S McLean R Bruno submission document
advertisement

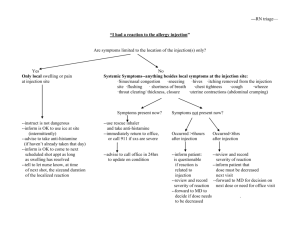
Harm reduction by filtration National Drug Strategy Consultation MDP 27 GPO Box 9848 Canberra ACT 2601 Submission to National Drug Strategy Harm reduction by syringe filters: A cost-effective means of improving the health of injecting drug users Professor Stuart McLean and Dr Raimondo Bruno 5 February 2010 SUMMARY Injecting drug users (IDUs) are liable to suffer harm not only from the illicit drugs themselves, but also from inadvertent injection of unwanted material present in these illicit drugs. This additional material includes insoluble particles and infectious microorganisms, and these are responsible for much of the medical complications associated with injecting illicit drugs: skin and soft tissue infections, endocarditis (infection of heart valves), pulmonary (lung) complications, and impaired blood flow to the limbs, leading to necrosis (tissue death) and amputation. The needle and syringe program (NSP) was introduced in Australia in the 1980s to counter the HIV epidemic, and it has been highly cost-effective in reducing viral infections by HIV and hepatitis C1. Filters are able to remove microorganisms and other particles but they are not uniformly available through NSP sites, and may not be used if available because of problems with the filters blocking and a belief amongst IDUs that some of the drug is lost on the filter. Despite these concerns and limited availability, one-third of frequent IDU in mainland jurisdictions have recently used syringe filters 2, and this rate is significantly greater in Tasmania (45%) where access to filters is subsidised 3. However, one-fifth of IDUs do not use any filters and a further two-fifths use cigarette filters, which are ineffective as they only remove the largest particles 4 5. The problem of particles is particularly severe when IDUs prepare injections from tablets that are designed for oral administration. The tablets are crushed and mixed with water and the mixture is injected. 1 Harm reduction by filtration However, tablets contain a large proportion of inactive ingredients to facilitate the manufacture, storage and therapeutic effect of the drug. Many of these ingredients are not water soluble and their injection can cause complications. The long-acting formulations of morphine sulfate, such as MS Contin®, are commonly used this way. These tablets contain a wax matrix which is used to confer the prolonged effect of morphine. A major problem is that the wax produces a large amount of insoluble particulate material when the tablet is crushed for injection. The prevalence of injection of morphine and other pharmaceutical opiates has increased in recent years, and has been noted as an issue of concern by the Royal Australian College of Physicians [see: http://www.racp.edu.au/index.cfm?objectid=EA87198D-CA47-AB21072D9B2F26FD4AA3] We have studied the particle content of injections prepared from longacting morphine tablets (MS Contin®) 5. Each unfiltered injection contained tens of millions of particles which ranged in size from smaller than 5 m to greater than 400 m. Intravenous injection of these particles is harmful, as they will lodge as emboli in the blood vessels, leading to tissue death. We found that virtually all of the particles can be removed by appropriate filtration, and that effectively the full dose of the drug can be retained by good preparation practices. It is our recommendation that effective filters and instructions on their use should be uniformly provided at NSP outlets. Appropriate syringe filters are able to remove particles and, using the 0.2 m pore size, can also remove microorganisms (bacteria and fungi, although not viruses). Thus with a single additional step, much of the harm caused by injections prepared from pharmaceutical tablets can be eliminated. The use of effective filters would also be expected to reduce the harm caused by injection of illicit drugs other than morphine from tablets, at least so far as this is due to the presence of insoluble particles and non-viral microorganisms. A full cost-benefit evaluation of this intervention has not yet been done. However, since the filters would be supplied through existing NSP outlets the costs of implementation would be not much more than the wholesale price of the filters ($1-2 each). The most common causes of hospital admissions of IDUs, soft-tissue infections and lung complications, can be prevented by effective skin-swabbing and filtration of