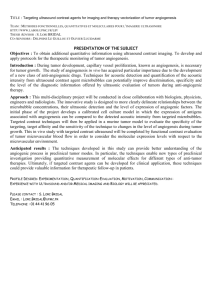
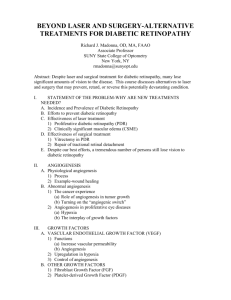
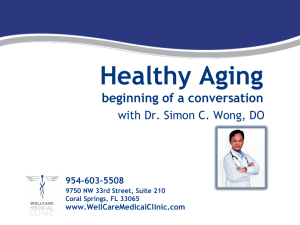
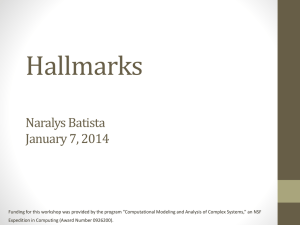
PPT Version - OMICS International
advertisement

OMICS Journals are welcoming Submissions OMICS International welcomes submissions that are original and technically so as to serve both the developing world and developed countries in the best possible way. OMICS Journals are poised in excellence by publishing high quality research. OMICS International follows an Editorial Manager® System peer review process and boasts of a strong and active editorial board. Editors and reviewers are experts in their field and provide anonymous, unbiased and detailed reviews of all submissions. The journal gives the options of multiple language translations for all the articles and all archived articles are available in HTML, XML, PDF and audio formats. Also, all the published articles are archived in repositories and indexing services like DOAJ, CAS, Google Scholar, Scientific Commons, Index Copernicus, EBSCO, HINARI and GALE. For more details please visit our website: http://omicsonline.org/Submitmanuscript.php Anti-Angiogenesis Therapy for Cancer Treatment: An Overview for Clinicians Xiaodong Feng, PhD, PharmD Associate Professor of Clinical Sciences Department of Clinical and Administrative Sciences California Northstate University College of Pharmacy Disclaimer The information within this presentation is for continuing education purposes only, and is not intended to substitute for the medical judgment of the healthcare provider. Recommendations for use of any particular therapeutic agents or methods are based upon the best available scientific evidence and clinical guidelines. Reference in this activity to any specific commercial products, process, service, manufacturer, or company does not constitute its endorsement or recommendation. Faculty Biography International Journal of Cell Biology International Journal of Cell Biology. 2013; vol2013:1-11 International Journal of Cell Biology International Journal of Cell Biology. 2013; vol2013:1-11 Xiaodong Feng, PhD, PharmD Associate Professor of Clinical Sciences Department of Clinical and Administrative Sciences California Northstate University College of Pharmacy Rancho Cordova, CA95670 Developer’s Bio EDUCATION: B. S. Physiology, Nanjing University, Nanjing, China Ph.D. Cellular & Molecular Physiology, Chinese Academy of Medical Sciences, Beijing, China M.S. Computer Science , University of Bridgeport , Bridgeport, CT PharmD, Albany College of Pharmacy, Albany, NY LICENSES: Registered Pharmacist, California State Board of Pharmacy Registered Pharmacist, New York State Board of Pharmacy Topic Related Publication: International Journal of Cell Biology. 2013; vol2013:1-11 US Pharmacist. 2010;35(7) (Oncology Suppl):4-9. Int Angiol. 2006 Dec;25(4):407-13. J Cardiovasc Pharmacol. 2006 Aug;48(2):6-13. J. Invest. Derm. 5; 40-46, 2000. Faculty Disclosures ● Dr. Feng has nothing to disclose. He does not intend to discuss non-FDA approved drugs or investigational use of any products. Objectives • • • • • • 1) Understand the physiology and pathophysiology of angiogenesis 2) Recognize angiogenesis as an essential hallmark feature of solid tumor development 3) Identify the potential drug targets for anti-angiogenesis therapy 4) Discuss and differentiate the mechanisms of action for the FDA approved anti-angiogenesis cancer drugs 5) Evaluate the triumphs and limitations of anti-angiogenesis cancer treatments 6) Assess the treatment strategies and follow up plans of antiangiogenesis cancer treatment Physiology of Angiogenesis • Definition: Angiogenesis is the growth of new blood vessels from pre-existing vessels red blood cell endothelial cell capillary lumen this endothelial cell will generate a new capillary branch pseudopodial process guides the development of the capillary sprout as it grows into the surrounding connective tissue capillary sprout hollows out to form tube (The Cell 4th ed 2002) Physiology of Angiogenesis • Angiogenesis is a dynamic and complicated multistep process involving vascular endothelial: Activation Invasion Migration Proliferation Sprout formation Tube formation Capillary network formation US Pharmacist. 