Health History
advertisement

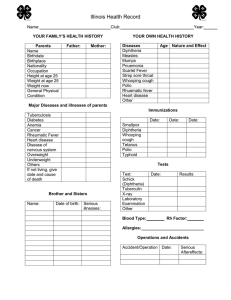
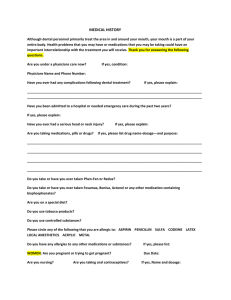
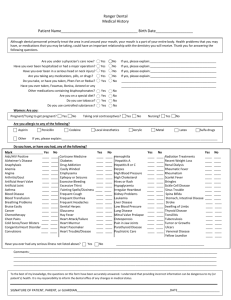
WELCOME TO OUR PRACTICE. AS A NEW PATIENT, PLEASE FILL OUT THE INFORMATION FOUND BELOW TO THE BEST OF YOUR ABILITY. Patient Name: __________________________________ Date: __________________________ Chief Complaint: _______________________________ Birth date: ___________________________ History of present illness: Location: ___________________________________________ Quality: _____________________________ (Where is the pain/problem?) (Ex: normal vs. abnormal color, activity, etc.) Severity: ______________________________________ Duration: ____________________________ (How severe is the pain/problem on a scale of 1-5 with 5 being the most severe) Timing: _______________________________________ (How long have you had this pain/problem Or, when did it start?) Context: ____________________________ (Does the pain/problem occur at a specific time?) (Where were you at the onset of this pain problem?) Associated signs/symptoms: _______________________ Modifying Factors: ___________________ _______________________________________________ ____________________________________ (What other associated problems have you been having?) (What makes the pain/problem worse or better? Or, have you had previous episodes?) Past Medical History Have you ever had the following: Measles Mumps Chicken pox Whooping Cough Scarlet Fever Diphtheria Smallpox Pneumonia Rheumatic Fever Heart Disease Arthritis Venereal Disease Hepatitis Thyroid Disease Any other disease (Please list) (Circle “no” or “yes”, leave blank if uncertain) no yes Anemia no yes Back trouble no yes no yes Bladder Infections no yes High Blood Pressure no yes no yes Epilepsy no yes Low Blood Pressure no yes no yes Migraine Headaches no yes Hemorrhoids no yes no yes Tuberculosis no yes Date of last Chest X-ray _______ no yes Diabetes no yes Asthma no yes no yes Cancer no yes Hives or Eczema no yes no yes Polio no yes AIDS or HIV+ no yes no yes Glaucoma no yes Infectious Mono no yes no yes Hernia no yes Bronchitis no yes no yes Blood or Plasma no yes Mitral Valve Prolapse no yes no yes Transfusions no yes Stroke no yes no yes Ulcer no yes Kidney Disease no yes no yes Bleeding Tendency no yes no yes ______________________________________________________________________________ Previous Hospitalizations/Surgeries/Serious Illnesses When? Hospital/City/State ___________________________________________ _______ ____________________ ___________________________________________ _______ ____________________ ___________________________________________ _______ ____________________ Medications: (Include nonprescription) _____________________________________________________________________________________ _____________________________________________________________________________________ Have you ever taken Phen-Fen/Redux? no yes Patient Social History Marital Status Use of Alcohol Use of Tobacco Use of Drugs Single_____ Never _____ Never _____ Never _____ Married _____ Separated_____ Divorced_____ Widowed______ Rarely ______ Moderate _____ Daily _______ Previously but Quit __________ Type/Frequency ___________________________________________ Family Medical History Father Mother Siblings Spouse Children Age _______ _______ _______ _______ _______ _______ _______ Diseases _________________________ _________________________ _________________________ _________________________ _________________________ _________________________ _________________________ If Deceased, Cause of Death ____________________________ ____________________________ ____________________________ ____________________________ ____________________________ ____________________________ ____________________________ ______ ______ _______________________ _______________________ _________________________ _________________________ HEALTH HISTORY