injections, saving the cost of hospitalization which is $A3,907 per average of all hospital admissions 6. Some idea of the national cost comes from the estimated cost to the public health system of treating injection-related injuries and diseases (excluding HIV and other viral infections) for Victoria, NSW and 2 Harm reduction by filtration Queensland, which was $19 million in 2005/6 7. Usually IDUs only seek treatment for the most serious reactions, and these are greatly outnumbered by potentially serious and non-serious reactions7. Therefore these known health costs represent only a small fraction of the total health impact of injecting drug use. 3 Harm reduction by filtration BACKGROUND Harm due to non-drug contaminants of injections Injecting drug users (IDUs) are liable to suffer harm due to the adverse effects of the drugs, such as respiratory failure after overdose with opiates or psychotic episodes after heavy use of amphetamines 8. However, in addition to these drug-related harms, a great number of medical complications can be attributed to, or are aggravated by, contaminants and other extraneous material in the injections 9-12. Some of these contaminants are deliberately added to illicit drug preparations as diluents (eg quinine, lactose, caffeine, sucrose) and some occur during production (eg chemical byproducts, dirt) 13. In the case of pharmaceutical tablets, various inactive substances are added during production to facilitate the manufacture, stability and therapeutic effectiveness of the tablet 14. The additives, or excipients, include a number of substances which are not soluble in water: talc, cornstarch, cellulose, magnesium stearate, waxes. Whatever their source, the injection of insoluble particles can cause health complications. Effects of injection of particles There are two broad types of problem which arise from the injection of particles. Particles tend to be irritant to tissue (think of dust in the eye), and can cause inflammation at the site of injection. Damage to the vein can lead to inflammation (phlebitis), formation of a clot (thrombus) or both (thrombophlebitis). This can block the flow of blood leading to a lack of oxygen in the downstream tissue (ischaemia). This condition can occur near the site of injection or in a deep vein (deep venous thrombosis or DVT) and is considered to be common amongst IDUs although often untreated12. Sometimes the injection is made into the skin or muscle, either because it misses the vein, or because the vein has been too damaged from previous injections 10 13. The inflammation in these tissues leads to a lump (granuloma) involving accumulation of white blood cells and deposition of scar tissue. This can progress, for example it it becomes infected, leading to an abscess, and chronic skin ulcer 15. The second type of problem occurs when a particle is injected into the bloodstream where it moves downstream until it encounters a vessel too small to pass, where it lodges forming a blockage, or embolism. This results in a lack of blood flow to the downstream tissue (ischaemia) which can lead to death of this tissue (necrosis) 9 16. When injected into a vein in the arm or leg, particles will be carried through ever-larger vessels to the heart, and then to the pulmonary circulation where they will encounter progressively smaller vessels from arteries to arterioles to capillaries 17. Particles larger than capillaries (about 7-9 m, where one 4 Harm reduction by filtration m or micrometer is one thousandth of a millimetre) will block there, while larger particles will block the arterioles (9-40 m diameter) or small arteries (300-400 m diameter). Particles larger than this are unlikely to be taken up through the syringe needle and will not be injected. Sometimes the injection is made into an artery in the arm or leg, either accidentally or deliberately when the veins have become too damaged to access. In this case the embolism and consequent ischaemic damage occurs in the limb and can lead to amputation of digits or the limb itself, depending on the site of the blockage 13 18. Microorganisms, such as bacteria and fungi, are also particles and can be removed by filtration provided the pore size is small enough 19. A filter size of 0.2 m is regarded as sterilizing since it will remove these microorganisms, although it will not remove viruses. Fortunately, the viruses of most concern for IDUs (HIV and hepatitis C) are blood borne and can be avoided by not sharing injection equipment 10. Medical complications of