2010;35(7) (Oncology Suppl):4-9. In Vitro Sprouting Angiogenesis of Human Dermal Microvascular Endothelial Cells Presence of Multiple Cells and Lumen International Journal of Cell Biology. 2013; vol2013:1-11 Sprouting Angiogenesis in Wound Healing dermis clot J. Invest. Derm. 5; 40-46, 2000. Angiogenesis: Physiology and Pathophysiology • Angiogenesis is an important process in physiological conditions: Wound healing Reproduction Embryonic development • Angiogenesis also plays an essential role in the pathophysiological conditions: Solid tumor growth Psoriasis Diabetic retinopathy Macular Degeneration US Pharmacist. 2010;35(7) (Oncology Suppl):4-9. Angiogenesis: Physiology and Pathophysiology • Under normal physiologic conditions, angiogenesis is well controlled by the local balance between endogenous angiogenesis stimulators and angiogenesis inhibitors, although the regulatory mechanism is still not clear. • During wound healing, the expression of vascular endothelial growth factor (VEGF), one of the most potent angiogenic stimulators is significantly upregulated to promote wound healing by restoring blood flow to injured tissues. Cancer Res 2005;65:3967-3979 Dynamic regulation of angiogenesis in wound healing: more angiogenesis in fibrin rich wound clot, less in collagen rich scar International Journal of Cell Biology. 2013; vol2013:1-11 Angiogenesis: Physiology and Pathophysiology • Deficient production of angiogenic stimulators turns off angiogenesis switch and leads to insufficient angiogenesis. • Inordinate production of angiogenic stimulators turn on the angiogenesis switch and drives excessive angiogenesis. • Both insufficient and excessive angiogenesis contribute to the pathogenesis of many major diseases • Thus discovering endogenous and exogenous angiogenic inhibitors provides potential drug targets to block angiogenesis for solid tumors. Cancer Res 2005;65:3967-3979. Examples of Angiogenesis Stimulators Vascular endothelial growth factor (VEGF) Fibroblast growth factor (bFGF/aFGF) Placental growth factor (PlGF) Platelet-derived growth factor (PDGF) Transforming growth factor (TGF) Developmental endothelial locus-1 (Del-1) Tumor necrosis factor alfa (TNF-α) Interleukin-8 (IL-8) Hepatocyte growth factor (HGF) Platelet derived endothelial cell growth factor (PD-ECGF) US Pharmacist. 2010;35(7) (Oncology Suppl):4-9. Examples of Angiogenesis Inhibitors Matrix derived Arresten Canstatin Endorepellin Endostatin Fibronectin fragment (Anastellin) ECM-binding integrins Fibulin Thrombospondin-1 and -2 Tumstatin Non-matrix derived Cytokines Interferons Interleukins Pigment epithelium derived factor (PEDF) Fragments of blood coagulation factors Angiostatin Antithrombin III Prothrombin kringle 2 Platelet factor-4 Pharmaceuticals 2010, 3, 3021-3039; Angiogenesis and Solid Tumor Development . J Natl Cancer Inst. 2006;98:316-325. Sustained Angiogenesis is a hallmark feature of solid tumors! Cell. 2011;144:646-674 •Hypoxia occurs in overgrowing tumors •Hypoxia causes accumulation of HIF (hypoxia induced factor) •HIF transports into the nucleus and induces the expression VEGF and other target genes. •VEGF is one of the main angiogenic stimualtors Angiogenesis and Solid Tumor • Progressive solid tumor growth is dependent on angiogenesis • Most tumors in human persist in situ for a long period of time in an avascular and quiescent status • The tumor switches to an angiogenic phenotype by a change in the balance between positive and negative regulators of angiogenesis , to invoke new capillary network formation • New Blood vessels provide nutrients for tumor growth • The expending tumor mass invade blood vessels and neoplastic cells disseminate in the blood stream inducing metastasis. US Pharmacist. 