CSE practice guidance

CHILD SEXUAL EXPLOITATION
Multi-agency Practice Guidance
October 2014
This practice guidance should be read in conjunction with the Merseyside
Multi-Agency Protocol for Child Sexual Exploitation.
( www.wirral.gov.uk/downloads/7220 )
Supplementary Guidance on Child Sexual Exploitation
Tackling Child Sexual Exploitation Action Plan DfE 2011
‘Puppet On A String The Urgent Need to Cut Children Free From Child Sexual Exploitation’
Sex and Relationship Education Guidance (DfE 0116/2000)
‘Sex and Relationships Educate (SRE) For the 21st Century’
1 CSE Practice Guidance
Contents
1. Introduction, Aims and Objectives
2. Definition and Models of Sexual Exploitation
3.
Dispelling Myths
4.
Signs and Indicators
5.
Push and Pull Factors
6.
Trafficking
7.
Language and Labelling
8.
Sex Offences and Underage Sexual Activity
9.
Multi Agency Child Sexual Exploitation (MACSE)
Meetings
10. Referral Process
11. Children’s Specialist Services
12. Children who are Looked After and the role of Children’s
Specialist Services
13. Cases below the Level 4 Specialist Services Threshold and Early Help
14. Intelligence and Information Gathering
15. Case Studies
16. Resources
Appendices
Appendix 1 Multi Agency Request for Services Form
Appendix 2 CSE Referral Form CSE 1
Appendix 3 CSE Screening Tool
Appendix 4 Flowchart for Referrals
Page 18
Page 19
Page 20
Page 22
Page 24
Page 31
Page 35
Page 41
Page 4
Page 5
Page 6
Page 7
Page 8
Page 10
Page 10
Page 12
Page 14
Page 15
Page 16
Page 17
2 CSE Practice Guidance
“Children who are sexually exploited are the victims of sexual abuse and should be safeguarded from further harm. Sexually exploited children should not be regarded as criminals and the primary law enforcement response must be directed at perpetrators who groom children for sexual exploitation.”
Baroness Morgan of Drefelin
Safeguarding Children and Young People from Sexual Exploitation (2009)
3 CSE Practice Guidance
Introduction
Child Sexual Exploitation (CSE) maintains a very high national profile and remains a key priority area for the Wirral Safeguarding Children Board (WSCB). Partnership work to tackle CSE is led through the CSE strategic group and all organisations have a role to play in ensuring children and young people are protected from CSE. The Jay report into CSE in
Rotherham highlighted that ‘collective failures’ of managers and professionals in partner agencies including Social Care and the Police to acknowledge and respond to the extent of
CSE contributed to 16 years of abuse of children and young people. The report reminds us that we must not be complacent for one minute and we should use the report’s recommendations to test our own responses to vulnerable children, young people and their families, and the effectiveness of our multiagency systems to detect and respond quickly to each and every instance of child sexual exploitation.
The WSCB CSE strategic group was established in 2012 to develop and implement a multiagency action plan to respond to CSE. The Wirral plan is aligned to the pan Merseyside and Cheshire CSE Strategy and the group contributed to the development of the
Merseyside Multi-agency CSE Protocol which was approved by the WSCB in June 2014.
The CSE protocol sets out the multi-agency procedure for tackling CSE in Wirral and across
Merseyside. The protocol details how through the Multi-Agency Child Sexual Exploitation
(MACSE) meetings organisations can work together to reduce the harm posed to children and young people from CSE.
Aims
The practice guidance aims to explain local working arrangements in Wirral around identifying and addressing CSE in line with the Multi Agency CSE Protocol. It will seek to identify the key local roles under the Protocol and help raise awareness of referral processes where CSE concerns exist.
Objectives
The objectives of the practice guidance are to:
1.
Explain local working arrangements and key roles
2.
Set out a clear governance structure and terms of reference
3.
Provide clarity as to the relationship between Sub Group, MACSE meeting and other specialist services groups
4.
Establish a clear referral pathway with key contacts.
In order to:
Minimise confusion around local practice
Promote informed decision making around appropriate use of resources,
Identify clear ‘ownership’ at the appropriate level and
Deliver a corporate memory around the local management of CSE
4 CSE Practice Guidance
Definition and Models of Sexual Exploitation
“For children over 10, sexual exploitation is the most pressing and hidden child protection issue in this country.”
(Anne Marie Carrie, Barnardos)
What is child sexual exploitation?
The sexual exploitation of children and young people under 18 involves exploitative situations, contexts and relationships where young people (or a third person or persons) receive ‘something’ (e.g. food, accommodation, drugs, alcohol, cigarettes, affection, gifts, money) as a result of performing, and/or others performing on them, sexual activities.
Child sexual exploitation can occur through use of technology without the child’s immediate recognition, for example the persuasion to post sexual images on the internet/mobile phones with no immediate payment or gain. In all cases those exploiting the child/young person have power over them by virtue of their age, gender, intellect, physical strength and/or economic or other resources.
(The National Working Group for Sexually Exploited Children and Young People, 2008)
Categories of child sexual exploitation
The Barnardo’s ‘Puppet on a String’ report defined three broad categories of child sexual
exploitation. These were described as:
Inappropriate relationships;
‘Boyfriend’ model of exploitation and peer exploitation; and
Organised/networked sexual exploitation or trafficking.
Young People exploited via gangs
There is some crossover between the first two categories.
They both involve an imbalance of power, which perpetuates the abuse and undermines the will of the victim to the extent that they feel unable to remove themselves from the position they are in.
“He may have other girlfriends but I am special…”
(Victims comment in Jay Report)
There is evidence that children across all cultures, and including a significant proportion of children in the care of local authorities, can be at risk of sexual exploitation. Vulnerability and low self-esteem are the most common factors amongst children who are at risk of being sexually exploited. In some cases, peers who are already involved may draw children into sexual exploitation.
5 CSE Practice Guidance
An older young person or adult who poses as, and who they view as, their partner, frequently coerces young people into sexual exploitation. The young person becomes physically and emotionally dependant on “the partner”, and this may be reinforced by the use of alcohol and drugs. Over time, the young person’s access to their friends and family becomes curtailed and they become alienated from agencies that may be able to identify and interrupt the abuse.
Safeguarding children and young people from sexual exploitation requires two interlinked strategies: one aimed at supporting the child or young person; the other aimed at disrupting and prosecuting alleged abusers.
Dispelling Myths
The Jay report referenced CPS guidance on CSE which had been revised in October 2013 by the Director of Public Prosecutions at that time, Keir Starmer. The revision was in response to widely held views, evidenced in children’s case files which had undermined the credibility of young victims.
This is the list of myths and practitioners should be mindful that they are challenged wherever expressed.
The victim used alcohol or drugs and was therefore sexually available
The victim didn't scream, fight or protest so they must have been consenting
The victim invited sex by the way they dressed or acted
The victim didn't complain immediately, so it can't have been a sexual assault
The victim is in a relationship with the alleged offender and is therefore a willing partner
A victim should remember events consistently
Child may come from a troubled background or have been involved in criminal behaviour in the past and therefore will not be a reliable witness
Children can consent to their own sexual exploitation
CSE is only a problem in certain ethnic/cultural communities
Only girls and young women are victims of child sexual abuse
Children from Black and Minority Ethnic (BME) backgrounds are not abused
There will be physical evidence of abuse.
