Business Imperatives of
Population Health Management
Winter Educational Conference | January 14, 2016
Rob W. York, Senior Vice President
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
Today’s Topics
1. Introduction
2. Physician and Clinical Alignment
3. Contracting Strategy
4. Network Optimization
5. Operational Efficiency
6. Enabling Infrastructure
7. Concluding Comments
8. Q&A/Discussion
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
1
Introduction
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
2
Population Health Management Changes Business Fundamentals
To succeed, executives must rethink:
• The scope of their business(es)
• Where, to whom, and how their organizations provide
services
• Which services are most appropriate
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
3
Five Interrelated Business Imperatives Need to Be Addressed
•
•
•
•
•
Physician and clinical alignment
Contracting strategy
Network optimization
Operational efficiency
Enabling infrastructure
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
4
Physician and Clinical Alignment
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
5
The Emerging Business Model Demands a Higher Degree of
Physician Alignment
• Transformation from volume to value
• An emphasis on coordination of care across the continuum
• Steady and increasing pressure on price
• Unpredictable utilization in medium term
• Improved IT connectivity between hospitals/doctors/patients
• Markets’ increasing preference for scale/essentiality
Physician alignment has always been important,
but in managing population health, it will be essential.
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
6
Integration Models Vary Widely in Their Ability to Impact the
Value Equation
Realizing the
promise of
population health
management
will require the
application of
the most difficult
integration
mechanisms
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
7
A Key Success Factor Is How Incentive Payments Will Be
Distributed
Key Questions:
1. What is the expected overall
financial performance and the
projected incentives?
2. What is the process for
determining the residual incentive
(less costs) that will
be distributed?
3. What is the methodology for
distributing those residual funds to
individual physicians?
| West Virginia HFMA
Best Practices:
1. Align goals with incentives
2. Seek transparency and fairness
3. Establish pools to foster greater
accountability (e.g., PCP, specialist,
ancillaries, acute, outpatient
diagnostics)
4. Develop detailed budgets and
deduct appropriate expenses prior
to determining distributions
5. Continually evolve the approach
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
8
Contracting Strategy
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
9
The Pursuit of Value-Based Initiatives Will Be Critical for LongTerm Sustainability
• Hospitals must: pursue value-based contracting strategies, face
exclusion from key networks, or play the role of a discounted vendor
• Many hospitals will: need to form strategic partnerships to execute
their value-based strategies or prevent network exclusion
Provider organizations able to manage defined populations across the
continuum will be more attractive to payers, employers
and consumers.
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
10
One Size Will Not Fit All – Purchasers Will Use Various
Mechanisms to Achieve Greater Value from Providers
Limited Networks
Wholesale:
“House Money,
House Rules”
Direct
Contract
Service-Level Consumerism
Narrow
Network
High
Deductible
Reference
Price
Centers of
Excellence
Shift Risk to Providers
FFS
P4P
Bundled
Payment
Shared
Savings
Shared
Risk
Full
Risk
Shift to Exchanges
Retail:
Shift Plan Choice
to Consumers
| West Virginia HFMA
Public
Exchange
Private
Exchange
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
11
Moving Across the Continuum of Risk Contracting Will Present
Unique Opportunities and Challenges
• The largest upside (and downside) potential is realized when moving to
the greater acceptance of risk
• Clinical and organizational integration will be a fundamental
requirement for the greater acceptance of financial risk
Small % of financial risk
FFS
IncentiveBased FFS
No risk
• Quality and
cost target
payments
• PQRS
• PCMH
Medium % of financial risk
P4P
• VBP
• Shared
Savings
• Bonuses
• Withholds
Limited Integration
| West Virginia HFMA
Case
Rates
• Episodic
• Bundled
payments
Moderate Integration
Large % of financial risk
Partial
Risk
• Limited
scope
• ACOs
Full
Risk
• Capitation
• PMPM
• Percent of
premium
Health
Plan
• Full
integration
• Health plan
and delivery
system
Full Integration
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
12
Network Optimization
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
13
Developing a High-Performance Delivery Network – Critical Issues
•
•
•
•
•
•
•
Network essentiality (size/scale)
PHM care continuum (breadth/depth)
Service distribution right-sizing
Network performance and outcomes
Overall “network adequacy,” as defined by regulators and/or payers
Delivery network growth strategy
Stakeholder engagement and distribution channels
These criteria and/or critical issues are not mutually exclusive, and each has
nuances that will require thoughtful evaluation.