2010;35(7) (Oncology Suppl):4-9 Anti-Angiogenesis Therapy for Cancer • The investigation to inhibit tumor angiogenesis has shed new light on cancer treatment. • The FDA approved almost twenty molecularly targeted anti-angiogeneis therapeutic drugs for cancer treatment, • Anti-angiogenesis therapy represents one of the most significant advances in clinical oncology. • More research needs to fully understand the biological mechanisms of tumor angiogenesis to optimize this new cancer treatment strategy US Pharmacist. 2010;35(7) (Oncology Suppl):4-9. Strategies for Anti-Antiangiogenesis Therapy • Restore the dynamic balance between angiogenic inhibitors and angiogenic stimulators ---Decrease the production or activities of angiogenic stimulators, such as VEGF ---Increase the production and activities of angiogenic inhibitors, such as endostatin • Disrupt the major components of angiogenesis process ---Inhibiting the activation of vascular endothelial cells ---Blocking endothelial adhesion , migration, invasion and tube formation Potential Molecular Targets for Anti-angiogenesis • Many enzymes, growth factors, extracellular matrix (ECM) proteins, ECM receptors and their signal transduction pathways . • Drugs based on blocking monoclonal antibodies and chemical inhibitors are being developed to block the effect of angiogenesis growth factors. • Since VEGF plays an essential role in stimulating tumor angiogenesis, blocking VEGF mediated signaling pathways has been one of the major strategy for anti-angiogenesis therapy. VEGF: The Main Molecular Target for Anti-angiogenesis • Currently, there are six members in the family of VEGFs, i.e. VEGF-A, -B, -C, -D, -E, and placenta growth factor (PlGF). • The VEGF family proteins bind in a distinct pattern to three structurally related receptor tyrosine kinases known as VEGF receptor (VEGFR)-1, -2, and -3. • Blocking antibodies, synthetic or natural proteins against VEGF or VEGFR, and inhibitors of VEGF receptor tyrosine kinase and its downstream signal transduction pathway are some of the major antiangiogenesis therapeutic agents. US Pharmacist. 2010;35(7) (Oncology Suppl):4-9. Anti-angiogenesis Drug Targets: Monoclonal antibody to VEGF Ribozyme targeting VEGF mRNA VEGF antisense oligonucleotide VEGF receptor inhibitor Soluble decoy receptor to trap VEGF VEGFR-2 inhibitor peptide VEGFR/PDGFR dual kinase inhibitor VEGFR1 peptide vaccine VEGFR2 peptide Vaccine Small molecule VEGF RTK inhibitor mTOR inhibitors Bevacizumab (Avastin) Angiozyme GEM 220, Veglin PTK787/ZK222584 VEGF Trap (Afilbercept) CT-322 TAK-593 VEGFR1-1084 peptide vaccine VEGFR2-169 peptide vaccine sunitinib (Sutent) sorafenib (Nexavar) temsirolimus (CCI-779) everolimus (RAD001), FDA Approved Anti-angiogenesis Therapy: bevacizumab (Avastin) Mechanism of Action • Bavacizumab is the first anti-angiogenesis therapy agents approved by the FDA. • It is recombinant humanized monoclonal antibody directed against VEGF-A which is widely expressed in many solid human cancers. • It inhibits formation of new blood vessels in primary tumor and metastatic tumors. FDA Approved Anti-angiogenesis Therapy: bevacizumab (Avastin) Approved Indication • First-line therapy to treat metastatic colorectal cancer in combination with 5-fluorouracil. It is not indicated for adjuvant treatment of colon cancer • Second-line therapy to treat metastatic colorectal in combination with FOLFOX-4. • To treat non-squamous non–small cell lung cancer in combination with carboplatin/paclitaxel. • Approved as a single agent treatment for glioblastoma with progressive disease following prior therapy. • To treat renal cell cancer in combination with interferon-alpha Efficacy of Bevacizumab: Metastatic Colorectal Cancer (mCRC) IFL + Avastin 5 mg/kg q 2 wks * p < 0.001 by stratified log rank test. † p < 0.01 by χ2 test. Number of Patients 411 402 Overall Survival* Median (months) 15.6 20.3 Hazard ratio 0.66 Progression-free Survival* Median (months) 6.2 10.6 Hazard ratio 0.54 Overall Response Rate† Rate (percent) 35% 45% Duration of Response Median (months) 7.1 IFL + Placebo IFL (irinotecan 125 mg/m2, 5-FU 