All of the above elements were referred to at some point in historic files seen as part of the Jay investigation into CSE in Rotherham between 1997 and 2011.
6 CSE Practice Guidance
Signs and Indicators
The following list of indicators is not exhaustive or definitive but it does highlight common signs which can assist professionals in identifying children who may be victims of sexual exploitation. Signs include:
underage sexual activity
inappropriate sexual or sexualised behaviour
sexually risky behaviour, 'swapping' sex partners
repeat sexually transmitted infections in girls, repeat pregnancy, abortions, miscarriage
receiving unexplained gifts or gifts from unknown sources
having multiple mobile phones and worrying about losing contact via mobile
having unaffordable new things (clothes, mobile) or expensive habits (alcohol, drugs)
changes in the way they dress
going to hotels or other unusual locations to meet friends
seen at known places of concern
moving around the country, appearing in new towns or cities, not knowing where they are
getting in/out of different cars driven by unknown adults
having older boyfriends or girlfriends
contact with known perpetrators
involved in abusive relationships, intimidated and fearful of certain people or situations
hanging out with groups of older people, or anti-social groups, or with other vulnerable
peers
associating with other children involved in sexual exploitation
recruiting other children to exploitative situations
truancy, exclusion, disengagement with school, opting out of education altogether
unexplained changes in behaviour or personality (chaotic, aggressive, sexual)mood swings,
volatile behaviour, emotional distress
self-harming, suicidal thoughts, suicide attempts, overdosing, eating disorders
7 CSE Practice Guidance
drug or alcohol misuse
Police involvement, Police records
involved in gangs, gang fights, gang membership
injuries from physical assault, physical restraint, sexual assault.
*These signs have been drawn from a range of research (Barnardo’s, 2011; CEOP, 2011;
Berelowitz et al, (2012) and from the NSPCC
Push and Pull Factors
There are a number of factors that may make a child more vulnerable to sexual exploitation and abuse due to their individual family or personal circumstances- these are called push and pull factors that may either push or pull a child into situations where they are vulnerable to or at risk of being sexually exploited. Abusive adults will look out for signs of these push factors in selecting a child to target.
Push
These include:
Children who have been the victim of physical abuse, sexual abuse, neglect and emotional abuse
Children from households where domestic violence and abuse has been a feature
Children of parents with a high level of vulnerabilities (e.g. drug and/or alcohol abuse,
mental illness, learning disability, their own history of an abusive childhood) There have
been cases where there is evidence of the family also being groomed
Family breakdown / disrupted family life / problematic parenting
Insecure immigration status
Children who have physical or learning impairments
Children with emotional difficulties; low self-esteem; estranged family relationships
Abusers will spend time getting to know their victims and look for indicators of vulnerability even via social networking sites, through chat lines etc. There are also indicators that a child is at risk of or particularly vulnerable to sexual exploitation and abuse:
Going missing – the most immediate indicator of vulnerability to sexual exploitation
Disengagement from education
Drug and/or alcohol dependency
8 CSE Practice Guidance
Physical symptoms e.g. sexually transmitted infections, miscarriage, abortion, bruising or marks indicating physical or sexual assault
Children who have not received appropriate levels of attention from concerned adults
Associating with older men or other ‘risky’ adults
Accounts of social activities with no plausible explanation of the source of the money to fund these activities
New possessions, acquisition of money, expensive clothes, drugs or other possessions
without plausible explanation about their source
Being alienated from family or community
Being in care and having placement breakdown
Associating with other children who are known to be victims of exploitation
Some kinds of offending behaviour
Pull
The grooming techniques used to gain the child’s attention, admiration and affection often taps into insecurities or a desire for acceptance and status by the child. These can be referred to as ‘PULL’ factors and include:
Being liked by someone older;
Being liked/fancied enough that a stranger asks for their mobile number;
Meeting someone who thinks they are special on the internet;
Receiving alcohol, drugs, money or gifts;
Getting a buzz and the excitement of risk taking/forbidden behaviour;
Being offered somewhere to stay where there are no rules/boundaries;
Being taken along to adult entertainment venues, red light or gay cruising areas (public sex environments);
Being given lifts, taken to new places, and having adventures with casual acquaintances.
9 CSE Practice Guidance
Trafficking
Children who are abused through child sexual exploitation may also be trafficked. There are three different types of trafficking of children for the purposes of sexual exploitation.
Firstly, there is trafficking from abroad into the United Kingdom.
The second category is internal trafficking, where children are moved from one place to another in the UK for the purposes of sexual exploitation. This may be from one street to a neighbouring street, from one area of a town or city to another area, or across county borders. It is not the distance that is relevant in the definition of internal trafficking, but the movement of a child for the purpose of sexual exploitation.
The third is being trafficked out of the UK to other countries and brought back again. It is probably helpful for professionals to think of trafficking as moving children around for the purpose of them being abused. An example would be a child from Oxford being taken to
London by their abusers or associates of the abusers and then being abused by other adults in London. Children being moved from street to street by their abusers is another form of trafficking within the UK. Trafficking children, including for the purpose of sexual exploitation is a criminal offence and concerns that a child may be being trafficked should always be reported to the Police and a referral made into CADT.
Professionals will need to collect as much data as possible which includes anything you hear the child say, or hear other children say about them, dates and times when you know or suspect they have been trafficked and any information about the people they were with and vehicles used to transport them. This should be recorded carefully and passed to the
Police for investigation.
Case Study
Trudy is 13 years old. She met a group of older men through her boyfriend who is also
15 years old. Her boyfriend started taking her to a house in her home town where she was forced to have sex with two older men. About a month later one of the men took her to Birmingham where she was taken to a hotel and forced to have sex with another man. Trudy was trafficked for the purpose of sexual exploitation which is a criminal offence.
Language and Labelling
Throughout this document the term ‘child’ will be used to describe any child aged 0 – 18 years. Whilst it is acknowledged that teenagers would wish to be referred to as ‘young people’ the term ‘child’ in this context helps professionals stay focused on the fact that they are children being abused and not young adults making positive choices.
The way we use language influences our thinking. Recent Serious Case Reviews in other areas have highlighted this as a significant issue which contributed to systemic failure to protect.
There are some labels which in the past have been used to describe children and their behaviour and which lead to inaccurate assumptions which in turn can help to minimise the risks and reality of their situation. Professional should avoid using such terms in their
10 CSE Practice Guidance
recording and conversations and should be mindful of when they enter their thinking and challenge them. These include:
Child prostitution: because this term implies that the child is choosing to sell themselves for sex when we know that is not the reality of their situation.
Street wise: because this term implies that the child is able to understand the dangers they face and protect themselves whilst missing from home or care when we know the reality of their situation is that they are vulnerable and exposed to situations they cannot control
Choosing to….: because in situations of child sexual exploitation the child is not making free choices and we know that they are subject to coercion, bribery, violence and threats in order to enforce compliance. Children cannot ‘choose’ to be abused.