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
14
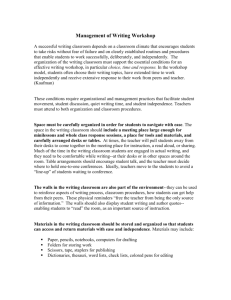
Providers Aiming to Achieve/Ensure Network Essentiality
Attributed Lives vs. CMI Adjusted Cost per Discharge by Network Systems
CMI Adjusted Cost Per Medicare Discharge
$12,000
$11,000
$10,000
System A
$9,000
System B
$8,000
$7,000
System E
$6,000
System C
$5,000
System D
$4,000
0
10,000
20,000
30,000
Membership Attribution
40,000
50,000
Note: Bubble size denotes net patient service revenue.
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
15
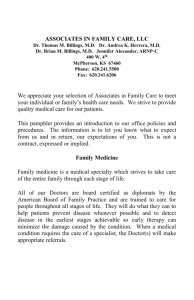
Network Design to Include Continuum of Care
Tertiary/Quaternary
Acute Care
Patient
Acuity
Level
Short-Stay, Psych
Infrastructure and
Ancillary Services
•
Diagnostics
•
Pharmacies
•
Laboratory
•
Therapy
Ambulatory
Specialty Care
Public Health Resources
•
Community Health
Centers
Post-Acute and
Transitional Care
Rehab and SNF
Long-Term Care
Home Care
Hospice/Palliative
Assisted Living
Primary Care
(PCMH)
Longitudinal Care Episode
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
16
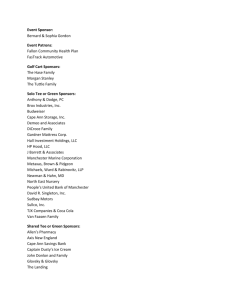
Service Distribution Optimization –
CABG Case Study
CABG Distribution Across the Regional Health System
Statistic
Hosp 1
Hosp 2
Hosp 3
Hosp 4
137
127
126
250
1,297
1,136
1,196
1,886
Length of Stay
9.5
8.9
9.5
7.5
8.6
CMI
6.6
6.5
6.2
6.2
6.3
% Emergent Estimate*
60%
44%
33%
20%
n/a
Internal
Utilization
Discharges
Days
Total
640
5,515
* % Emergent estimated using % treated in the ED for discharges in each hospital’s PSA, Q3 2012 – Q2 2013
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
17
Future Network Growth Requires Appealing to a Variety of
Consumers
Network
Assembly:
Employers
Network
Growth
Network
Selection:
Individual
Enrollment
Provider
Steerage:
Physician
Referral
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
18
Operational Efficiency
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
19
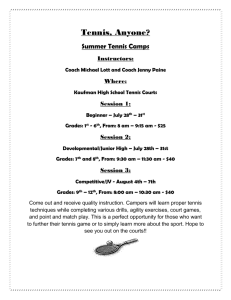
As the Sphere of Influence Widens, Focus Shifts to Total Cost
Management
Population
Health Focus
Traditional
Focus
Mental Health
Prevention
Acute Care
Urgent Care
Emergent
Care
Home Care
Ambulatory
Care
Wellness
Diagnostics
Physician
Clinic
Post-Acute
Care
Chronic Care
Retail
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
20
Reducing Total Cost Demands a New Scope of Initiatives
Hard
Harder
Margin Improvement
Business (Re)Configuration
Hardest
Clinical Effectiveness
Clinical labor productivity
Corporate/market scale
Care processes
Nonclinical labor productivity
Geographic footprint(s)
Clinical variation
Overhead
Service offerings
Care utilization
Supply chain
Service line distribution
Care management
Revenue cycle
Physician alignment and optimization
strategy
Clinical integration
Facility planning/maintenance
New contracting/pricing models
Care transitions
Capital allocation
Consumer and retail strategy
End-of-life care
Nonoperating assets/liabilities
Innovation strategy
Patient education
Corporate risk management
Community investment strategy
Public health and wellness
Required cost focus areas under all business models
Required additional cost focus areas for value based
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
21
A Long-Term Roadmap for Cost Transformation Is Required
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
22
Enabling Infrastructure
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
23
The Enabling PHM Infrastructure Is Critical to Success
• Management/governance structures that include a high level of
physician involvement and cover contracting, risk assessment,
clinical/operational decision making
• Delivery network of sufficient size and scope
• IT systems to support care management, common electronic health
record systems, clinical/predictive analytics, payment
receipt/distribution
• Care management tools and protocols tied to enterprise-wide decision
support and reporting functions
• Contracting and risk assessment and management capabilities,
including actuarial skills if assuming full risk for a population
• Patient engagement programs to build loyalty to the organization
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
24
Overall strategy:
Integration with
broader Healthcare
Company
E XAMPLE
PHM Division Governance and Executive Leadership
PHM Division Operations
Centralized PHM
infrastructure:
Build, buy, and
partner options
PHM delivery hubs:
Physician orgs,
employers,
purchasers, medical
neighborhoods, etc.