500 mg/m2, and leucovorin (LV) 20 mg/m2 given once weekly for 4 weeks every 6 weeks) http://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=93 9b5d1f-9fb2-4499-80ef-0607aa6b114e FDA Approved Anti-angiogenesis Therapy: bevacizumab (Avastin) Black Box Warning • Gastrointestinal Perforation: Occurs in up to 2.4% of Avastintreated patients. Discontinue Avastin for gastrointestinal perforation. • Surgery and Wound Healing Complications: Discontinue in patients with wound dehiscence. Discontinue at least 28 days prior to elective surgery. Do not initiate Avastin for at least 28 days after surgery and until the surgical wound is fully healed. • Hemorrhage: Severe or fatal hemorrhage, hemoptysis, gastrointestinal bleeding, CNS hemorrhage, and vaginal bleeding are increased in Avastin- treated patients. Do not administer Avastin to patients with serious hemorrhage or recent hemoptysis. Clinical Considerations for Bevacizumab (1) • Do not infuse in a dextrose containing solution. • Increased risk of arterial thromboembolic events, including myocardial infarction and stroke. Risk factors are age >65 years and history of angina, stroke, and prior arterial thromboembolic events. • Potential for serious and, in some cases, fatal hemorrhage resulting from hemoptysis in patients with non squamous non–small cell lung cancer. • Patients with recent hemoptysis (>1/2 tsp of red blood) should not receive bevacizumab. Clinical Considerations for Bevacizumab (2) • Use with caution in patients who have undergone recent surgical and/or invasive procedures. • Bevacizumab should be given at least 28 days after any surgical and/or invasive intervention. • In patients who have undergone surgical resection of the liver, bevacizumab should not be given for at least 6 to 8 weeks after the surgical procedure. • Use with caution in patients with uncontrolled hypertension . Discontinued in patients with hypertensive crisis. Clinical Considerations for Bevacizumab (3) • Discontinue in patients with nephrotic syndrome. Hold for proteinuria >2 grams/24 hours and resumed when <2 grams/24 hours. • Reversible posterior leukoencephalopathy syndrome (RPLS) can occur from 16 hours to 1 year after initiation of bevacizumab • Infusion-related symptoms with fever, chills, urticaria, flushing, fatigue, headache, bronchospasm, dyspnea, angioedema, and hypotension can be treated by benadryl and acetaminophen. • Although bevacizumab is pregnancy category B, don’t recommend it for pregnancy, since angiogenesis is essential for embryonic development. Anti-angiogenesis Therapy: ziv-aflibercept (Zaltrap) Mechanism of Action • Ziv-Aflibercept is a fused protein comprised of segments of the extracellular domains of human VEGF receptors 1 (VEGFR1) and 2 (VEGFR2), and constant region (Fc) of human IgG. • Afilbercept inhibits angiogenesis by functioning as a soluble decoy receptor to trap VEGFs. Indication: • It is indicated in combination with FOLFIRI (5-fluorouracil, leucovorin, irinotecan) for patients with metastatic colorectal cancer (mCRC) that is resistant to or has progressed following an oxaliplatin-containing regimen. • Warning and toxicity: very similar to bevacizumab Efficacy of Zaltrap in mCRC resistant to oxaliplatin-based combination chemotherapy, with or without prior bevacizumab Placebo/FOLFIRI (N=614) Overall Survival Number of deaths, n (%) ZALTRAP/FOLFIRI (N=612) Stratified Hazard ratio (95% CI) 460 (74.9%) 403 (65.8%) 12.06 (11.07 to 13.50 (12.52 to 13.08) 14.95) 0.817 (0.714 to 0.935) Stratified Log-Rank test p-value 0.0032 Median overall survival (95% CI) (months) Progression Free Survival (PFS) Number of events, n (%) Median PFS (95% CI) (months) Stratified Hazard ratio (95% CI) Stratified Log-Rank test p-value Overall Response Rate (CR+PR) (95% CI) (%) Stratified Cochran-Mantel-Haenszel test p-value 454 (73.9%) 4.67 (4.21 to 5.36) 393 (64.2%) 6.90 (6.51 to 7.20) 0.758 (0.661 to 0.869) 0.00007 11.1 (8.5 to 13.8) 19.8 (16.4 to 23.2) 0.0001 http://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=f6725df6-50ee-4b0a-b900-d02ba634395d Anti-angiogenesis Therapy: Angiogenic Signal Inhibition • The discovery of downstream signal-transduction pathways for RTK has also led to the development of many new targeted agents. • The three major signal transduction pathways for angiogenic growth factors RTK include the Ras/Raf/MAPK pathway, PI3K/Akt/ mTOR pathway and PKC pathway. US Pharmacist. 