FIRST RESPONDER / EMT
advertisement

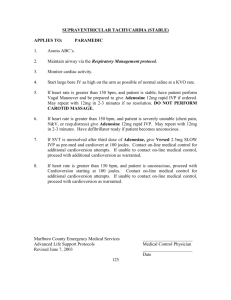
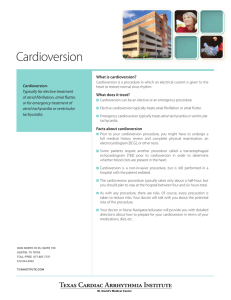
PEDIATRIC TACHYCARDIA WITH POOR PERFUSION See also RED 9-NARROW-COMPLEX TACHYCARDIA (SVT) FIRST RESPONDER / EMT-BASIC 1. Open airway. Consider airway adjunct, if airway not maintainable by head positioning or a towel under the shoulders 2. High flow O2, assist ventilation with bag-mask ventilation and suction as necessary 3. Keep child warm and dry 4. Request ALS if available EMT-BASIC 5. Pulse oximeter PARAMEDIC 6. Advanced airway as indicated 7. Cardiac monitor / IV as indicated 8. Stable patient, no serious signs or symptoms a. Transport b. Vagal maneuvers c. Twelve-lead EKG (ORANGE 5) 9. Unstable patient, serious signs and symptoms. Establish heart rate as cause of serious signs and symptoms d. Twelve-lead EKG (ORANGE 5) e. Evaluate QRS duration QRS DURATION NORMAL FOR AGE: ≤0.08 QRS DURATION WIDE FOR AGE: >0.08 Probable ST Probable SVT Probable VT Hx compatible with Hx incompatible 10. Immediate cardioversion 1 J/kg sinus tach with sinus tach 11. Sedation if possible: diazepam 0.1-0.2 P waves present P wave absent mg/kg IV/IO (max. 4mg), 0.5 mg/kg PR HR varies with HR not variable (max. 10 mg), but do not delay activity/resp with activity/resp cardioversion. Variable RR with Abrupt rate 12. If no change, repeat cardioversion as constant pr changes necessary at 2 J/kg Infants: <220 bpm Infants: >220 13. Lidocaine 1mg/kg IV bolus Children: <180 bpm bpm Children >180 bpm 10. Consider vagal maneuvers (no delay) 11. Cardioversion 1 J/kg. Sedation if possible: diazepam 0.1-0.2 mg/kg IV/IO (max. 4mg), 0.5 mg/kg PR (max. 10mg), but do not delay cardioversion 11. Or Adenosine: if IV/IO access immediately available 0.1 mg/kg (max first dose 6mg) followed by 5cc saline bolus May double dose and repeat twice (maximum dose 12 mg) PINK 9