Consensual sex: because it is unlawful for a child under 16 to have sex and they cannot legally consent and also because consent implies an understanding of the situation, the risks and an aspect of free choice when we know in CSE the child is not in a position to make such choices
Boyfriend: because in a CSE situation the child is not in a relationship of equals in which they can make free and developmentally appropriate choices about the extent of their sexual activity
Read the following two recordings about a child and reflect on the immediate perception you have of their situation:
Sally is 14 years old and has been living at Care View for 3 months. She is a streetwise young woman who from day one has been a persistent absconder. She chooses to associate with older friends in the town centre where she drinks alcohol and uses drugs.
She refuses to engage with staff and take guidance believing, as always, that she knows best. Sally is known to be sexually active and is promiscuous. She says she has had sex with 7 different partners in the past month. She has already been treated for Chlamydia but she doesn’t seem to care about the impact on her health. We think she is prostituting herself to get money for drugs and new clothes and she is certainly materialistic. Sally is a negative influence on the other young people and often involves younger residents in her inappropriate activities.
Sally is 14 years old and has been living at Care View for 3 months. From day one we have been concerned about her going missing and she is thought to be a very vulnerable child.
Sally is known to be spending time with older men in the town centre and is drinking alcohol and using drugs. This increases her vulnerability. Staff, are working hard to engage
Sally but at the moment she cannot accept our help and support. Sally is sexually active and we believe she is having sex with a number of older men. Sally has been treated for
Chlamydia and we are concerned about her sexual health and well-being. Sally often has money and new clothes which she cannot explain and we feel that she is at risk of, or already being abused through child sexual exploitation. Sally often takes younger residents off with her and we are worried that she is being coerced into introducing other children to the abusers.
Sex Offences and Underage Sexual Activity
11 CSE Practice Guidance
Definitions
For the purpose of this guidance the key age groups identified are:
Children under 13
Children aged 13-15 years old
Children over the age of consent (16) and up to the age of 18
Young people over the age of consent and up to 18 years may still suffer sexual harm through exploitation by predatory adults or through a sexual partner who is abusing a
Position of Trust. Any young person between the age of 16 and 18 who is engaging in sexual activity with a person in a position of trust (i.e. teacher, foster carer or similar) is being sexually exploited and such cases must be referred to the Local Authority Designated
Officer and CADT.
Sexual Offences
Under 13's
A child under 13 is not legally capable of consenting to sexual activity. Any offence under the Sexual Offences Act 2003 involving a child under 13 is very serious and should be taken to indicate that the child is suffering, or is likely to suffer, significant harm. Cases involving children aged under 13 should always be discussed with a nominated child protection lead in the organisation. Under the Sexual Offences Act, penetrative sex with a child under 13 is classed as rape. Where the allegation concerns penetrative sex, or other intimate sexual activity occurs, there would always be reasonable cause to suspect that a child, whether a girl or boy, is suffering or is likely to suffer significant harm. The case should be referred to CADT. A strategy discussion should be held that will involve
Children's Social Care, Police and relevant agencies, to discuss appropriate next steps with the professional. All cases involving under 13s should be fully documented including detailed reasons where a decision is taken not to share information. These decisions are exceptional and only made with the documented approval of a senior manager.
13-15 year olds
Sexual activity with a child under 16 is also an offence. Where it is consensual it may be less serious than if the child were under 13 years, but may nevertheless, have serious consequences for the welfare of the child. Consideration should be given in every case of sexual activity involving a child aged 13-15 as to whether there should be a discussion with other agencies and whether a referral should be made to Children's Social Care. This should always be the case where there is a considerable age difference (i.e. 13 + 17; 15 +
21).
When considering if an offence has occurred. The professional should base this decision using the criteria below. Within this age range, the younger the child, the stronger the presumption must be that sexual activity will be a matter of concern. However, concerns of a similar extent are warranted for older children who are known to have had sexual activity with significantly older adults (i.e. 17 + 33). Cases of concern should be discussed with the nominated child protection lead and/or the professionals’ line manager and subsequently
12 CSE Practice Guidance
with other agencies if required. Where there is reasonable cause to suspect that significant harm to a child has occurred or might occur, the case should be referred to CADT and a
Strategy Discussion should be held to discuss appropriate next steps. Again, all cases should be carefully documented including where a decision is taken not to share information.
Criteria
The considerations in the following checklist should be taken into account when assessing the extent to which a child (or other children) is suffering or is likely to suffer, significant harm and therefore whether a referral to CADT should be made. The age of the child:
Sexual activity at a young age is a very strong indicator that there are risks to the welfare of the child (whether boy or girl) and, possibly, others;
Behaviour of the child i.e. withdrawn/anxious;
The level of maturity and understanding of the child i.e. whether the child is competent to understand and consent to the sexual activity they are involved in;
What is known about the child's living circumstances or background;
Familial child sex offences
Age imbalance, in particular where there is a significant age difference;
Overt aggression or power imbalance, in cases where there is abuse of a Position of
Trust a referral will always be made;
Coercion or bribery including the use of sex for favours i.e. exchanging sex for clothes,
CDs, trainers, alcohol, cigarettes etc. - This could also manifest itself in a child having large amounts of money, jewellery or other valuables that cannot be accounted for.
The misuse or giving of substances as a disinhibitor;
Whether the child's own behaviour, because of the misuse of substances places him/her at risk of harm resulting in an inability to make an informed choice about any activity;
Whether any attempts to secure secrecy have been made by the sexual partner beyond what would be considered usual in a teenage relationship;
Whether the child denies, minimises or accepts concerns;
Whether the methods used are consistent with grooming and/or an accompanying adult gives professional cause for concern;
Whether the sexual partner/s is known by one of the agencies
13 CSE Practice Guidance
Disabled children
Disabled children are more likely to be abused than non-disabled children and they are especially at risk when they are living away from home (NSPCC 2002). They may be particularly vulnerable to coercion due to physical dependency and intimate care needs; or because a learning disability or a communication difficulty means that it is not easy for them to communicate their wishes to another person. This increases the risk that a sexual relationship may not be consensual.
Multi Agency Child Sexual Exploitation (MACSE)
Meetings
The Merseyside multi agency CSE protocol should always be followed in conjunction with the current safeguarding procedures (See Section 4) and is meant to adopt a wider focus on not just the victim(s) but also the perpetrator, enablers and locations in order to reduce the opportunity for further sexual exploitation of children.
The aims and purpose of the protocol are to:
To identify those at risk of being sexually exploited
To apply pro-active problem solving to address the risks associated with victims, perpetrators and locations and ensure the safeguarding and welfare of children and young people who are or may be at risk from sexual exploitation
To take action against those intent on abusing and exploiting children and young people in this way
To provide timely and effective interventions with children and families to safeguard those vulnerable to sexual exploitation
The objectives of the MACSE are to:
Identify those who are at risk of being sexually exploited by sharing information and assessing risk
To carry out risk assessment according to a common framework
To address the risks associated with victims, perpetrators and locations by proactive problem solving
To work collaboratively to ensure the safeguarding and welfare of children and young people who are being or are at risk of being sexually exploited
To take effective action against those intent on abusing and exploiting children and young people in this way
To provide early intervention to reduce the harm posed to children and young people
To investigate, prosecute and disrupt perpetrators
14 CSE Practice Guidance
Promote positive physical and emotional health and well-being of individuals identified as being at risk of child sexual exploitation
To develop a shared picture of child sexual exploitation intelligence
Cases involving children who are at imminent risk, should not wait for the monthly MASCE meeting and professionals must refer the child or young person into the Central Advice and Duty Team (CADT) immediately to ensure safeguarding procedures are commenced and a strategy meeting convened. The referral must include a completed CS1 referral form and completed screening tool.