1. Care Model Coordination/
Integration
3. Service Delivery and Network
Operations (the Continuum)
5. Financial Risk Management and
Modeling
2. Value-Based and Risk
Contracting/Products
4. PHM Analytics & Info. Systems
6. PHM Innovation, Training, and
Education
Local PHM
Network 1
Primary Engmt.
& Mgmt.
Care
Population
| West Virginia HFMA
Local PHM Network
3+
Local PHM
Network 2
??
Primary Engmt.
& Mgmt.
Care
Population
??
Primary Engmt.
& Mgmt.
Care
??
Population
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
25
Risk Management
•
•
•
Strategic and operational risk
Actuarial or insurance risk
Financial asset and liability risk
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
26
Concluding Comments
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
27
Concluding Comments
• Population health management is a significantly new way of doing
business with broad and complex implications
• The changes span the entire organization
• The benefits — and risks — of managing population health are
proportional to the degree of risk assumed
• Successful population health management requires:
– Strong physician and clinical alignment
– Thoughtfully developed contracting strategy
– Optimization of delivery networks
– Operational efficiency
– Enabling infrastructure
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
28
About the Speaker
Robert W. York
Senior Vice President
Kaufman, Hall & Associates, LLC
5202 Old Orchard Road, Suite N700
Skokie, Illinois 60077
847.441.8780, ext. 129
ryork@kaufmanhall.com
Rob York is a Senior Vice President of Kaufman Hall and leader of the Population Health Management
division in the firm’s Strategy practice. He provides strategic services for a range of healthcare industry
clients, including payers, physician organizations, academic health centers, large healthcare systems,
public/safety-net providers, and community hospitals. Mr. York’s responsibilities focus on developing
strategies to help providers remain relevant and viable in the new healthcare environment. Such
strategies are based on understanding required shifts to the overall healthcare model, rigorous market
landscape and organizational competitive position analysis, attributed population definition,
segmentation and demand analysis, value-based competency and network design requirements, and
strategic partnership evaluation.
Mr. York regularly speaks to boards and at meetings of professional societies, and has published
numerous articles in industry journals, including Health Affairs, Spectrum (a publication of the
American Hospital Association’s Society for Healthcare Strategy and Market Development), and
Strategic Financial Planning (a newsletter from the Healthcare Financial Management Association).
Prior to joining Kaufman Hall, Mr. York was a consultant with KPMG LLP’s West Coast and Midwest
Healthcare Practices. He has an M.B.A. from the University of Notre Dame and a B.S. in Business
Administration with honors from the University of Arizona.
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
29
Qualifications, Assumptions and Limiting Conditions (v.12.08.06):
This Report is not intended for general circulation or publication, nor is it to be used, reproduced, quoted or
distributed for any purpose other than those that may be set forth herein without the prior written consent of
Kaufman, Hall & Associates, LLC (“Kaufman Hall”).
All information, analysis and conclusions contained in this Report are provided “as -is/where-is” and “with all faults
and defects”. Information furnished by others, upon which all or portions of this report are based, is believed to
reliable but has not been verified by Kaufman Hall. No warranty is given as to the accuracy of such information.
Public information and industry and statistical data, including without limitation, data are from sources Kaufman Hall
deems to be reliable; however, neither Kaufman Hall nor any third party sourced make any representation or
warranty to you, whether express or implied, or arising by trade usage, course of dealing, or otherwise. This
disclaimer includes, without limitation, any implied warranties of merchantability or fitness for a particular purpose
(whether in respect of the data or the accuracy, timeliness or completeness of any information or conclusions
contained in or obtained from, through, or in connection with this report), any warranties of non -infringement or
any implied indemnities.
The findings contained in this report may contain predictions based on current data and historical trends. Any such
predictions are subject to inherent risks and uncertainties. In particular, actual results could be impacted by future
events which cannot be predicted or controlled, including, without limitation, changes in business strategies, the
development of future products and services, changes in market and industry conditions, the outcome of
contingencies, changes in management, changes in law or regulations. Kaufman Hall accepts no responsibility for
actual results or future events.
The opinions expressed in this report are valid only for the purpose stated herein and as of the date of this report.
All decisions in connection with the implementation or use of advice or recommendations contained in this report
are the sole responsibility of the client.
In no event will Kaufman Hall or any third party sourced by Kaufman Hall be liable to you for damages of any type
arising out of the delivery or use of this Report or any of the data contained herein, whether known or unknown,
foreseeable or unforeseeable.
| West Virginia HFMA
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.
30
5202 Old Orchard Road, Suite N700, Skokie, Illinois 60077
847.441.8780 phone | 847.965.3511 fax
www.kaufmanhall.com
© 2016 Kaufman, Hall & Associates, LLC. All rights reserved.