oral sedation medical history
advertisement

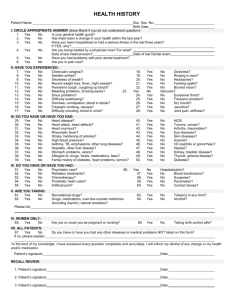
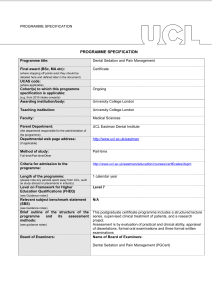
ORAL SEDATION MEDICAL HISTORY Patient’s name:________________________________________________________Date__________________________ Address:______________________________________________________________________________________________ Physician’s Name & Address ___________________________________________________Phone Number_____________ Approximate date of last examination_______________________Patient’s Height_____________Weight______________ 1. Are you currently under medical treatment? Yes____ No____ If yes, please explain________________________________________________________________________ 2. Do you have or have you ever had any of the following? (circle Y for Yes or N for No) a. A heart ailment/prosthetic heart valve b. High/low blood pressure c. Any lung disease d. Diabetes e. Scarlet/rheumatic fever f. Rheumatism or arthritis g. Any blood disease h. Any liver disease or hepatitis i. Any kidney disease j Stomach or intestinal disease Y - N Y Y Y Y Y Y Y Y Y - N N N N N N N N N k. Shortness of breath with limited activity l. Chest pain or angina pectoris m. Asthma n. Stroke o. Sinus problems p. Alcohol or drug dependency q. Artificial joints r. Blood transfusion s. ADD or ADHD t. Hemophilia u. AIDS or HIV Y - N Y Y Y Y Y Y Y Y Y Y - N N N N N N N N N N v. w. x. y. z. aa. bb. cc. dd. ee. Cold sores or fever blisters History of Fen-Phen or Redux Emphysema Heart murmur Tumors or growths Pacemaker Heart attacks Panic attacks Prolonged bleeding following injury or surgery Low bone density/ Osteoporosis medications Y - N Y - N Y Y Y Y Y Y - N N N N N N Y - N Y - N 3.Is there anything of importance in your medical history that has not been asked?_______________________________________ 4.Are you allergic to any known materials?_________________________Latex Allergy?__________________ 5. Have you had any adverse response to drugs such as Penicillin, Aspirin. Codeine?_____________________________________ 6. Are you now taking any drugs or medicines? If so, please list_______________________________________________________ 7. Are you now on any special kind of diet?_______________________________________________________________________ 8. Do you have a history of fainting or convulsions?______________________________________________________________ 9. Radiation treatments or chemotherapy?_____________________________________________________ 10. Is there anything of importance in your medical history that has not been asked?_________If yes, please explain___________ ________________________________________________________________________________________________________ For Women Only: a. Are you now pregnant? If so, when are you due?________________________________________________________________ b. Are you taking birth control pills? ___________________________________________________________________________ c. I understand I should consult my pharmacist if I ever take antibiotics, concerning their effect on birth control. Initials__________ I have read and completed the medical history and I authorize the release of my dental records from my previous dentists, and any future dentists. Patient’s/Parent’s signature: ____________________________________________________ Date:_________________________ Staff signature: _______________________________________________________ Date: _________________________________ Oral sedation medical history 6/10