Where a case has followed this route, and a strategy meeting has been held, the pertinent details must be reported to the next MACSE meeting by the Specialist Services representative. This is essential to ensure that a full intelligence picture is provided to the
MACSE meeting.
In order for the Wirral Safeguarding Children Board (WSCB) to develop a useful intelligence picture, all identified victims, perpetrators, and relevant associates of both must be collated by the MACSE meeting and reported into the WSCB CSE Strategic Group.
The information will also be shared with the regional Merseyside group to identify patterns
1.
2.
3.
4.
and hotspots locally.
Agenda for MACSE
5.
6.
7.
Introductions and apologies
Matters arising
Review of current cases (Review Action Plans)
New referrals (Risk Assess and Set Action Plans)
Intelligence (Including Regional Trends)
Priority Locations
AOB
Referral Process
The entry point for any referral where CSE is a concern is through the Central
Advice and Duty Team (CADT).
Referrals should be made on Multi Agency Request for Services Form (Appendix 1) into
CADT from a secure email accompanied by a CSE 1 Form (Appendix 2). Professionals may find it useful to also use the CSE screening tool (Appendix 3) prior to referral. The tool helps referrers focus on the specific indicators of CSE and provides evidence about the level of risk. Completed screening tools should accompany the MACSE referral.
Referral forms should be emailed to CADT at: cadtsocialcare@wirral.gcsx.gov.uk
Upon receipt at CADT, The MASH Manager will complete a CSE 2 form to assess the level of risk to the child. Both the CSE1 and CSE2 form will be forwarded to the police for discussion at the next MACSE meeting. The police MACSE administrator will send invitations to professionals to attend the appropriate MACSE meeting 7 days before the meeting.
15 CSE Practice Guidance
The MACSE will share information, as per the Information Sharing agreement contained within the Protocol, and review and amend the CSE2 in line with the risks identified. The group will then formulate an Action Plan to reduce the risk to that child or young person.
Cases will be removed from MACSE where agencies agree that the level of risk to the Child or Young Person has sufficiently reduced. If child already has TAF/CIN/CP/LAC plan the actions agreed at the MACSE meeting will be incorporated into that plan.
Detailed information about the operation of the MACSE meeting is contained in the
Merseyside Multi-Agency Protocol for Child Sexual Exploitation which can be accessed and downloaded here: www.wirral.gov.uk/downloads/7220
The referral process is illustrated in Appendix 4.
Children’s Specialist Services
Referral
When a parent, professional, or another person contacts CADT with concerns that a child is being sexually exploited, children’s specialist services should decide on its course of action within 24 hours. This will normally follow discussion with any referring professional or service, and involve other professionals and services as necessary, including the police as a criminal offence may have been committed against a child.
Strategy Discussion
Whenever there is reasonable cause to suspect that a child is suffering, or is likely to suffer, significant harm there should be a strategy discussion involving specialist services, the police, health and other bodies such as the referring agency. This might take the form of a multi-agency meeting or phone calls and more than one discussion may be necessary.
A strategy discussion can take place following a referral or at any other time, including during the assessment process.
Planned emergency action will normally take place following a strategy discussion which will include speaking with the child and ensuring they are kept safe.
Management of cases
All cases referred for CSE will be discussed at the MACSE meeting. Cases which are accepted by specialist services will be allocated a social worker and an assessment will take place under Section 17 or Section 47 of the Children Act. The timescale for the assessment should reflect the level of risk for that particular child. For cases assessed under Section 47 (child protection), if the assessment concludes that the child is at continuing risk of harm then a child protection conference should be convened. If the child is judged to be at immediate risk of harm following the strategy meeting then action should be taken to safeguard the child and if appropriate, legal advice should be sought.
Open Cases
Cases already open to specialist services where CSE is subsequently identified as a factor should also be referred into the MACSE meetings. These cases do not need to be referred into CADT and can be referred directly to the MASCE meetings. The child’s social worker should complete the CSE 1 form and the CSE 2 form with their manager and email it to:
A.BCU.MFH@merseyside.pnn.police.uk
16 CSE Practice Guidance
Where applicable the social worker must inform the child’s IRO that a referral into MACSE has been made. Actions agreed at the MACSE meetings will be incorporated into the relevant plan for the child, i.e. Child in Need plan, LAC Care Plan or Child Protection plan.
When the CSE2 has been completed, the social work team will make a decision as to whether relevant planning meetings need to be brought forward e.g. Child Protection
Review Conference/Core Group/Child in Need Meeting/LAC Care planning meeting. The team should not wait for the MACSE meeting before taking action to safeguard a child.
Children who are Looked After and the role of
Children’s Specialist Services
When a CSE referral is received by CADT and passed to the Looked After Child’s social worker , the allocated social worker must inform their team manager. If this is a child of another local authority then the appropriate local authority must be immediately informed by telephone and in writing.
A Care Planning Meeting chaired by the child’s Independent Reviewing Office (IRO) should be convened and should be attended by the police and relevant professionals: The meeting should consider:
The CSE risks to the child and other children in the placement and what action
should be taken to reduce the risk.
Whether the child should remain in their present placement; and
The feasibility of controlling the child’s movements, and the likely effects of doing so.
What support should be identified to support the child/young person and the carers.
The meeting should also consider the appropriateness and method of informing the child’s parents. If children are accommodated, parent/s must be informed of all significant matters. When a child is subject to a care order, generally their parent/s should be informed of such a significant matter. A decision not to inform the parent/s and the reason should be recorded on file.
If the child is not known to the MACSE meeting the social worker should complete a CSE 1 form and a CSE2 form in conjunction with their manager and send it to:
A.BCU.MFH@merseyside.pnn.police.uk
The social worker will be invited to provide information for the next MACSE meeting which will inform the on-going plan to protect the child from CSE. This may include work undertaken to address issues of going missing, low self-esteem, healthy relationships and sexual relationships.
17 CSE Practice Guidance
Additional Points for children in Foster Care/Residential Care
If the child is in foster care, the social worker and supervising social worker, in conjunction with the fostering team manager, should meet with the foster carer to decide which steps the foster carer could reasonably take to protect the child from going missing and being sexually exploited and this should feed into the care planning meeting.
If the child is in residential care, the residential child care professional and their manager should attend the care planning meeting and agree what actions can be taken to protect the child from going missing.
It may be extremely challenging for carers and staff to prevent a child from being sexually exploited and carers and staff will require on-going support, advice and training in knowing how to respond. These needs must be considered and resources identified, either by the manager of the residential unit or the fostering link worker.
Foster carers and residential staff should ensure that they record all relevant information about anyone a child is associating with, including their appearance, car details, telephone activity, patterns of missing episodes and details of any other children who may go missing with the child at the same time. When a CSE concern is identified regarding any other child referrals must be made in line with the protocol.
Cases below the Level 4 Specialist Services
Threshold
For cases which do not meet the Level 4 Specialist Services threshold (i.e. no identified safeguarding concerns) the case will be passed to the Targeted Services Gateway to undertake an assessment which will identify the relevant support services.