2010;35(7) (Oncology Suppl):4-9. Anti-angiogenesis Drug Targets : RTK Small Molecule Inhibitors • In addition to the ligand blocking agents, anti-angiogenesis drugs are also being developed to block the signal transduction pathway for angiogensis stimulators. • Several small molecular weight receptor tyrosine kinase (RTK) inhibitors, such as sunitinib and sorafenib, have been developed to target the signal transduction pathway of angiogenic stimulators: – – – – – – platelet-derived growth factor receptors (PDGFRα and PDGFRβ), vascular endothelial growth factor receptors (VEGFR1, 2, 3) Stem cell factor receptor (KIT), Fms-like tyrosine kinase-3 (FLT3), Colony stimulating factor receptor Type 1 (CSF-1R), Glial cell-line derived neurotrophic factor receptor RET) Anti-angiogenesis Drug Targets : RTK Small Molecule Inhibitors RTK Inhibitors Main Targets Indications Sunitinib (Sutent) PDGFR , VEGFR1, 2, 3 KIT, FLT3, CSF-1R, RET gastrointestinal stromal tumor after disease progression on or intolerance to imatinib Sorafenib (Nexavar) RAF, KIT, FLT-3, VEGFR-1, 2, 3, RET, and PDGFR Unresectable hepatocellular carcinoma Advanced renal cell carcinoma Vandetanib (Caprelsa) EGFR, VEGFR , RET, BRK, TIE2, EPH receptor and Src treatment of symptomatic or progressive advanced medullary thyroid cancer Cabozantinib (Cometriq) RET, MET, VEGFR-1, 2, 3, KIT, progressive, metastatic medullary thyroid cancer TRKB, FLT-3, AXL, and TIE-2 (MTC) Axitinib (Inlyta) VEGFR)-1, 2, 3 advanced renal cell carcinoma after failure of one prior systemic therapy Regorafenib (Stivarga) RET, VEGFR1, 2, 3, KIT, PDGFR, FGFR, TIE2, DDR2, TrkA, Eph2A, RAF-1, and Abl Metastatic colorectal cancer (CRC) Locally advanced, unresectable or metastatic gastrointestinal stromal tumor (GIST) Pazopanib (Votrient) VEGFR-1, 2, 3, PDGFR, FGFR, advanced renal cell carcinoma Kit, Itk, Lck), and c-Fms advanced soft tissue sarcoma Anti-angiogenesis Drug Targets : RTK Small Molecule Inhibitors RTK Inhibitors Black Box Warning Sunitinib (Sutent) Hepatotoxicity may be severe, and deaths have been reported Sorafenib (Nexavar) N/A Vandetanib (Caprelsa) QT interval prolongation, Torsades de pointes , Do not use in patients with long QT syndrome, correct hypocalcemia, hypokalemia, hypomagnesemia Cabozantinib (Cometriq) Perforations and Fistulas; Severe, sometimes fatal, hemorrhage including hemoptysis and gastrointestinal hemorrhage Axitinib (Inlyta) N/A Regorafenib (Stivarga) Severe and sometimes fatal hepatotoxicity. Monitor hepatic function prior to and during treatment. Pazopanib (Votrient) Severe and fatal hepatotoxicity has been observed in clinical trials. Monitor hepatic function and interrupt, reduce, or discontinue dosing as recommended Anti-angiogenesis Drug Targets : mTOR Inhibitors • Mammalian target of rapamycin (mTOR) is one of the key protein kinases controlling signal transduction from various angiogenic stimulators and upstream proteins to the level of mRNA translation and ribosome biogenesis. • mTOR plays vey critical role in regulating cell cycle progression, cellular proliferation and growth, and angiogenesis. • In 2007, the FDA approved temsirolimus (Torisel), the first drug in the class of mTOR inhibitors, for metastatic renal cell carcinoma (RCC). • In 2009, the FDA approved everolimus (Afinitor), a second drug in the class of mTOR inhibitors, for the treatment of advanced RCC after failure of treatment with sunitinib or sorafenib. Clinical Considerations of mTOR Inhibitors (1) • Use with caution in patients with hepatic impairment, and dose reduction and/or interruption should be considered. • Premedicated with an diphenhydramine to reduce the incidence of