about the Deloitte Center for Health Solutions, its projects and events, please
visit: www.deloitte.com/centerforhealthsolutions.
Deloitte Center for Health Solutions
1001 G Street N.W.
Washington, DC 20001-4545
Phone 202 220 2177
Fax 202 220 2178
Toll free 888 233 6169
Email healthsolutions@deloitte.com
Web http://www.deloitte.com/centerforhealthsolutions
This publication contains general information only and Deloitte is not, by means of this publication, rendering accounting, business, financial, investment, legal, tax, or other professional
advice or services. This publication is not a substitute for such professional advice or services, nor should it be used as a basis for any decision or action that may affect your business.
Before making any decision or taking any action that may affect your business, you should consult a qualified professional advisor.
Deloitte shall not be responsible for any loss sustained by any person who relies on this publication.
About Deloitte
Deloitte refers to one or more of Deloitte Touche Tohmatsu Limited, a UK private company limited by guarantee, and its network of member firms, each of which is a legally separate
and independent entity. Please see www.deloitte.com/about for a detailed description of the legal structure of Deloitte Touche Tohmatsu Limited and its member firms. Please see
www.deloitte.com/us/about for a detailed description of the legal structure of Deloitte LLP and its subsidiaries. Certain services may not be available to attest clients under the rules and
regulations of public accounting.
About the Center
The Deloitte Center for Health Solutions (DCHS) is the health services research arm of Deloitte LLP. Our goal is to inform all stakeholders in the health care system about emerging
trends, challenges and opportunities using rigorous research. Through our research, roundtables and other forms of engagement, we seek to be a trusted source for relevant, timely
and reliable insights.
Copyright © 2012 Deloitte Development LLC. All rights reserved.
Member of Deloitte Touche Tohmatsu Limited
Copyright © 2012 Deloitte Development LLC. All rights reserved.
About Deloitte
Deloitte refers to one or more of Deloitte Touche Tohmatsu Limited, a UK private company limited by guarantee, and its network of
member firms, each of which is a legally separate and independent entity. Please see www.deloitte.com/about for a detailed
description of the legal structure of Deloitte Touche Tohmatsu Limited and its member firms. Please see www.deloitte.com/us/about
for a detailed description of the legal structure of Deloitte LLP and its subsidiaries. Certain services may not be available to attest
clients under the rules and regulations of public accounting.
Copyright © 2012 Deloitte Development LLC. All rights reserved.
Member of Deloitte Touche Tohmatsu Limited