The CSE1 and CSE2 on these cases will still be passed for discussion at the MACSE meetings to ensure that the appropriate support is provided to the child. This may include for example, that a Catch-22 worker as the lead professional, or a Response worker may be included in the Team around the Family (TAF).
In cases where the risk increases, cases will be stepped up into Specialist Services and following review by the MASH manager, appropriate actions will be taken.
Early Help
Early help provide a range of services including youth and community work, family support, young carer’s support, face to face youth counseling, parenting support to parents of adolescents and other universal or targeted services. The role of early help staff in relation to CSE is primarily the prevention, recognition and referral stages. They have a key role to play in educating children to stay safe and prevent the risk of CSE through awareness-raising and keep safe work. Staff should be familiar with and able to use the screening tool and should know when and how to make a referral should they be concerned about a child.
18 CSE Practice Guidance
Staff working in early help services are in a strong position to identify issues within the community including patterns of street activity, street grooming and risk taking behaviours.
They may also become aware of individuals or premises where children are becoming involved. Staff should carefully record such information and pass it on to the police and make referrals to CADT in relation to relevant children.
Intelligence and Information Gathering
In general terms any information that relates to an identifiable individual where CSE or vulnerability to CSE is a concern then a formal referral should be made into CADT and the
Wirral MACSE.
However, professionals and members of the wider community may came across or hold other information relevant to CSE which would be very useful for professionals at the
MACSE meeting to know about and to add to the body of intelligence held by the police.
Examples could be information about a particular off-licence or shop which is selling alcohol to young people, or an address or hotel where teenagers are often or repeatedly dropped off late at night.
If information can identify an individual child or young person then it should be included on the CSE 1 form and referred into CADT. In cases where an individual young person cannot be identified the information can be emailed into the following address with the subject line CSE Intelligence: A.BCU.MFH@merseyside.pnn.police.uk
Professionals submitting information may be contacted and asked to complete a CSE 1 referral.
If any person believes a child or young person is being harmed or is at immediate risk of harm they should always dial 999.
19 CSE Practice Guidance
CASE STUDIES
Child Sexual Exploitation takes many forms: ‘If you can’t rule it out, rule it in’
(Barnardo’s)
This section sets out a number of mini case studies highlighting the different forms of child sexual exploitation. They are all based on real cases where information is in the public domain and are from different areas of the country. They are here as an aid to professionals who may be thinking about whether their concerns about a child are child sexual exploitation. It is important to think about the early grooming stages which are often the point at which parents and professionals instinctively start to feel that something is wrong.
Case Study 1
Two men ages 22 and 23 years manage to meet two 13 year old girls on
Facebook. One of the girls gives the men her mobile phone number. They chat on FB over a few weeks and the men send the girls texts which are sexually suggestive.
The girls agree to meet the men in the local KFC. Both girls are wearing their school uniforms and the men comment how young they look. Over a six month period the men bombard the girls with FB messages and texts and meet them several times.
When the men push the girls to have sex one of them panics and tells her mother. Both men were convicted of grooming for sexual exploitation and enticing a child into sexual activity and were jailed.
Case Study 2
Alex was a 16 year old boy who was struggling in many aspects of his life and had become involved in low level criminal activity. He was involved with the
Youth Offending Service. He was missing school and did not have many friends.
Alex was a vulnerable boy with some social presentation issues including being very overweight and had severe acne which made him anxious about his appearance.
He met a woman who was a lot older than him and she engaged him in drinking and drug taking. The relationship became sexual. His parents and professionals were concerned but because he was 16 years old made a decision that the relationship was consensual.
The woman had significant influence over Alex and the adults around Alex felt that Alex was being manipulated by the adult for her own ends. Eventually she led Alex into drug dealing and he was arrested and charged.
20 CSE Practice Guidance
Case Study 3
Two brothers in their mid-20’s met young girls age 13 and 14 years old via
Facebook, on the street and through the girls’ friends. They were given alcohol and later drugs.
The girls were given Blackberry phones and the men used Blackberry Messenger to contact them (Blackberry Messenger communications are not traceable). The men had more than 20 girls contact details on their phones.
Gradually they enticed the girls into having sex with them and this progressed to them selling the girls for sex to other men.
Case Study 4
Two brothers aged 28 and 32 years old meet a 13 year old girl, Jodie in the local shopping centre in and tell her that the things she is looking at are lovely and she would look pretty in them. The next Saturday she and her friend are shopping again and the same two men approach them and offer to buy them a drink in the café. The girls go.
The next week, just the younger man comes and he spends all afternoon with her. He takes her outside for a walk and kisses her. He starts touching her and then persuades her to have sex. The man rings and texts her all the time and she knows he loves her. He tries to get her to bring her friend to meet his brother.
One day her mum finds stained underwear and rings the Police. She won’t give a statement to the Police but they have her knickers which have semen stains and her mum and dad agree the man should be prosecuted even though Jodie doesn’t want that and says she agreed to sex. He was convicted of sexual activity with a child and sent to prison.
21 CSE Practice Guidance
Resources
CEOP: Child exploitation and online protection centre. Provides many useful resources including training programmes for professionals. There is a short video on what to look out for in relation to grooming. There are great resources for working with children too. To access training materials you have to register to use the site. It’s a simple process which takes 5 minutes and is free. www.ceop.police.uk/
Stop It Now: Resources and training materials. Also develop bespoke training packages including child sexual exploitation. Much of the material on the site is about sexual abuse rather than CSE. There are a couple of very useful downloadable leaflets including ‘The
Internet and Children-What’s The Problem’. This would be really useful for schools and children’s workers and also parents. It covers the use of internet and technology for grooming. Access via the Lucy Faithfull link under the next paragraph.
The Lucy Faithfull foundation is the only UK-wide child protection charity dedicated solely to reducing the risk of children being sexually abused. They work with entire families that have been affected by abuse including: adult male and female sexual abusers; young people with inappropriate sexual behaviours; victims of abuse and other family members.
They provide bespoke training and also specialise in work with offenders. Their focus is on sexual abuse rather than CSE but much of their material is transferrable. www.lucyfaithfull.org
NSPCC: a national organisation with a wide range of information and advice on the web site. This includes ‘Casenotes’ – reports on key issues including links relevant to CSE such as running away and sexual abuse. There is a professional advice section which includes some good resources linked to ‘Young People With Harmful Sexual Behaviour’. www.nspcc.org.uk
National Working Group for Sexually Exploited Children & Young People: The National
Working Group (NWG) is a charity and UK wide network of practitioners, policy makers and researchers working with children and young people who are at risk of, or who experience, sexual exploitation. Their primary aim is to offer support and advice to those working with children and young people affected by sexual exploitation. For more information about the
National Working Group and child sexual exploitation, visit http://www.nationalworkinggroup.org
Resources for working with children (although they may also be useful for
raising awareness in staff teams and with individual workers)
Chelsea’s Choice: a powerful theatre production which is designed to raise awareness of grooming and child sexual exploitation amongst children. The drama is used in group settings and is a 30 minute drama with a 30 minute follow up discussion of the issues raised.