injecting drug use In some cases the drug itself can produce critical illness, for example stroke and myocardial infarction after cocaine injection 8. Many substances have been used to dilute illicit drugs, including quinine, lactose, caffeine, sucrose 13. Although it is water-soluble, quinine is capable of damaging the walls of blood vessels and its injection can cause clotting (thrombosis) in veins 15. However, there are a large number of medical complications of injecting drug use which are attributable, wholly or in part, to particles and microorganisms present in the injection and which could be removed by filtration. The most common complications requiring treatment which are experienced by IDUs are skin and soft tissue infections, and diseases of the heart and lungs (Table 1). These sites have the greatest contact with the injection constituents, either as sites of injection (skin, muscle), or as the first organ of contact in the circulation (heart), or as having the first microcirculation of contact (in the lungs). 5 Harm reduction by filtration Table 1. Selected1 Medical Complications of Injecting Drug Use Tissue Injection into vein Skin and muscle Cellulitis Abscesses Nodules Complication2 Blood vessels and lymphatics Thrombophlebetis Thrombosis Pseudoaneurysm Necrosis Necrotizing ulcers Necrotizing fasciitis Chronic venous insufficiency Lymphoedema Heart Endocarditis Lungs Fibrosis Granuloma Nodules Conglomerate masses Pulmonary hypertension Panacinar emphysema Septic arthritis Osteomyelitis Skeleton Injection into artery Limbs Ischaemia Necrosis Gangrene Amputation Infections Local and systemic infections with Staphylococci, Streptococci, Psudomonas, Clostridium. 1A very large number of complications have been reported, involving almost any body organ 20 2All of these complications have been associated with injection of particles References: 9-11 13 16 21 22 6 Harm reduction by filtration The initial damage may lead to local tissue necrosis which enables pathogenic microorganisms to colonise the tissue, and the resulting infection leads to more serious disease. For example, in the skin, irritation causes a type of inflammation (cellulitis), then a lump of scar tissue (granuloma). The damage can progress to local infection (skin abscess) and, if this should spread to the bloodstream, a serious systemic infection. The microoganisms usually involved are bacteria which are commonly found on the skin (Staphylococcus aureus and Streptococcus species), and infections are associated with a failure to disinfect the injection site 13 15 23, indicating that the IDU has probably become infected by omitting to sterilize their skin 10 15. In the heart, it is the tricuspid valve which has been most commonly infected in IDU-related endocarditis 11 24. The tricuspid is the valve through which the injection constituents pass on the way to the lungs. Here, the major pathogens are Staphylococci, Pseudomonas and the fungus, Candida, all of which are commonly present in the environment 10. The lungs are the primary target organ in which small vessels are blocked following the intravenous injection of particles. This has been well described for talc, which produces characteristic lesions in the lungs 9 16. With repeated injections the talc accumulates in the lungs. The talc can migrate out of the blood vessels into the lung tissue where an inflammatory reaction leads to the development of scar tissue (fibrosis) which takes the form of small lumps or nodules. These nodules can coalesce into larger conglomerate masses. The overall picture is one of progressive damage involving the lung and other chest structures leading to a reduction in lung efficiency (emphysema) and impaired breathing (dyspnoea) and sometimes elevated blood pressure (pulmonary hypertension). The latter carries a high risk of heart failure. Evidence that particles cause complications The most direct evidence that particles cause complications comes from studies of IDUs who used crushed tablets. Talc and other insoluble tablet fillers have been implicated in lung and other thoracic complications 9 16 25-27. The talc deposits could be seen in histological specimens from the lung. Injection of crushed buprenorphine tablets causes many skin conditions: cellulitis, abscess, nodules, necrosis, thrombophlebitis and oedema 13. Crospovidine, an insoluble polymer used in pharmaceutical tablets, has been found as particles in the pulmonary arteries and extravascular foreign body granulomas in the lungs of injecting drug users 