hypersensitivity reactions. • Closely monitor triglycerides, cholesterol, serum glucose levels in all patients, especially those with diabetes mellitus. • Closely monitor patients for new or progressive pulmonary symptoms, including cough, dyspnea, and fever, hold Temsirolimus for pulmonary toxicity • It is a strong immunosuppressant, patients are at increased risk for developing opportunistic infections Clinical Considerations of mTOR Inhibitors (2) • It is a strong immunosuppressant, patients are at increased risk for developing opportunistic infections, avoid live vaccine • Adjust dose with CYP3A4 inhibitor, such as ketoconazole, itraconazole, erythromycin, clarithromycin, and grapefruit • Adjust dose with CYP3A4 inducers, such as phenytoin, carbamazepine, rifampin, phenobarbital, and St. John’s Wort • Avoid alcohol or mouthwashes containing peroxide in the setting of • oral ulcerations as they may worsen the condition. • Prengancy category D Other Anti-angiogenesis Drugs: thalidomide (Thalomid) Mechanism of Action • May exert an anti-angiogenic effect through inhibition of basic FGF and VEGF as well as through as yet undefined mechanisms. Indication • To treat newly diagnosed multiple myeloma in combination with dexamethasone • To treat cutaneous manifestations of erythema nodosum leprosum (ENL). Other Anti-angiogenesis Drugs: thalidomide (Thalomid) Black Box Warning • Embryo fetal toxicity, pregnancy category X • It is only available through a restricted distribution program, the THALOMID REMS™ program (formerly known as (S.T.E.P.S.) program) • Significant increased risk of deep vein thrombosis (DVT) and pulmonary embolism (PE) Other Clinical Considerations • Men taking thalidomide must use latex condoms for every sexual encounter with a woman of childbearing potential • HIV mRNA levels may be increased while on thalidomide. • It can cause drowsiness, avoid operating heavy machinery or driving a car while on thalidomide • Risk of serious skin reactions, Stevens-Johnson syndrome Other Anti-angiogenesis Drugs: lenalidomide (Revlimid) Mechanism of Action • May exert an anti-angiogenic effect through inhibition of basic FGF and VEGF as well as through as yet undefined mechanisms. Indication • Myelodysplastic syndrome: 10 mg PO daily. • To treat multiple myeloma in combination with dexamethasone Other Anti-angiogenesis Drugs: lenalidomide (Revlimid) Black Box Warning • Embryo fetal toxicity, pregnancy category X • REVLIMID REMS™ distribution program (formerly known as the “RevAssist® program” • Significant neutropenia and thrombocytopenia • Significant risk of DVT) and PE Other Clinical Considerations • Men on this drug must use latex condoms for every sexual encounter with a woman of childbearing potential, • Should not donate blood or semen while receiving treatment, and for at least 1 month after • Toxic to the bone marrow. Adjust dose for liver dysfunction Prospective Anti-angiogenesis Therapy Target (1): PTK787/ZK222584 • The VEGF receptor inhibitor PTK787/ZK222584 in combination with standard chemotherapy is in phase III clinical trials for colorectal cancer. • It is also in phase II clinical trials for a number of other tumors, such as metastatic gastrointestinal stromal tumors, unresectable malignant mesothelioma. Prospective Anti-angiogenesis Drug Targets (2): Regulating Tumor Microenvironment • The 3D extracellular matrix environment also plays an active role in the regulation of angiogenesis by dynamic interaction between vascular endothelial cells and extracellular matrix. • A study by Cheresh and his colleagues indicated that integrin alpha v beta 3, the receptor for fibrinogen, vitronectin, fibronectin and other matrix proteins, is the marker of sprout angiogenesis. • Blocking antibodies and chemical inhibitors of integrin alphaV beta3 significantly inhibit tumor angiogenesis. Prospective Anti-angiogenesis Drug Targets (3): Regulating Tumor Microenvironment • Many endogenous inhibitors of angiogenesis are fragments of larger extracellular matrix (ECM) molecules. • These fragments