My Dangerous Loverboy: a campaign to raise awareness of internal trafficking of children for the purpose of sexual exploitation. Includes a short video which can be used with
22 CSE Practice Guidance
young people in 1-1 or group settings to get them thinking and talking about what is happening to them. www.mydangerousloverboy.com
The End Of My World – by Emma Jackson. This is a book written by a young woman who experienced abuse through child sexual exploitation. It is a powerful story of the author’s experiences and would be good for professionals to read to raise their awareness and understanding of one model of abuse. It is also suitable for young people to read albeit powerful and explicit in relation to Emma’s abuse. It would be a good book for professionals to read alongside a young person or group and discuss the issues raised.
Professionals would need to use their discretion about the suitability of the content for work with an individual child and are advised to read it themselves to enable them to make that judgement.
3. Resources For Families - these are mainly support services and information.
Life centre: www.lifecentre.uk.com/index.html
Lifecentre is a UK based charity that supports survivors of rape & sexual abuse. It offers a national helpline.
Mosac: MOSAC (Mothers of Sexually Abused Children) is a voluntary organisation supporting all non-abusing parents and carers whose children have been sexually abused.
They provide advocacy, advice and information, befriending, counselling, play therapy and support groups following alleged child sexual abuse. Visit www.mosac.org.uk
for more information or call their national helpline on 0800 980 1958.
NAPAC: is the National Association for People Abused in Childhood. It is a registered charity providing support and information for people abused in childhood. Visit www.napac.org.uk
SURVIVORS UK: provides information, support and counselling for men who have been raped or sexually abused. Thousands of men contact them each year. Visit www.survivorsuk.org
or call their national helpline on 0845 1221201. Helpline hours:
7pm-9.30pm Mon/Tue/Thu.
Parents Protect: General information about protecting children from sexual abuse. Focus largely on intra familial sexual abuse but some useful information on signs of abuse and impact on the child. Parents of young children abused through child sexual exploitation may find some of this material useful. www.parentsprotect.co.uk
23 CSE Practice Guidance
Appendix 1
REQUEST FOR SERVICES FORM
______________________________________________________________
This form is to be used to access services for children at levels 2, 3 and 4 of the Continuum of Need.
-
-
-
-
-
All Referrals must have section A and F completed
To request a Level 2 (Single Agency) service please complete section B
To request co-ordination of level 3 (Multi-Agency) services through
Team Around the Family please complete section C
To Request an additional service for a case which is already in Team
Around the Family please complete section D
To request a service from Social Care please complete section E – CSE concerns must be referred to CADT accompanied by a CSE1 form and completed screening tool
If you require a level 2 or 3 service please email to: gateway@wirral.gcsx.gov.uk
or Fax: 0151 604 3501
It you require a level 4 service please email to: cadtsocialcare@wirral.gcsx.gov.uk
______________________________________________________________
Date of Referral
Section A - Family Details
Address including Postcode
Main Contact Telephone Number
Email Address
Owner/Occupier
Private
Landlord
Housing
Association
Homeless
Children/Young People under 18 living at the above address Please see guidance for completing this
section
First Name Surname
DoB
(dd/mm/yyyy)
M/
F
Age Eth EET School
1 st
Lan g
Disability
Adults living at the above address Please see guidance for completing this section
First Name Surname
DoB
(dd/mm/yyy y)
M/
F
PR/CR
*
Eth* EET
Relationshi p
1 st
Lan g
Disability
24 CSE Practice Guidance
Other relevant people/family members not at the above address Please see guidance for completing this
section
First Name Surname
DoB
(dd/mm/yyyy)
M/F
Address including
postcode
Eth
Relationship
1 st
Lang
Disability
Contact Number
Doctor’s Name:
Dentist’s Name:
Health Visitor’s Name:
School Nurse’s Name:
Are there any potential risks that would affect Staff visiting the home?
Please see guidance for completing this section
Section B – Level 2 Single Agency Services
Service Required In respect to which family member
Please fully describe the need for this service including any specific areas of support E.G
Domestic Abuse, Substance Misuse, Mental Health
What is the primary unmet need for the family? (Please tick one)
Parenting Education/ Work Housing Community
Relationships
School Transfer Family Relationships Money / Finances Health
Section C - level 3 Multi agency / Team Around The Family
Services currently involved with family:
Agency Professional Name In relation to family member
25 CSE Practice Guidance
What is the primary unmet need for the family? (Please tick one)
Parenting Education/ Work Housing Community
Relationships
School Transfer Family Relationships Money/ Finances Health
Please fully describe the need for this service including specific areas of support E.G Domestic Abuse/
Mental Health/ substance misuse)
Does the family agree to a CAF?
Are you the best placed to act as lead professional
Yes No
Yes No
Section D - Cases in Team Around the Family and requiring Additional Service
Name of Lead Professional:
Service Required In respect to which family member
Please fully describe the need for this service including any specific areas E.G Domestic Abuse/
Mental Health/ substance misuse
Section E - Level 4 – Statutory Services
Please advise why you are completing this Request for Services Form:
Child Protection
Concern
Information
Request
Other, please specify in the box below:
Please detail why you are requesting a service from Children’s Social Care:
26 CSE Practice Guidance
Please evidence why this meets the threshold for Social Care intervention:
Please detail any additional services that are already provided or have been attempted:
27 CSE Practice Guidance
Childs Needs
Please comment on each of the following: health, education, emotional and behavioural development, identity, family and social relationships, social presentation and self care skills.
Parenting Capacity
Please comment on each of the following: basic care, ensuring safety, emotional warmth, stimulation, guidance and boundaries and stability.
Family & Environmental Factors
Please comment on each of the following: family history, wider family, housing, employment, income, community integration and community services.
28 CSE Practice Guidance
Section F Consent to Store and Share Information
Information collected in this referral form will need to be shared with agencies identified in the form to help us provide the services you need. If we need to share information with any other organisations later to offer you more help we will ask you about this before we do.
In line with the Data Protection Act (1998) we require your consent to share and store the information in this form.
I/We understand the information that is recorded on this form and that it will be only be stored and shared for the purposes of providing services to me and my family.
I/We have had the reasons for information sharing explained to me and I understand them.
I/We agree to the sharing of information, as agreed, between all relevant services listed in this form.
I/We also agree to the sharing of this and other information, with the relevant services / organisations listed below:
Wirral Council
Your Child / Children’s current school / education provider
Your housing provider
Health Visitor
School Nurse
GP
Adult mental health services
Drug and Alcohol advice and support services
Child and Adolescent Mental Health Services
Other local health services (e.g. A&E, Community services)
Voluntary Services Sector
If you are pregnant or have a child under 5 years:
I/We agree to the sharing of information with our local Children Centre and I understand that we will be contacted by the centre to discuss any support requirements with us.
To consent to sharing information each family member must sign below, or be signed for (if family member(s) are unable to sign for themselves). I understand I may add to or withdraw consent at any time by informing the Key Worker/Lead Professional.
Signed by adult(s) Signature on your file
Signed Name Date Yes No
Date Yes No Signed
Signed by each child
Signed
Name
Name
Signed Name
Name Signed
Signed Name
Please state if consent from all family members has not been obtained e.g. due to being unavailable or objected
Signed on behalf of referring agency / organisation
Print name
Organisation & Position/Role
Contact Tel. Number & email
Date
Date
Date
Date
Date
Signature on your file
Yes No
Yes
Yes
Yes
Yes
No
No
No
No
29 CSE Practice Guidance
Would you be prepared to be lead professional if appropriate? Yes No
Please retain the signed version of this form on file as you may be required to produce it as part of a quality assurance process
Requests for services can only be accepted without consent if it is deemed that to seek parental/carers agreement would place the child at increased risk of significant harm.