28. Deep neck abscesses have been found in injecting Ritalin® users 29. This was related to an inflammatory foreign body reaction to the inactive components in the tablet, followed by superinfection with oral or 7 Harm reduction by filtration skin flora. Injection of buprenorphine tablets has been assocated with puffy hand due to obstruction of the lymph ducts 30. Injection of buprenorphine tablets has also been associated with infective endocarditis and Staph. aureus septicaemia with a high mortality rate of 42% 22. Other illicit drug preparations contain insoluble particles, although the composition of these is not well understood. However, the characteristic track marks seen in regular IDUs are due to the deposition of particles under the skin 10. It is also generally considered among experts that contaminating particles are a major contributing factor to physical complications of drug abuse, especially when microbes are considered 911 13 15 16. Finally, it is biologically plausible that insoluble particles are major contributors to health complications. Unlike insoluble particles, drugs and other substances which are in solution are not usually able to cause blockages in blood vessels or deposit in tissues. Also, despite the exceptions of quinine, and cocaine (which can excessively constrict blood vessels), drugs and inert diluents in solution do not usually cause damage to blood vessels, unlike particles which can physically damage the vessel walls leading to thrombosis or even laceration and ballooning of the wall (pseudoaneurysm) 9. The infection which commonly follows tissue damage is due to non-viral micoorganisms, bacteri and fungi, which are also particles. These infections may be a primary cause of complications 9 13. Infections which commence locally (eg in the skin or a heart valve) can progress to involve the entire body 10 15. Evidence that many infections are due to poor injection technique It is self-evident that exclusion of microorganisms will prevent infection, and this underlies the use of sterile injection procedures in normal medical practice. Several authors have commented that IDU infections are attributable to non-sterile injection procedures 9 10 13 31 32. Vlahaov 23 showed that skin cleaning lowered the incidence of abscesses and endocarditis. Caflisch 19 found that filtration through a sterilizing 0.22 m filter, but not a 20 m filter or cigarette filter, was very effective in removing bacteria from illicit drug injections. In a large Australian study, Dwyer and colleagues 7 12 found that not washing hands was associated with an increased risk of infections amongst IDUs. They recommended hygienic injecting procedures and filtration as important protective measures. 8 Harm reduction by filtration Recent studies show that, despite this evidence, while the majority of IDUs (84%) do clean their injection site prior to injection12, only 14% always wash their hands7 and only 31% have used a filter in the past 12 months2 33. Injections directly into the skin or muscle, which is done when the veins have become too damaged, is another strong risk factor for abscesses 15. Procedures used by IDUs We have surveyed 260 IDUs in the Hobart area to determine the filtering methods they applied on their last occasion of morphine injection 5. This was selected as it was the most common opiate drug injected in Tasmania3, and preparations or morphine have very high levels of particulate contamination. Despite this, the survey revealed that, on their last occasion of morphine injection, one third used no filter, 41% used cigarette filters and 21% used syringe filters5. Smaller numbers used other makeshift filters (cotton balls, tampons, etc) or combinations of filters. BENEFITS OF FILTRATION OF INJECTIONS Particles can be removed by filtration We have recently characterised the particles present in injections prepared from extractions of crushed morphine tablets (MS Contin®), and shown that they can be removed by appropriate filtration 5. The tablets were crushed and mixed with water and filtered using methods based on those employed by IDUs. Appearance of injection mixtures The unfiltered extracts were milky in appearance and had clearly-visible white insoluble material (Figure 1, tube 1). The extract was then passed through various filters used by IDUs. The commonly-used cigarette filter only removed some of the larger particles, and the filtrate had the appearance of diluted milk (Figure 1, tube 2). The small-pore syringe filters (0.45 m and 0.22 m) blocked with the unfiltered injection, but if the unfiltered solution was first passed through a cigarette filter and then the syringe filter, this passed through easily, giving a solution that was clear and bright (Figure 1, tube 3). 