Chapter 12: Schizophrenia

Chapter 12: Schizophrenia (Sz)
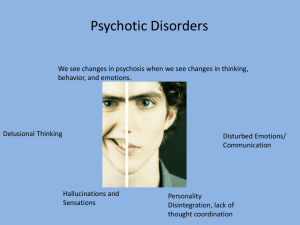
I. Clinical Features
Are there symptoms unique to the disorder, or that define it?
_% of adult Cdn population
Gender differences?
Culture …
Most cases = slower more gradual decline
Stigma
DSM-IV: Diagnostic Criteria for Sz
A.
Characteristic symptoms: 2 or more of the following, each present for a sig period of time during a 1-month period (or less if successfully treated):
1. Delusions
2. Hallucinations
3. Disorganized speech
4. Grossly disorganized or catatonic behaviour
5. Negative symptoms
B.
Social/occupational dysfunction
C.
Duration: Continuous signs of the disturbance must persist for at least 6 months.
D.
Schizoaffective and mood disorder exclusion
E.
Substance/medical exclusion
F.
Relationship to pervasive dvptal disorder: If there is a history of autistic disorder or another pervasive dvptal disorder, the additional diagnosis of Sx is made only if prominent delusions or hallucinations are also present for at least a month (or less if successfully treated)
Related Disorders
1.
Delusional disorder
1 or more non-bizarre delusions, but do NOT have other characteristic schizophrenic symptoms
- functioning is usually not markedly impaired
- behaviour is not obviously unusual apart from delusions
2.
Schizoaffective disorder
Person displays sufficient symptoms for BOTH an affective episode
(depression, mania or mixed) and Sz
3.
Substance-induced psychotic disorder
Prominent hallucinations and delusions that result from the ingestion of a chemical substance
4.
Brief psychotic disorder
Sudden onset of at least 1 prominent psychotic symptom
Duration: 1 day - 1 mo, followed by a full return to premorbid levels of functioning
5.
Schizophreniform disorder
Presence of symptoms similar to those of Sz
Duration: 1 mo - 6 mo
Disturbances of Thought & Speech
A.
Delusions = ____________________________________________________
Several types
- Persecution / Paranoid
- Religious
- Grandiose / Grandeur
- Thought broadcasting
- Thought insertion
- Thought withdrawal
- Somatic delusions - Delusions of reference
- Of being controlled
B.
Thought Disorder
Looseness of associations / derailment
Poverty of speech
Neologisms
Perseveration
Clanging (rhyming …)
2. Attentional Deficiencies
Difficulty filtering out irrelevant distracting stimuli
Hypervigilance
3. Hallucinations = ___________________________________________________
Command hallucinations
Any sensory modality; most common …
4. Emotional Disturbances
Flat affect
–
Do they experience emotion but fail to express them?
________________
Inappropriate affect
5. Catatonia
characterized by:
Stupor
Excitement
Waxy flexibility
Rigidity
Posturing
Echopraxia
Echolalia
6. Other Types of Impairment
avolition
anhedonia
asociality
Positive Symptoms Negative Symptoms
Onset
Intellectual Ability
Response to Medication
Why?
Type I (+) Type II (-)
Subtypes of Schizophrenia …
Paranoid
Disorganized
Catatonic
Undifferentiated
II. Theoretical Perspectives
(A) Genetic Factors
PP who are more closely related to pp with Sz are at increased risk
– if both parents have Sz, child’s chances of Sz : __%
– MZ twins: concordance rate: __%
However, genetic component alone is not sufficient to explain the incidence of Sz
( B) Biochemical Influence
Neurotransmitter: ________________________ …
– Evidence:
•
Neuroleptics
• Amphetamines
(C) Viral Infections
Pre- or post-natal
Viral infections …
Inconclusive
(D) Brain Abnormalities
Ventricle enlargement …
Structural damage --- probably prenatally or early in life …
Brain areas:
•
•
•
Tying it Together
Diathesis-stress model …
Evidence…
–
Stress (e.g., sociocultural factors) predicts initial onset in geneticallyvulnerable pp
–
Gene-environment interactions
• cannabis use may trigger Sz in genetically-vulnerable pp
(cause-effect?)
–
Adoptee studies
–
Longitudinal studies of high-risk children (pp. 450-1)
(E) Family Theories
Early theories: schizophrenogenic mother
2 sources of family stress:
1. Deviant Communications
–
Double-bind communications
–
Vague, disruptive, fragmented; attack ...
2. Expressed Emotion
III. Treatment
Pharmacotherapy
Therapy Based on
Learning Models
Psychosocial
Rehabilitation
Family Therapy
Neuroleptics (antipsychotic agents)
–
Block _______________________
Do not cure Sz
Help some but not all pp with Sz
Do they work better on positive vs negative symptoms?
Do they affect relapse rates?
Produce side-effects , which often lead to noncompliance:
tardive dyskinesia…
Newer medications …
Recommendation: combine w other treatments …
Interventions include:
Selectively reinforcing appropriate behaviour
Token economies
Social skills training
Self-help groups
Multiservice rehab centres