(Working Together to Safeguard Children 2013)
30 CSE Practice Guidance
Appendix 2
CSE 1 – Referral Form
This form should be completed by any professional who has concerns that a child/young person may be at risk or is a victim of Child Sexual Exploitation. This form should be returned to CADT with a completed Request for Services form.
E-mail: cadtsocialcare@wirral.gcsx.gov.uk
Fax: 0151 604 3501
REFERRERS DETAILS
Name Date of Referral
Agency Job Title
Email address
YOUNG PERSON’S DETAILS
Forename(s)
Telephone No.
(M/F)
D.O.B Surname/
Family name(s)
Ethnicity Religion
Home address Postcode
Nationality
Home tel no.
GP name
Mob/other contact no.
Surgery
School/ nursery
Relationship to suspect
Medical
Examination
Home tel no.
Y N
LOOKED AFTER HISTORY
Lives with family, no experience of care
Care Leaver Foster family
Lives with extended family, previous experience of care
Residential unit Secure
Accommodation
Section 20 -
Forename(s)
Section 31 – Care
Voluntary Order
PARENT/CARER/GUARDIAN’S DETAILS
Section 38 –
Interim Care Order
(M/F) Parental Y
Unknown
N
Surname/ family name(s)
Responsibility
D.O.B
Ethnicity Religion
Home address Postcode
Nationality
Mob/other contact no.
Occupation
31 CSE Practice Guidance
PARENT/CARER/GUARDIAN’S DETAILS
Forename(s) (M/F) Parental
Responsibility
D.O.B Surname/ family name(s)
Ethnicity Religion
Y N
Nationality
Home address Postcode
Mob/other contact no. Home tel no.
Occupation
SIBLINGS/ADDITIONAL VICTIMS/OTHER PERSONS WITH PARENTAL RESPONSIBILITY
Relationship to young person
Forename(s) (M/F)
Surname/family name(s)
Home address
D.O.B
Home tel no.
Postcode
Mob/other contact no.
Relationship to young person
Forename(s) (M/F)
D.O.B Surname/family name(s)
Home address Postcode
Home tel no. Mob/other contact no.
SUSPECTED PERPETRATOR DETAILS
Forename(s) (M/F)
D.O.B Surname/family name(s)
Home address
Home tel no.
Has suspect previously breached a court order or police bail?
Postcode
Mob/other contact no.
Y N
(If Y provide details below)
32 CSE Practice Guidance
Child suspects only (under 18 years)
School/ occupation
Surname/family name(s)
Forename
Details of person holding parental responsibility:-
Home address Postcode
Home tel no. Mob/other contact no.
CIRCUMSTANCES OF INCIDENT/ANY OTHER INFO
33 CSE Practice Guidance
ASSOCIATES OF CHILD / RELEVANT PARTIES
ASSOCIATES OF SUSPECTED PERPETRATOR / RELEVANT PARTIES
IF MISSING WHO WERE THEY FOUND WITH AND WHERE?
LOCATIONS OF CONCERN WHERE YOU BELIEVE CSE IS AN ISSUE
VEHICLES THAT COULD BE LINKED TO CSE AND TO THE CHILD/YOUNG PERSON
TELEPHONE NUMBERS LINKED TO THE CHILD/YOUNG PERSON/SUSPECTED
PERPETRATOR
PLEASE SEND THIS FORM VIA CADT TO THE MACSE (Multi Agency CSE) MEETING
It is the responsibility of the referring agency to determine whether the referred child’s parents are informed that their child will be discussed at the MACSE meeting.
Clearly best practice would always be to inform / consult with parents regarding their children, but this may be detrimental in some cases. It may not always be in the child’s best interests to inform parents and each case should be considered on its own merits. A referral into Children ’s Specialist Services and the MACSE meetings can be made without informing parents if to do so would place the child at increased risk of serious harm.
34 CSE Practice Guidance
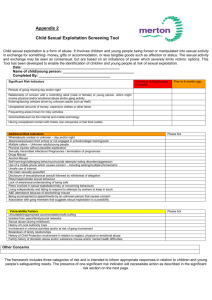
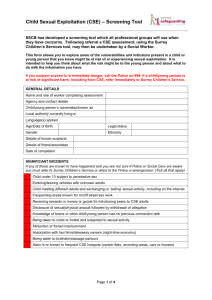
Appendix 3 Catch-22 Screening Tool
CHILD SEXUAL EXPLOITATION SCREENING TOOL
This screening tool should be used by all professionals working with children aged 10+.
Professionals may also decide it is appropriate to use the tool to screen younger children as nationally children as young as 8 years old have been found to be abused in this way. Boys as well as girls are abused through CSE.
This screening tool will help you focus on the specific indicators of sexual exploitation and determine whether further investigations are needed. The tool could be used in supervision, in discussions with parents and carers, with other professionals and with the child.
Many of the indicators of child sexual exploitation are also part of normal teenage behaviours and it is the presence of higher risk factors or multiple other factors which may be indications of child sexual exploitation. Where a child is aged 13 years old or younger the presence of any one high risk factor must be seen as a potential indicator of sexual exploitation.
Professionals need to exercise their own judgement when completing the tool. This includes capturing concerns about which they have some evidence AND concerns based on their “gut feelings”. Staff should differentiate between the two and explain this in the notes section.
Where child sexual exploitation is suspected the worker should discuss their concerns with their manager and should also inform their agency’s lead professional who will be monitoring the bigger picture for any emerging patterns.
Professionals should feel free to use the tool creatively, including as part of awareness raising work with children or in engaging parents and carers in understanding the issues.
It is recommended that a scoring process is applied to enable the level of risk to be quantified.
Where the risk is assessed as low, this qualifies 1 point, where the risk is medium, this qualifies
2 points and where the risk is high, 3 points should be given. At the end of each of the domains, please input the total value of the risk to inform your assessment of comparative domain scores. At the end of the assessment, total up your risk scores to calculate the overall risk rating.
Once completed if it confirms concerns you MUST make a referral to your local CSE
Operational Group or equivalent (using your local area referral form) and should include a copy of the completed screening tool. If the screening tool indentifies High Risk , you must make a referral to Children Social Care using the standard child protection referral process.
35 CSE Practice Guidance
Child’s Name :
Name and job title of person completing:
Dob :
Date completed:
Organisation:
Contact e-mail:
Telephone:
When completing the screening tool you must use your own judgement as factors such as the child’s age, any additional vulnerabilities, their history, etc, may mean that what for another child would be low level, for that child is high level. Workers should feel free to amend the suggested level using that judgement.
You can either indicate the level of risk using High/medium/low or simply tick the box if the risk element is present (you may wish to use more ticks where the risk is higher.
Remember, this tool is to help you make a professional assessment and you should not feel constrained by the format. Record your rationale in the notes boxes.
Health Domain
Physical injuries such as bruising, suggesting of either physical or sexual assault
A sexually transmitted infection (STI), particularly if it is recurring or there are multiple STI’s
Pregnancy and / or seeking an abortion
Present?