9 Harm reduction by filtration Figure 1. Injections prepared from a tablet of morphine (MS Contin®) crushed and mixed with 3 mL water. 1 = unfiltered; 2 = cigarette filtrate; 3 = 0.22 m syringe filtrate. The injection mixtures were then examined under a microscope. The unfiltered extract showed many particles ranging in size from less than 5 m to more than 400 m (Figure 2A). After passage through a cigarette filter there were still a large number of particles, although some of the larger particles had been removed (Figure 2B). When this filtrate was passed through a syringe filter (0.22 or 0.45 m), nearly all of the particles were removed. A small number of particles remained, due to the inevitable environmental contamination (eg by dust) of a working area which is neither sterile nor particle-free, as is used by IDUs. 10 Harm reduction by filtration Figure 2A. Photomicrograph of a sample of the unfiltered injection. Note that there are many particles, with a large range of sizes and that their shapes are highly irregular. Figure 2B. Photomicrograph of a sample of the injection after passage through a cigarette filter. Note that there are still many particles, although fewer of the largest particles. Figure 2C. Photomicrograph of a sample of the injection after passage through a syringe filter (0.45 m). Note that nearly all of the particles have been removed by filtration. The remaining particles are most likely due to normal environmental contamination. 11 Harm reduction by filtration Particle counts per injection The number of particles in each size group was counted in a small sample of each mixture, and used to estimate the number of particles in each injection. The unfiltered injection mixture was densely packed with tens of millions of particles, especially in the range 5 – 50 m (Figure 3, Unfiltered). Although not apparent in Figure 3, there were significant numbers of particles in the largest size group (larger than 400 m) – on average, 12,000 per injection of a single tablet. Although the cigarette filter removed some of the larger particles (larger than 50 m) a large number of particles of all sizes remained (Figure 3, Cigarette Filter). Small-pore syringe filters (0.45 m and 0.22 m) were not very satisfactory with the unfiltered injection, as they tended to block. However, syringe filters were very effective once the solution had first been passed through a cigarette filter: this passed through the syringe filter easily and yielded a solution that was essentially particlefree (Figure 3, 0.22 m Filter). The blockage of these otherwise extremely effective syringe filters without this pre-filtering step is cited by many consumers as one reason that they do not routinely use these devices. The finding that the problem of blocked filters was removed by a simple pre-filtering step is a good example of the importance of the requirement for educating IDU about the most effective use of these filters, rather than solely providing the equipment. Particles in Injections 0 3000 2000 1000 0 Particle size (m) Particle size (m) 5000 4000 3000 2000 1000 0 >4 0 10 0 040 0 50 -9 9 20 -4 9. 9 10 -1 9. 9 59. 9 1000 4000 Particles per injection (thousands) 2000 (7112) 5000 >4 0 10 0 040 0 50 -9 9 20 -4 9. 9 10 -1 9. 9 59. 9 3000 0.22 m Filter Cigarette Filter Particles per injection (thousands) 4000 >4 0 10 0 040 0 50 -9 9 20 -4 9. 9 10 -1 9. 9 59. 9 Particles per injection (thousands) Unfiltered 5000 Particle size (m) Figure 3. Numbers of particles by size in morphine tablet injections. The unfiltered injection mixture was first filtered through a cigarette filter, then through a 0.22 m porosity syringe filter. The numbers are expressed in thousands (that is, 5,000 units = 5 million particles) with mean and SD of 3 replicates. 12 Harm reduction by filtration Recovery of morphine after filtration One reason IDUs do not filter their injections is a belief that some of the dose will be lost in the process. We found that this need not be the case, since by rinsing the filters, the morphine could be recovered without significant loss (Figure 4). ). This is consistent with findings by another research group at the University of Otago 34. Morphine Recovery Morphine recovered (mg) 60 50 40 30 20 10 m er Fi lte r 0. 