become released upon proteolysis of the ECM and the vascular basement membrane by enzymes, such as matrix metalloproteinases (MMPs), cathepsins and elastases. • Dr. Folkman’s laboratory discovered that endostatin, a naturally-occurring 20-kDa C-terminal fragment derived from type XVIII collagen, significantly inhibits tumor growth by blocking tumor angiogenesis. Anti-angiogenesis Drug Targets (4): Regulating Tumor Microenvironment • Regulation of hypoxia induced Factor 1α (HIF-1α) and extracellular marix (ECM) breakdown plays important role in angiogenesis. • Vascular disrupting agents, including tubulin destabilizers that also inhibit HIF-1α expression, may be used to disrupt tumor blood vasculature. Examples of Prospective Anti-angiogenesis Drug Targets Blocking ECM degradation Matrix metalloproteinase (MMP) inhibitors Urokinase/plasmin inhibitors Endogenous Plasminogen and angiogenesis inhibitor collagen XVIII,degradation fragments Vascular targeting Aminopeptidase N, agents tubulin Hypoxia cell Hypoxia agents BMS275291,COL3,Neovastat WX-UK, WK293 Angiostatin, Endostatin, 2ME 2 ZD6126, CA4P,NGR peptides Tirapazamine, Anti-angiogenesis Drug Targets (5): Other targets • Histone deacetylase (HDAC) inhibitors modulate the expression of angiogenesis-related genes, such as hypoxia-inducible factor-1alpha (HIF-1a) and vascular endothelial growth factor (VEGF), NF-κB modulation. • Copper also play important role in the regulation of tumor angiogenesis Anti-angiogenesis Drug Targets: Other targets Epigenetic modification Histone deacetylase (HDAC) DNA methyltransferase (DNMT) inhibitors LBH589, NFkB Proteasome inhibitors PS-341 Copper Copper chelator Ammonium tetrathiomolybdate 5-aza-2'deoxycytidine, zebularine Anti-angiogenesis Drug Targets (3): Other targets • There are at least 30 known endogenous angiogenesis inhibitors found in the body, they are also potential drug targets for anti-angiogenesis therapy. • Angiogenesis inhibitors have also been discovered from natural sources, including: tree bark, fungi, shark muscle and cartilage, sea coral, green tea, and herbs (licorice, ginseng, cumin, garlic). • In total, more than 300 angiogenesis inhibitors have been discovered to date. Anti-angiogenesis Drug Targets (3): Other targets • There are at least 30 known endogenous angiogenesis inhibitors found in the body, they are also potential drug targets for anti-angiogenesis therapy. • Angiogenesis inhibitors have also been discovered from natural sources, including: tree bark, fungi, shark muscle and cartilage, sea coral, green tea, and herbs (licorice, ginseng, cumin, garlic). • In total, more than 300 angiogenesis inhibitors have been discovered to date. SUMMARY • Anti-angiogenesis therapy represents one of the most significant advances in clinical oncology. • More research needs to fully understand the biological mechanisms of tumor angiogenesis to optimize this new cancer treatment strategy. • More drugs are still in development to increase the target specificity and to investigate their roles in the treatment of different cancers. • Although majority of the approved anti-angiogenesis drugs only offers a modest survival benefit in a limited patient population, they paves the way for the development of more optimized anti-angiogeneis strategy for cancer treatment. References • • • • • • • • • • • • • • • • • • • • • • • • • • • • • 1. Nussenbaum F, Herman IM. Tumor angiogenesis: insights and innovations. J Oncol. 2010;2010:132641. 2. Tonnesen MG, Feng X, Clark RA. Angiogenesis in wound healing. J Invest Derm. 2000;5:40-46. 3. Tortora1G, Melisi D and Ciardiello F. Angiogenesis: A Target for Cancer Therapy. Current Pharmaceutical Design, 2004;10: 11-26 4. Isaiah JF and Lee ME. Neoplastic Angiogenesis — Not All Blood Vessels Are Created Equal. N Engl J Med. 2004;351: 215-216. 5. Ma JX, Zhang SX, Wang JJ. Down-regulation of angiogenic inhibitors: a potential pathogenic mechanism for diabetic complications. Curr Diabetes Rev. 2005;1:183-196. 