Yes/No/Possible. Please comment:
Risk Rating
1=L, 2=M, 3=H
Sexually risky behaviour
Self-harming
Thoughts of or attempted suicide
Eating disorder
Evidence of misuse of drugs / alcohol, including associated health problems
Change in appearance, including losing weight, putting on weight
Learning Disability
TOTAL HEALTH RISK:
Behaviour Domain
Sexually offending behaviour
Truancy/disengagement with education or considerable change in performance at school
Present?
Yes/No/Possible. Please comment:
Risk Rating
1=L, 2=M, 3=H
36 CSE Practice Guidance
Volatile behaviour, exhibiting extreme array of mood swings or abusive language which is unusual for the child
Aggressive or violent, including to pets/animals
Becoming angry/ hostile if any suspicions or concerns about their activities are expressed
Physical aggression towards parents, siblings, pets, teachers or peers
Detachment from age-appropriate activities
Secretive behaviour
Known to be sexually active
Low self-image, low self-esteem
Young offender or anti-social behaviour
Sexualised language
Hostility in relationship with parents / carers and other family members
Getting involved in petty crime such as shoplifting or stealing
TOTAL BEHAVIOUR RISK:
Grooming Domain
Entering or leaving vehicles driven by unknown adults
Excessive use of mobile phones, including receiving calls late at night
Reports that the child/young person has been seen in places known to be used for sexual exploitation
Unexplained relationships with older adults
Associating with other young people who are known to be sexually exploited, including in school
Sexual relationship with a significantly older person
Phone calls, texts or letters from unknown adults
Mobile phone being answered by unknown adult
Inappropriate use of the Internet and forming relationships, particularly with adults, via the Internet. Note: adults may pose as peers to entrap the child
Accounts of social activities with no plausible explanation of the source of necessary funding
Having keys to premises other than those they should have
Possession of money with no plausible explanation
Present?
Yes/No/Possible. Please comment:
Risk Rating
1=L, 2=M, 3=H
37 CSE Practice Guidance
Acquisition of expensive or sexual clothes, mobile phone or other possession without plausible explanation
Having new mobile phone, several mobile phones and/or SIM cards, especially
Blackberry or iPhone (because messages cannot be traced). Always have credit on their mobile phones, despite having no access to money or having no credit so phone can only be used for incoming calls
Recruiting others into sexual exploitation
Seen at public toilets known for cottaging or adult venues (pubs and clubs)
Adults loitering outside the child/young person’s usual place of residence or school
Leaving home/care setting in clothing unusual for the individual child
(inappropriate for age, borrowing clothes from older young people)
Wearing an unusual amount of clothing
(due to hiding more sexualised clothing underneath or hiding their body)
Persistently missing, staying out overnight or returning late with no plausible explanation
Returning after having been missing, looking well cared for in spite of having no known home base
Returning after having been missing looking dirty, dishevelled, tired, hungry, thirsty
Missing for long periods with no known home base and / or homeless
Possession of excessive numbers of condoms
New contacts with people outside of town
Looked After Children Domain
Living in residential care
Frequently missing from placement
Multiple placement breakdown
Going missing with other children
TOTAL GROOMING RISK:
Present?
Yes/No/Possible. Please comment:
TOTAL LOOKED AFTER CHILD RISK:
Risk
Rating
1=L, 2=M,
3=H
38 CSE Practice Guidance
Family and Social Domain Present?
Yes/No/Possible. Please comment:
A family member or known associate working in the adult sex trade
Unsure about their sexual orientation or unable to disclose sexual orientation to their family
History of physical, sexual and/or emotional abuse; neglect
Witness to domestic violence at home
Parental difficulties; drug and alcohol misuse; mental health problems; physical or learning difficulty. Being a young carer
Pattern of street homelessness or sofa surfing
Living in hostel, B&B or Foyer accommodation
Conflict at home around boundaries, including staying out late
Recent bereavement or loss
Gang association either through relatives, peers or intimate relationships
Lacking friends their own age
Living in a gang neighbourhood
E Safety Domain
TOTAL FAMILY AND SOCIAL RISK:
Present?
Yes/No/Possible. Please comment:
Risk
Rating
1=L, 2=M,
3=H
Risk
Rating
1=L, 2=M,
3=H
Evidence of sexual bullying and/or vulnerability through Internet or social networking sites
Concern that inappropriate images of a young person are being circulated via the
Internet/phones
Exchanging inappropriate images for cash, credits or other items
Receiving gifts through the post from someone the young person does not known
Concern that a young person is being coerced to provide sexually explicit images
Concern that a young person is being bribed by someone for their inappropriate online activity
Concern that a young person is selling sexual services via the Internet
Accessing dating agencies via mobile phones (eg 2 flirt line)
39 CSE Practice Guidance
Unexplained increased mobile phone / gaming credits
Going online during the night
Being secretive, using mobile phone for accessing websites, etc, more than computers
Unwilling to share / show online or phone contacts
Concerns that a young person’s online friendship has developed into an offline relationship
Concern that a young person is having an online relationship
Sharing of inappropriate images amongst friends
New contacts with people outside of town
Increased time on webcam, especially if in bedroom
Spending increasing amount of time with online friends and less time with friends from school or neighbourhood
Spending increasing amount of time on social networking sites including
Facebook or on shared gaming sites
TOTAL SAFETY RISK:
What is the level of risk for this child? Why?
High ( 177 - 264)
Medium (89 – 176)
Low (0-88)
In every case where sexual exploitation is a risk factor for a child (high, medium or low) you should refer the child into the MACSE meeting using the referral form and attaching the CSE screening tool.
If professionals are still unsure of the level of risk once the form has been completed please, contact your line manager to talk through the assessment and outcome.
40 CSE Practice Guidance
Appendix 4
Flowchart for Referrals
Concern
Based on warning signs and screening tool
Referral into CADT
Completion of Request for Service form,
CSE screening tool and
CSE 1 Referral form
Forms emailed to cadtsocialcare@wirral.gcsx.gov.uk
Consideration at CADT:
Manager completes CSE2 and sends with CSE1 to
MACSE A.BCU.MFH@merseyside.pnn.police.uk
Decides threshold, if level 4 the case goes through MASH and has network or strategy meeting -record on Liquidlogic
If not level 4 - Step Across Case to Gateway for
Early Help Family CAF assessment or single agency assessment and record on Liquidlogic
Case Managed at Level 4
Social Worker prepares report for MACSE meeting and send report via social care representative
Actions from
MACSE shared with Social
Worker and incorporated into child’s plan.
Case Managed at
Levels 2 or 3
Level 3 - Appropriate agency to be part of
TAF identified at
MACSE
Level 2 – Appropriate agency to receive referral through
Targeted Services identified
Actions recorded and shared by Targeted
Services representative at
MACSE
Consideration at MACSE:
Information sharing requests sent to identified participants
Invitations sent 7 days before meetings
Risk Assessment undertaken
Action plan agreed to reduce risk
Consideration of ongoing cases
Intelligence shared and recorded on Protect system
Ongoing Cases
Cases continue to be considered at
MACSE until multi-agency agreement reached that CSE is no longer a risk
41 CSE Practice Guidance