22 ig .F ilt C U nf ilt er ed 0 Figure 4. Amount of morphine recovered before and after filtration of a 60 mg tablet (mean SD, N = 3). Note that an individual tablet may legally contain between 55 and 65 mg of morphine. Conclusions Our study has shown that the MS Contin® crushed-tablet mixture injected by many IDUs across Australia contain tens of millions of particles in each injection. Such particles, together with microorganisms, are known to be the underlying cause of much of the harm associated with this practice. However, appropriate filtration can remove virtually all of the particles including microorganisms, and would consequently be expected to greatly reduce the harm caused by injecting mixtures from crushed tablets. We have since examined injection mixtures prepared from another pharmaceutical, Oxycontin®, with similar results. By extension, the particle-related harm from injection of other illicit drug preparations could also be reduced by effective filtration methods. Cautions Although what we already know justifies the immediate use of filters to reduce injection-related harm, more studies are required to improve the evidence-base for this practice. There are a large number of filters available, made from different materials and with different porosities. 13 Harm reduction by filtration Sterilizing filters are designed to remove relatively few microorganisms from an essentially clean solution, and the manufacturers caution against their use for heavily contaminated suspensions. Even the coarser filters (larger than 0.45 m) are liable to be damaged if overloaded with particles or if high pressures are used. Thus, we need to investigate the use of particular filters for different illict drug injections to thoroughly evaluate the procedures. The effectiveness in removing microorganisms (bacteria and fungi) should also be confirmed. It is not possible to prepare an injection to pharmaceutical standard without clean facilities, as particles and microorganisms from the environment will contaminate the preparation. The injection of illicit substances will remain inherently dangerous due to the effects of the drugs themselves and filterable (soluble) contaminants. However, the harm associated with unfiltered or ineffectively filtered injections can be greatly reduced by effective filtration. RECOMMENDATIONS 1. Filtration of all injections through 0.22 m filters, together with basic aseptic technique (cleaning of hands, injection sites and equipment), has the potential to dramatically reduce the harm associated with injection of illicit drugs, both diverted pharmaceuticals and illicit drugs such as heroin and methamphetamine. 2. The Needle and Syringe Program should be extended to include 0.22 m sterile syringe filters capable of filtering crushed tablet extracts in a single operation. Filtration through a coarse then a ‘sterilizing’ filter is a simple procedure which could dramatically reduce the harm associated with injecting drug use. This could be done by connecting together two filters of the required porosity, or with a combined two-stage sterile 0.8/0.22 m syringe filter, which are commercially available. 3. The equipment (needles, syringes, swabs, filters) should be available in NSP outlets together with trained staff and educational material to increase the uptake of safer injecting practices by IDUs. 14 Harm reduction by filtration References 1. National Centre in HIV Epidemiology and Clinical Research. Return on investment 2: Evaluating the cost-effectiveness of needle and syringe programs in Australia: University of NSW, 2009. 2. Stafford J, Burns L. Australian Drug Trends 2009: Findings from the Illicit Drug Reporting System. Sydney: National Drug and Alcohol Research Centre, 2010. 3. de Graaff B, Bruno R. Tasmanian Drug Trends 2008: Findings from the Illicit Drug Reporting System (IDRS). Australian Drug Trends Series No. 23. Sydney: National Drug and Alcohol Research Centre, 2009. 4. Scott J. Laboratory study of the effectiveness of filters used by heroin injectors. Journal of Substance Use 2005;10(5):293-301. 5. McLean S, Bruno R, Brandon S, de Graaf B. Effect of filtration on morphine and particle content of injections prepared from slow-release oral morphine tablets. Harm Reduction Journal 2009;6(37). 6. Commonwealth Department of Health and Ageing. Cost Report Round 12 (2007– 2008), 2009. 7. Dwyer R, Power R, Topp L, Maher L, Jauncey M, Conroy A, et al. The IRID Project: an exploratory study of non-viral injecting-related injuries and diseases among Australian injecting drug users. Melbourne: Macfarlane Burnet Institute of Medical Research and Public Health, 2007. 