6. Zaman K, Driscoll R, Hahn D, et al. Monitoring multiple angiogenesis-related molecules in the blood of cancer patients shows a correlation between VEGF-A and MMP9levels before treatment and divergent changes after surgical vs. conservative therapy,” International Journal of Cancer. 2006;118,755–764. 7. Pandya NM, Dhalla NS, Santani DD. Angiogenesis—a new target for future therapy. Vascul Pharmacol. 2006;44:265-274. 8. Papetti M, Herman IM. Mechanisms of normal and tumor-derived angiogenesis. Am J Physiol Cell Physiol. 2002;282:C947-C970. 9. Semenza GL. A new weapon for attacking tumor blood vessels. N Engl J Med. 2008;358:2066-2067. 10. Folkman J. Role of angiogenesis in tumor growth and metastasis. Semin Oncol. 2002;29(suppl 16):15-18. 11. Winer E, Gralow J, Diller L, et al. Clinical cancer advances 2008: major research advances in cancer treatment, prevention, and screening—a report from the American Society of Clinical Oncology. J Clin Oncol. 2009;27:812-826. 12. Augustin HG. Translating angiogenesis research into the clinic: the challenges ahead. Br J Radiol. 2003;76:S3-S10. 13. Holden SN, Eckhardt SG, Basser R, et al. Clinical evaluation of ZD6474, an orally active inhibitor of VEGF and EGF receptor signaling, in patients with solid, malignant tumors. Ann Oncol. 2005;16:1391-1397. 14. Ferrara N, Kerbel RS. Angiogenesis as a therapeutic target. Nature. 2005;438:967-975. 15. Aragon-Ching JB, Dahut WL. VEGF inhibitors and prostate cancer therapy. Curr Mol Pharmacol. 2009;2:161-168. 16. Chamberlain MC, Raizer J. Antiangiogenic therapy for high-grade gliomas. CNS Neurol Disord Drug Targets. 2009;8:184-194. 17. Higa G, Abraham J. Biological mechanisms of bevacizumab-associated adverse events. Expert Rev Anticancer Ther. 2009;9:999-1007. 18. Cohen MH, Gootenberg J, Keegan P, Pazdur R. FDA drug approval summary: bevacizumab plus FOLFOX4 as second-line treatment of colorectal cancer. Oncologist. 2007;12:356-361. 19. Krause DS, Van Etten RA. Tyrosine kinases as targets for cancer therapy. N Engl J Med. 2005;353:172-187. 20. Huang D, Ding Y, Li Y, et al. Sunitinib acts primarily on tumor endothelium rather than tumor cells to inhibit the growth of renal cell carcinoma. Cancer Res. 2010;70:1053-1062. 21. FDA. Votrient (pazopanib): highlights of prescribing information. http://www.accessdata.fda. gov/drugsatfda_docs/label/2009/022465lbl.pdf. Accessed May 15, 20010. 22. Montemurro M, Schöffski P, Reichardt P, et al. Nilotinib in the treatment of advanced gastrointestinal stromal tumours resistant to both imatinib and sunitinib. Eur J Cancer. 2009;45:2293-2297. 23. Helmy M. Guirgis. A perspective on tyrosine kinase inhibitors in gastrointestinal stromal tumors and cancer: past and present with emphasis on future and cost. Cancer Therapy. 2007:5: 417-436. 24. Fasolo A, Sessa C. mTOR inhibitors in the treatment of cancer. Expert Opin Investig Drugs. 2008;17:1717-1734. 25. Triano LR, Deshpande H, Gettinger SN. Management of patients with advanced non-small cell lung cancer: current and emerging options. Drugs. 2010;70:167-179. 26. Hudes GR. Targeting mTOR in renal cell carcinoma. Cancer. 2009;115(suppl 10):2313-2320. 27. Board RE, Thatcher N, Lorigan P. Novel therapies for the treatment of small-cell lung cancer: a time for cautious optimism? Drugs.2006;66:1919-1931. 28. Cabebe E, Wakelee H. Role of anti-angiogenesis agents in treating NSCLC: focus on bevacizumab and VEGFR tyrosine kinase inhibitors. Curr Treat Options Oncol. 2007;8:15-27. 29. Xiaodong Feng, William Ofstad and David Hawkins. Antiangiogenesis therapy: a new strategy for cancer treatment. US Pharmacist. 2010;35(7) (Oncology Suppl):4-9. OMICS Group Open Access Membership OMICS publishing Group Open Access Membership enables academic and research institutions, funders and corporations to actively encourage open access in scholarly communication and the dissemination of research published by their authors. For more details and benefits, click on the link below: http://omicsonline.org/membership.php Xiaodong Feng Associate Professor College of Pharmacy California Northstate University USA