Bowel Elimination
advertisement

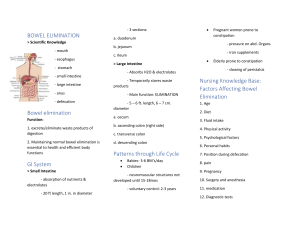
Bowel Elimination NUR101 Fall 2008 Lecture # 23 K. Burger, MSEd, MSN, RN, CNE PPP By: Sharon Niggemeier RN MSN J Borrero 12/08 Functions of the GI Tract • Prepare fluids and nutrients for absorption and use by cells via mechanical and chemical breakdown • Absorb fluids and nutrients • Receives secretions from organs (eg. gallbladder, pancreas) Anatomy & Physiology • Organs of the GI tract? • Function of Large intestine: absorption Extends from Ileocecal valve to anus • Chyme • Peristalsis & Mass peristalsis Act of Defecation • Defecation reflex • Valsalva maneuver • Defecation Alteration in Bowel Elimination • • • • • Diarrhea Constipation Incontinence Fecal Impaction Flatulence Characteristics of Stool • • • • • • Volume Color Odor Consistency Shape Constituents Factors That Influence Bowel Elimination • • • • • • • Age Fluid Intake & Diet Daily Routine Activity Medications Health Status Stress Diet High fiber foods: • Legumes (beans) • Cereals • Whole grains • Raw Fruits • Vegetables Laxative effect foods: • Spicy & greasy • Bran/Chocolate • Coffee/Alcohol • Raw fruits & vegetables Assessing Elimination Status • Usual pattern • Changes in bowels • Aids to eliminate • Current problems Physical Assessment • Inspection- observe contour of abd and note visible peristalsis • Auscultation- listen for bowel sounds all quadrants • Percussion- resonant or tympany over hollow organs…dullness over intestinal obstruction • Palpation- feel for masses, tenderness etc… Stool Specimen Collection • Routine specimen • Occult blood • Ova & parasite • Timed specimens Nursing Dx R/T Bowel Elimination ? Outcome Criteria • Pt. will: • Develop regular pattern of elimination • Have less episodes of incontinence • Incorporate fluids/diet that promote bowel elimination Interventions to Promote Elimination • • • • • • Routine Positioning Privacy Comfort Activity Diet/Fluids Interventions: Promote Bowel Elimination • • • • Laxatives and Cathartics Enemas Suppositories Digital Removal Types of Enemas Types of Enemas Cleansing Retention Return Flow Enema Solutions • Tap water (Hypotonic) • Normal saline (Isotonic) • Soap • Hypertonic • Oil Tap Water (TWE) • • • • Amount: 500-1000cc Action: Distends, increases peristalsis Time: 15 min. Indicated: inflamed bowels/irritated colon • Contraindicated: Atonic bowels, fluid restrictions Normal Saline • • • • Amount: 500-1000cc Action: Distends, increases peristalsis Time: 15 min. Indicated:Inflamed bowels/irritated colon • Contraindicated: Na retention problems, fluid restrictions Soap (SSE) • Amount: 500-1000cc (Castile 5ml/1000cc) • Action: Distends, Irritates • Time: 15 min. • Indicated: Constipation • Contraindicated: Prior to rectal exams Hypertonic • • • • • Amount: 70-130 cc solution Action: Distends/Irritates Time: 5-10 min. Indicated: Constipation, convenience Contraindicated: Dehydration, Na problems Oil Retention • • • • • Amount: 120-200cc Action: Lubricates Time: 30 min. Indicated: Fecal impaction Contraindication: none Enema Administration • PPE • IV pole • Position L Sims • Lubricant • Linen protector • Enema bag with solution • Receptacle (bedpan, commode, toilet) • Tissue paper Enema Administration • • • • • • Position L Sims Insert lubricated tip 4” Bag raised 18-20” above anal canal Administer slowly - 10 min. Administration is individualized. Pt. holds for 15 min. Evaluation • Unusual findings • Solution given blood, • Amount expelled helminthes, pus • Characteristics of etc. stool • Client reaction: • Passing of flatus change in skin color, VS changes, fatigue Medications Effecting Bowel Elimination • Laxatives- induce emptying of GI tract • Antidiarrheal- slow peristalsis, Pepto Bismol, Kaopectate • Codeine/morphine/iron- cause constipation • Antibiotics-may cause diarrhea • Opiates: paragoric, lomotil- habit forming Flatulence Causes: • Decreased peristalsis • Constipation • Medications • Surgery • Diet • Stress • Decreased activity NonInvasive Interventions for Flatulence *Ambulation* • Knee chest position Invasive Interventions for Flatulence • Glycerin Suppository • Harris Flush • Rectal Tube Evaluation of Bowel Function • Achievement of regular defecation habits • Patient’s understanding of normal elimination • Maintenance of adequate food and fluid intake • Regular exercise program • Comfort • Skin integrity Gastrointestinal Charting Chuckles The patient had waffles for breakfast and anorexia for lunch. She stated that she had been constipated for most of her life until 1989, when she got a divorce. Bleeding started in the rectal area and continued all the way to Los Angeles. Rectal examination revealed a normal-size thyroid. The patient was to have a bowel resection. However, he took a job as a stockbroker instead. Fleet enema given with stool hard as pine knots. Patient complains of indigestion since last night when he ate a stake. Patient passed flatus . . . two short, one long. Patient was seen in consultation by the physician, who felt we should sit tight on the abdomen, and I agreed.