8. Mokhlesi B, Garimella PS, Joffe A, Velho V. Street drug abuse leading to critical illness. Intensive Care Med 2004;30(8):1526-36. 9. Gotway MB, Marder SR, Hanks DK, Leung JWT, Dawn SK, Gean AD, et al. Thoracic complications of illicit drug use: An organ system approach. Radiographics 2002;22:S119-S135. 10. Cherubin CE, Sapira JD. The medical complications of drug addiction and the medical assessment of the intravenous drug user: 25 years later. Ann Intern Med 1993;119(10):1017-28. 11. Chiang W, Goldfrank L. The medical complications of drug abuse. Med J Aust 1990;152(2):83-8. 12. Dwyer R, Topp L, Maher L, Power R, Hellard M, Walsh N, et al. Prevalences and correlates of non-viral injecting-related injuries and diseases in a convenience sample of Australian injecting drug users. Drug and Alcohol Dependence 2009;100(1-2):9-16. 13. del Giudice P. Cutaneous complications of intravenous drug abuse. British Journal of Dermatology 2004;150(1):1-10. 14. Sinko PJ. Martin's Physical Pharmacy and Pharmaceutical Sciences. 5 ed. Baltimore: Lippincott Williams & Wilkins, 2006. 15. Ebright JR, Pieper B. Skin and soft tissue infections in injection drug users. Infect Dis Clin North Am 2002;16(3):697-712. 16. Roberts WC. Pulmonary talc granulomas, pulmonary fibrosis, and pulmonary hypertension resulting from intravenous injection of talc-containing drugs intended for oral use. Proc (Bayl Univ Med Cent) 2002;15(3):260-1. 15 Harm reduction by filtration 17. Seeley RR, Stephens TD, Tate P. Anatomy and Physiology. 7 ed. New York: McGraw Hill 2006. 18. Loo HW, Yam AKT, Tan TC, Peng YP, Teoh LC. Severe upper limb complications from parenteral abuse of Subutex (R). Annals Academy of Medicine Singapore 2005;34(9):575-578. 19. Caflisch C, Wang J, Zbinden R. The role of syringe filters in harm reduction among injection drug users. American Journal of Public Health 1999;89(8):1252-1254. 20. Hagan IG, Burney K. Radiology of recreational drug abuse. Radiographics 2007;27(4):919-U10. 21. Beeching NJ, Crowcroft NS. Tetanus in injecting drug users. Bmj 2005;330(7485):208-9. 22. Chong E, Poh KK, Shen L, Yeh IB, Chai P. Infective endocarditis secondary to intravenous Subutex abuse. Singapore Medical Journal 2009;50(1):34-42. 23. Vlahov D, Sullivan M, Astemborski J, Nelson KE. BACTERIAL-INFECTIONS AND SKIN CLEANING PRIOR TO INJECTION AMONG INTRAVENOUS-DRUG-USERS. Public Health Reports 1992;107(5):595-598. 24. Brown PD, Levine DP. Infective endocarditis in the injection drug user. Infectious Disease Clinics of North America 2002;16(3):645-+. 25. Ward S, Heyneman LE, Reittner P, Kazerooni EA, Godwin JD, Muller NL. Talcosis associated with IV abuse of oral medications: CT findings. American Journal of Roentgenology 2000;174(3):789-793. 26. Wong LC, Chang H, Su JM, Wu TC, Tseng CH. Pulmonary granulomatosis associated with insoluble fillers in a heroin addict. Journal of the Formosan Medical Association 2003;102(3):198-201. 27. Hammar SP, Williams MG, Dodson RF. Pulmonary granulomatous vasculitis induced by insoluble particulates: A case report. Ultrastructural Pathology 2003;27(6):439-449. 28. Ganesan S, Felo J, Saldana M, Kalasinsky VF, Lewin-Smith MR, Tomashefski JF. Embolized crospovidone (poly N-vinyl-2-pyrrolidone ) in the lungs of intravenous drug users. Modern Pathology 2003;16(4):286-292. 29. Zemplenyi J, Colman MF. Deep neck abscesses secondary to methylphenidate (Ritalin) abuse. Head Neck Surg 1984;6(4):858-60. 30. Simonnet N, Marcantoni N, Simonnet L, Griffon C, Chakfe N, Wertheimer J, et al. Puffy hand in long-term intravenous drug users. Journal Des Maladies Vasculaires 2004;29(4):201-204. 31. Palepu A, Tyndall MW, Leon H, Muller J, O'Shaughnessy MV, Schechter MT, et al. Hospital utilization and costs in a cohort of injection drug users. Canadian Medical Association Journal 2001;165(4):415-420. 32. Salmon AM, Dwyer R, Jauncey M, van Beek I, Topp L, Maher L. Injecting-related injury and disease among clients of a supervised injecting facility. Drug and Alcohol Dependence 2009;101(1-2):132-136. 33. Varga LM, Chitworth DD, Fernandez MI. Research note: Factors associated with skin cleaning prior to injection among drug users. Journal of Drug Issues 2006;36(4):1015-1029. 16 Harm reduction by filtration 34. Fawcett P, Farquhar S, Green J, Kennedy M, Kershaw M, Salehi F, et al. Do Wheel Filters Retain Drugs During Preparation For Intravenous Injection? Report to Needle Exchange New Zealand. Dunedin: University of Otago, 2010. 17